Stream 1 - Introduction
d2: John Snow's Publications - Group 2  (# 16-30)
(# 16-30)
 Return to John Snow Publications
Return to John Snow Publications
16. "Alkalescent urine and phosphatic calculi"
Source: Snow, John. London Medical Gazette 38, 20 November 1846, pp. 877-880.
Read at the Westminster Medical Society on November 6, 1846.
By John Snow, M.D.
Lecturer in Forensic Medicine at the Medical School, Aldersgate Street.
(Read at the Westminster Medical Society Nov. 7, 1846.)
Case in which a small quantity of urine remaining constantly in the bladder caused the decomposition of all that was secreted--experiments to show that a very small quantity will have this effect--the bladder cannot be completely emptied of urine when it contains a foreign body: this is the reason why it becomes incrusted with the phosphates, and why these salts form the chief part of so many calculi--cause of alkalescent urine in injuries of the spine, extreme old age, etc.--necessity of injecting the bladder with warm water in most cases of alkaline urine--benefit to be expected from this practice in stone in the bladder.
In a state of health the urine is generally slightly acid; it may, however, be for a short time neutral, or slightly alkaline, from articles of food or drink which contain potash or soda in combination with a vegetable acid--as apples, pears, grapes, etc., and saline draughts made with the citrates, tartrates, or acetates; the vegetable acid is digested, and the alkali passes into the urine. This condition of the secretion, however, is but temporary, and when the urine is strongly alkaline, or remains alkaline for days together, this must be looked on as a departure from the physiological condition.
When healthy urine is allowed to remain in a vessel, it is well known that it becomes alkalescent from decomposition; the urea it contains becoming changed into carbonate of ammonia. In paralysis of the bladder, when it remains constantly distended, and the urine dribbles away to make room for what is secreted, it is known to become offensive and ammoniacal. The same change of the urine takes place also in some cases of paraplegia, of enlarged prostate, and of stricture, when the bladder remains full for some time.
In the latter part of 1842, I had a patient suffering from incontinence of urine after a very tedious labour: when was applied to about the circumstance, I found the urine very ammoniacal, and containing a good deal of phosphate of lime in a state like mortar, the patient suffering much from excoriation of the genital organs. On introducing a catheter I found that about a table-spoonful of urine remained constantly in the bladder. After this viscus had been injected with warm water, the urine which flowed all the remainder of the day was free from alkalescence, and tolerably healthy. Here was a case, then, in which the continuance of about half an ounce of urine in the bladder caused the decomposition of all that passed through it. In order to see the bearing of this circumstance on a number of cases in which the bladder cannot be completely emptied, including, as I shall presently show, stone in the bladder, it became desirable to ascertain if a still smaller quantity remaining in that organ might not have a similar effect. With this view I performed experiments in the following manner. About half a pint of newly-voided urine was put into a glass vessel which terminated at the lower part in a tube of minute calibre, through which it dropped into a glass jar below, at the rate of about twelve drops in a minute, which is about an ounce and a half in an hour, that being not far from the quantity usually passing into the bladder from the ureters. The vessels were kept near the fire at the temperature of 100°. At the end of six or eight hours, when the urine had all dropped into the lower vessel, it was emptied, all but about thirty drops, and the upper glass, which served as a funnel, again replenished. It was found that the urine in the lower vessel became decomposed generally in about twenty-four hours--in about the same time, in short, as urine preserved at the same temperature from the beginning of the experiment, the time varying according to the quality of the urine. It generally became quite fœtid in two or three days, at all events highly alkalescent, and remained so as long as the experiment was continued, always fresh and acid in the upper vessel, provided it was washed out occasionally, and always decomposed in the lower one, although the urine, except a small fraction of it, was of the same age in both.
It is well known that an alkalescent state of the urine, and a deposition of the phosphates, usually coexist. The decomposition of urine, whether it takes place in or out of the bladder, is accompanied by the precipitation of the earthy phosphates. The ammonia resulting from the decomposition of the urea and animal matter of the urine combines with the phosphate of magnesia naturally present in solution to form the insoluble triple phosphate; it also combines with part of the phosphoric acid, which holds the lime in solution as a superphosphate, leaving a neutral phosphate of lime, which is insoluble. I have observed that minute crystals of triple phosphate very often begin to appear, as a delicate cloud, in urine that is kept before it has lost the property of reddening litmus. This observation I consider of importance, as it shews that the presence of these minute crystals in acid urine at the moment it is voided does not necessarily depend on an excess of phosphates. When the decomposition of the urine takes place to any great extent in the bladder, so that it becomes strongly ammoniacal, it irritates the mucous membrane, and causes it to secrete a quantity of phosphate of lime, or of phosphate and carbonate of lime, mixed with the mucus; this comes away with the urine, if there is no calculus or other foreign body in the bladder to which it may adhere. In the case of incontinence of urine to which I have alluded, the mucous membrane of the upper part of the vagina also secreted a quantity of phosphate of lime, apparently from the irritation of ammoniacal urine coming in contact with it. Dr. Chowne examined this patient with me.
When there is nothing to interfere with the healthy function of the bladder, it completely empties itself at intervals of a few hours by a vigorous contraction; and if we examine into the various circumstances which may prevent the complete emptying of the bladder, we shall find that they are all liable to be followed by an alkalescent state of the urine and deposit of phosphates. We will take, first, the instances of foreign bodies in the bladder. One of the symptoms of their presence is the occasional sudden stoppage of the stream of urine before the bladder is emptied; in addition to this, it is evident that the bladder can seldom contract around a foreign body so exactly as completely to expel all the urine; and moreover, calculi and nearly all other foreign bodies which gain admittance to the bladder, are porous, and contain urine imprisoned in their pores; accordingly it is a general law, with extremely few exceptions, that foreign bodies in the bladder become incrusted with the earthy phosphates. The usual explanation of this phenomenon, in which Dr. Prout, Sir B. Brodie, and others, agree, is that the foreign body causes chronic inflammation of the bladder, accompanied with a secretion of alkaline mucus which decomposes the urine: but a pea, or a bit of fibrine, or any other substance not of a nature to cause even irritation, is as certain to form the nucleus of a phosphatic calculus as the most hard and angular; and in most recorded cases there has been a total absence of symptoms of chronic inflammation at the time a foreign body was becoming incrusted; consequently, whilst I am ready to admit that the usual explanation may be true in some cases, and may act as a secondary or an auxiliary cause in others, there can be no doubt that the explanation now given is the correct one for most instances, as it shews a physical cause which can scarcely fail to be in operation. Vesical calculi are themselves foreign bodies, and consequently we find that every calculus, whatsoever its nature, is liable to become incrusted with the earthy phosphates; even the strongly acid state of the urine which usually prevails where there is uric acid calculus being generally overcome; whilst, on the other hand, the phosphatic incrustation is scarcely ever covered with any other deposit, but goes on increasing, the phosphatic deposition, when once it has commenced, being a cause of its own continuance. Mr. Taylor only alludes, in the Catalogue of the Calculi in the College of Surgeons, to two phosphatic calculi which became covered by another deposit, one in the museum of the College, in which the secondary deposit is oxalate of lime, and the other in the museum of St. Bartholomew's Hospital, in which it is uric acid.
When a catheter is introduced, if the bladder is not paralysed, it will contract as the urine flows, and be completely emptied, or nearly so; but if the catheter is left in the bladder, this viscus does not of course continue constantly in a state of active contraction, but is collapsed, and no doubt allows a small quantity of urine to remain in it, more or less, according to the position of the patient and the catheter: consequently we find that a catheter can seldom be left for two or three days in the bladder without inducing an alkalescent state of the urine, and becoming incrusted with the phosphates.
Dr. Prout, Sir B. Brodie, and numerous observers since, have remarked that injuries of the spine are liable to be followed by alkaline urine. This has usually been thought to depend on an altered secretion by the kidneys, arising from impaired nervous influence; it has been found, however, in various cases of disease and injury of the spine, that the urine, although alkaline in the bladder is acid when first secreted by the kidneys. Dr. Golding Bird (Med. Gaz. vol. xxxii, page 10; Urinary Deposits, 2d edition, p. 222.) accounts for this change by supposing that the healthy bladder preserves its contents from decomposition by its vital endowments, and that this property of the bladder is impaired by injuries and other affections of the spine; and Mr. Curling (Ibid. [that is, Med. Gaz.] vol. xiii, p. 76.) supposes that, when the bladder loses its sensibility from spinal lesion, it begins to secrete unhealthy alkaline mucus, which decomposes the urine. Now I have observed that healthy urine will keep fresh out of the body at blood-heat as long as it ever remains fresh in the bladder; and, with respect to the change in the mucus, there is every reason to believe that in these cases it is the consequence, and not the cause, of the alkalescence of the urine. Since the experiments I have related, we are in a position to give a more satisfactory explanation, and one which fortunately suggests a remedy of easy application. The explanation is, that the detrusor urinæ, like other muscles, is liable to various degrees of loss of power, besides total paralysis; and that, when it is weakened, along with the other muscles, by injury or disease of the spine, it can empty the bladder in a great measure, but cannot contract in that vigorous and complete manner necessary to expel the last drops of urine; and that thus a source of the decomposition exists. It is not improbable that, when the bladder is long occupied by highly alkalescent urine, the decomposition may be propagated in course of time in a retrograde manner along the ureters to the kidneys, and ultimately destroy the patient. This seems the best solution of certain cases in which phosphatic calculous matter is found in the pelvis of the kidney after death in persons who have suffered from injury or disease of the spine.
Dr. Prout (Stomach and Urinary Diseases.) has taught us that a state of great nervous irritability and depression is characteristic of the phosphatic diathesis, and leads to the secretion of alkaline urine by the kidneys. Now I have observed that an alkalescent state of the urine kept up by a local cause in the bladder leads to great depression and debility; and it is not improbable that general nervous and muscular debility may be a cause of alkaline urine by preventing the proper emptying of the bladder: consequently, whilst I do not dispute the existence of the phosphatic diathesis in the proper sense of the term--viz. the secretion of the phosphates in excess by the kidneys--I am inclined to believe it rare. The urine is often alkalescent in the decrepitude of extreme old age. We can now perceive the reason, since the muscular tunic of the bladder must of course partake of the debility common all the voluntary muscles.
Simon, of Berlin, has noticed an alkaline state of the urine in typhus, generally when comatose symptoms are setting in. Now, since sensation and volition, as regards the bladder, are often totally lost in typhus, it is almost certain that this organ must frequently suffer a partial loss of function, when, although still able to void the urine, it will not expel it completely. Under these circumstances the urine ought to be alkalescent in the bladder, and continue so till during convalescence the patient is able to empty the bladder properly.
The indications of treatment arising from these views of the subject are obviously to do for the bladder what it is incapacitated for doing of itself: to remove that little leaven of decomposition which alters the whole of the urine as fast as it flows into the bladder. The way to do this is to introduce a catheter, and inject warm water, to wash the bladder thoroughly out. The operation of injecting the bladder is, I believe, but little practised except in some states of disease of its mucous membrane; but I have no doubt it will be found the most efficacious treatment in nearly all cases of alkalescent urine. Mineral acids may be a very useful adjunct to this practice, but hitherto they have been far from successful in what has been called the phosphatic diathesis; and it is not to be expected that any quantity of acid, which can safely enter the circulation, and be separated by the kidneys, will be able to counteract such a powerful cause of phosphatic urine as I have pointed out. In the case of incontinence of urine to which I have alluded, the injection of the bladder, by removing the ammoniacal state of the urine, at once relieved the greater part of the patient's sufferings, and its repetition every day for a few weeks, until the bladder began to regain the power of retaining and expelling its contents, preserved the urine in a pretty healthy condition, and no doubt prevented inflammation, thickening, and contraction of he bladder, and perhaps spreading of disease to the kidneys. We may expect, at least, as much benefit in injuries of the spine, and numerous other cases; we may hope to prevent the formation of phosphatic calculi in many instances, and may reasonably expect to have a much greater power over vesical calculi of every kind than we have hitherto possessed without a serious operation. We may hope not merely to prevent their enlargement, but to get them to dissolve. Dr. Prout is of opinion--and there is every reason to believe it is a sound one--that healthy urine is the best solvent of all kinds of calculi which we can hope to possess; and washing out the bladder occasionally will undoubtedly be a great means of keeping the urine in a healthy state in cases of stone. The effect of injecting the bladder every day, or every other day, will be at once extremely beneficial on phosphatic calculi if the kidneys are secreting acid urine, as in most instances there is reason to believe they [880/881] are; and the great difficulty in the treatment of uric acid calculi has always been, the danger of inducing an alkaline state of the urine, which we should be unable to remove, and of thus causing the stone to increase, by a deposition of phosphates, faster than it has increased before: but, since we know how easily such a condition can be removed under the circumstances, we can give Vichy water, citrate of potash, and other appropriate remedies for excess of uric acid, without fear.
54, Frith Street, Soho Square.
Nov. 9, 1846.
Return to John Snow Publications
17. "Case of strangulation of the ileum in an aperture of the mesentery"
Source: Snow, John. London Med. Gazette 38, 18 December 1846, pp. 1049-1052.
By John Snow, M.D., (Read at the Royal Med. and Chir. Society, June 23d, 1846).
The subject of the following case was the patient of Mr. Marshall of Greek Street, and I am indebted to him for the following account of her illness, having seen her during life myself only at his last visit.
Mrs. Oliver, 24 years of age, of good constitution, in the 8th month of her first pregnancy, was seized early on Saturday morning, March 21st, 1846, with rather severe pain, extending over the whole of the belly, of an intermitting character, being increased at intervals varying from a quarter of an hour to half an hour. There were sickness and vomiting, but little or no tenderness on pressure of the abdomen. The pulse was about 80: the bowels had been moved by castor oil. She thought her labour was coming on, but the os uteri was not at all dilated. Supposing that the pain depended on irregular spasmodic action of the intestines, a grain and a half of opium, and a carminative mixture, were administered. In the evening the pain had somewhat abated, and the vomiting had nearly ceased.
22d.--She had slept very little during the night; the pain was as severe as on the previous morning, with shorter intervals of intermission, and the vomiting had returned. Opiates were continued at intervals, and effervescing and cathartic draughts. In the evening the breathing was accelerated, and the pulse was upwards of 100: there was slight distension of the bowels from flatulence. An enema was administered, and was followed by what the nurse considered to be a copious and healthy motion, but it was not seen by me. She now complained of thirst.
23d.--She had passed another restless night. The pulse was now 120, and full;the breathing extremely hurried, and the thirst very great. The countenance was anxious. Sixteen ounces of blood were abstracted from the arm, to the great relief of the dyspnia; the pulse was not diminished in frequency. To take calomel and opium, and effervescing draughts. The clyster was repeated, but no fecal evacuation followed.
24th.--The vomiting continued, and during the night a considerable quantity of dark green liquid was brought up; not, however, having a fecal odour. There was a little tenderness on firm pressure, and great tympanitic swelling of the abdomen. The countenance was somewhat improved since yesterday, but the pulse was very rapid--140. A repetition of the clyster, and a continuance of the calomel and opium, and the fomentations which had been employed throughout, were directed. She died four hours after this visit, on the 4th day of her illness.
Examination 24 hours after death.--The abdomen was tympanitic and very much swollen, and a great quantity of dark green liquid, similar to that which had been vomited, had flowed out. The stomach and small intestines were extremely distended with flatus; the only lymph observed was a little of a creamy consistence between two folds of small intestine in the center of the abdomen; this part of the intestine exhibited a reddish surface externally: the rest of the intestines were nearly of the natural pale colour, except the last portion of the ileum, about 18 inches of which were of a deep purple, approaching nearly to black, and lay in folds in front and to the right side of the ascending colon. The contents of the uterus being removed in order to bring this part more clearly into view, these folds of ileum were seen to be bound down hust in front of the junction of the cecum with the colon, and constricted as closely as if a thread had been twitched tightly round them. The band which held them down did not seem thicker than the smallest hempen twine; one end of it was continuous with the peritoneum covering the vermiform appendix at about three-fourths of an inch from its commencement, and the other with [1049/1050] the peritoneum covering the ileum, about an inch from its termination. The appendix vermiformis was doubled on itself at the junction of this band, and the process of peritoneum inclosing it was dragged upwards, so as to give the appearance of a tight ligament, extending from that point to the upper edge of the pelvis, in front of the right sacro-iliac symphysis. On Mr. Marshall's attempting to pass his finger under the band, it gave way, and liberated the strangulated ileum, but the parts still remained in an unnatural position; the ascending colon was twisted on itself, so that the cecum was turned with its inner edge outwards, the ileum entering on the outerside, and the origin of the vermiform appendix being on the anterior and external side; these intestines, however, were readily removed into their natural places. The coats of the dark-coloured portion of ileum which had been strangulated were much swollen from the great congestion. The stomach was pale externally; its mucous membrane was ashy brown, and gave way under the fingers. This viscus, and the duodenum, contained dark green fluid, and the jejunum and the ileum, down to the strictured portion, contained a good deal of yellow liquid feces; the colon was empty. The head of the fetus was closely fitted to the cavity of the pelvis, and the os uteri was dilated to the size of a half-penny, the membranes being unruptured.
On examining the preparation* (*now in the possession of Mr. Marshall) which accompanies this paper, it will be found that the vermiform appendix is enclosed within a double layer of peritoneum, which forms a kind of broad ligament, which is attached above to the cecum and ilium, and was attached externally and inferiorly to the iliac fossa and brim of the pelvis.
The hand could be passed behind this expansion. On the external side of the vermiform appendix there is an aperture in this membrane, with defined edges, through which the thumb can be passed, and behind the portion of it which extends with a curve from the vermiform appendix to the ileum, there is a pouch into which a finger can be passed for about two [1050/1051] inches. The thin membrane passing from the appendix vermiformis ceci to the ileum, and leaving the aperture through which the strangulation took place, forms an extension of the above-mentioned curve. It has been tied at the spot where it was broken.
The symptoms in this case were such as usually arise from any mechanical obstruction in the bowels. There was nothing to indicate the cause, or even the situation, of the obstruction; for there was not more pain at one part of the abdomen than another. The enlargement of the uterus, by displacing the small intestines upwards and to each side, was probably the immediate cause of the insinuation of the ileum through the aperture. This opinion is confirmed by the circumstance that, in the first of the two cases quoted at the end of this paper, in which the band causing the strangulation was, in size and situation, very much like the one in this case, the immediate cause of the strangulation was evidently a particular posture of the patient. The twisted state of the ascending colon was, no doubt, a consequence of the strangulation, or of the distenstion which followed it: a twisted state of the bowels has been met with in several cases of intussusception and strangulation by membranous bands. There are many cases on record of strangulation of the bowels in an aperture made by morbid adhesion of the vermiform appendix of the cecum with neighbouring parts; but the appearance of the membrane in this case, the absence of evidences of old inflammation in the abdomen, and the circumstance that the membranous band appears to be a natural continuation of a larger fold, lead me to consider it as a congenital production of peritoneum, leaving an aperture on the inner side of the appendix vermiformis similar to the one we see on its outer side.
The recorded cases which I have been able to find that most resemble this just detailed, follow as an appendix, but the authors do not offer any opinion as to whether the apertures were congenital or not: there is, however, one case of strangulation from a congenital malformation related by M. Moscati, p. 468, of the 3d vol. of the same Memoires. In that case the ileum gave off a branch 2.5 feet previous to its termination, in the form of a funnel, terminating in a ligamentous band about 5 inches in length, and attached by its other extremity to the mesentery, leaving an opening through which some loops of the ileum became strangulated. This branch, I conclude, was the remains of the ductus omphalo-mesentericus.
Mr. Thomas Morton and Mr. Prescot Hewett have informed me that they have seen the appendix vermiformis enclosed in a fold of peritoneum forming a kind of broad ligament.
I subjoin two cases translated from the Memoires de l'Academie Royale de Chirurgie:-
"M. de la Faye informed us in 1750 of a strangulation of the intestine by a similar band. Being invited to assist at the opening of a body in order to make a report in concert with the surgeon in attendance, he learned that the subject, who was newly married, had experienced on the night of his nuptials a very severe pain of colic, such as had occurred to him for the last seven years every time that he had lain with a women. On this occasion it was more violent than before, and followed by all the symptoms which accompany a volvulus. The patient died in thirty-six hours, notwithstanding all the assistance that could be rendered him in that short interval. The belly was swelled out like a balloon: on its being opened the cause of death was evident. On going over the intestines with care, there was remarked, at an inch from the termination of the ileum in the cecum, a band of the thickness of a strong thread, and of three finger-breaths in length, attached on one side to the appendix ceci, and on the other to the part of the mesentery nearest to that intestine. The ileum had passed under that band to the extent of a foot: the strangulated portion was collapsed and inflamed. From the stomach to the seat of strangulation the intestinal canal was very much distended, and the part beyond the stricture was in the ordinary state. The band must have been vascular, for it was black and already gangrenous, so that it required only the slightest effort to break it. If the patient could have lived till the rupture of this band had taken place, he might possibly have recovered."-M. Hevin on Volvulus, in the Mem. De l'Acad. Roy. de Chirurgie, p. 237, vol iv. quarto edition.
"On the 16th April, 1765, M. Sancerotte, Surgeon in Ordinary of the late King of Poland, Duke of Lorraine, opened the body of a man who had been brought to the hospital the evening before. He had been ill nine days with the usual symptoms of strangulated hernia, although there was no appearance of it externally. The pulse had always been small, with severe pain in the right lumbar region. There was an annular opening in the mesentery of a ligamentous consistence, through which had passed the cecum with a part of the colon, and a greater extent of the ileum. The swelling which came on, having changed the relative proportions, these parts of the intestine became strangulated, and not being able to disengage themselves they mortified, after having occasioned first bilious and then stercoraceous vomiting, as usual in such cases. These parts could be withdrawn through the aperture, after evacuating by a puncture the air which distended them."-Ibid. p. 239.
54, Frith Street, Soho Square.
Return to John Snow Publications
18. "Table on the quantity of vapour of ether in 100 cubic inches of air, saturated with it at various temperatures"
Source: Snow, John. Medical Times 15, 23 January 1847, p. 325.
By John Snow, M.D.
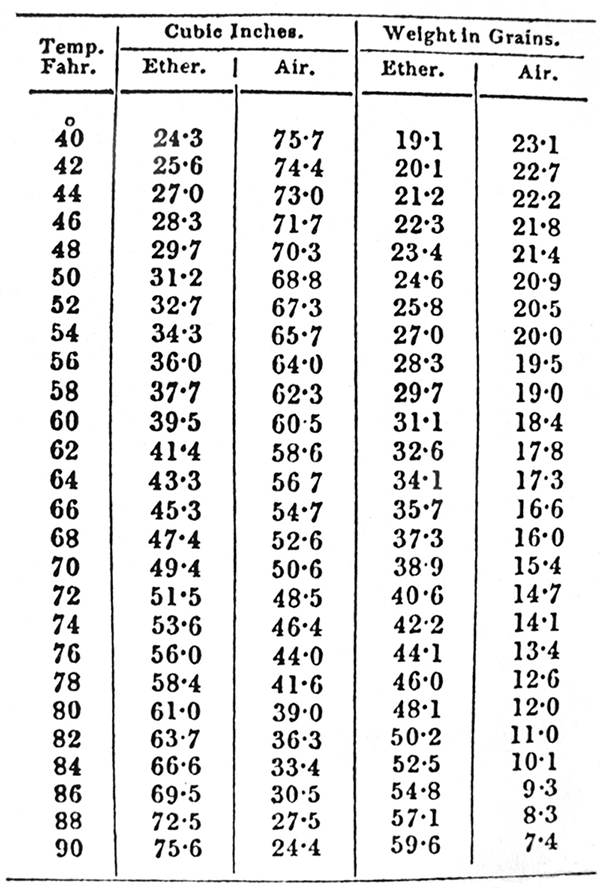
At about 45° the weights of vapour of ether and of air are equal, and at a little above 70° the volumes are equal.
The weights are calculated with the barometer at thirty.
Return to John Snow Publications
19. "Table of the quantity of the vapour of ether "
Source: Snow, John. London Medical Gazette 39, 29 January 1847, pp. 219-220.
By John Snow, M.D.
Table of the quantity of vapour of ether in 100 cubic inches of air, saturated with it at various temperatures.--
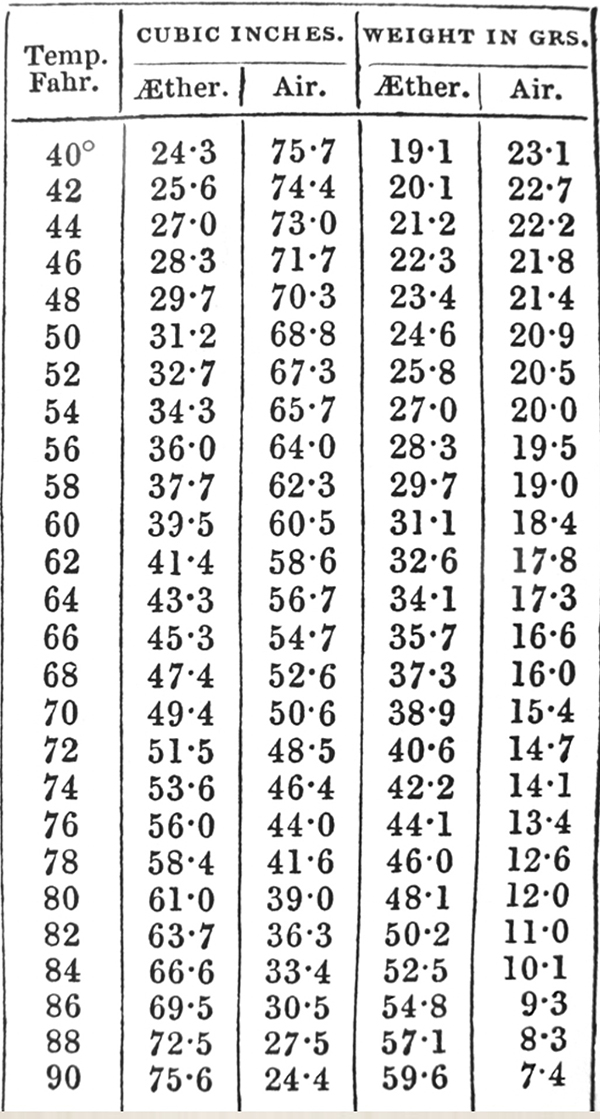
At about 45° the weights of vapour of ether and of air are equal, and at a little above 70° the volumes are equal. The weights are calculated with the barometer at 30.
From this it will be seen that the quantity of ether administered with air varies materially with the temperature.
Return to John Snow Publications
20. "Table of the quantity of the vapour of ether in one hundred cubic inches of air, saturated with it at various temperatures"
Source: Snow, John. The Pharmaceutical Journal 6, 1 February 1847, p. 361.
By John Snow, M.D.
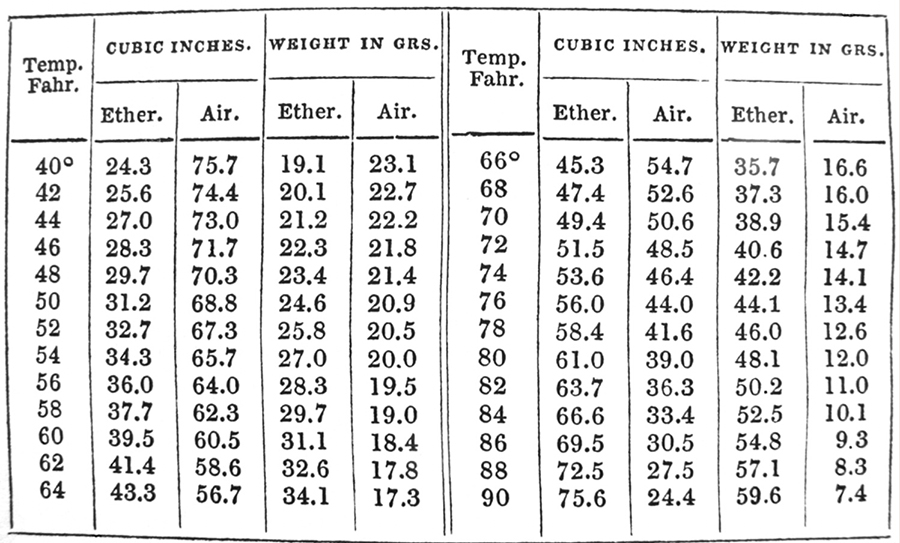
At about 45° the weights of vapour of ether and of air are equal, and at a little above 70° the volumes are equal.
The weights are calculated with the barometer at thirty.
[The mixture of the vapour of ether with atmospheric air being highly explosive, surgical operations ought never to be performed under its influence by candlelight. The result of an explosion under such circumstances would be dreadful.--Ed.]
Return to John Snow Publications
21-22. On the inhalation of the vapor of ether
Source: Snow, John. London Med. Gazette39, 19 March 1847, pp. 498-502, 26 March 1847, pp. 539-542.
By John Snow, M.D., Lecturer on Forensic Medicine at the Medical School Aldersgate Street.
PART 1
It will be at once admitted that the medical practitioner ought to be acquainted with the strength of the various compounds which he applies as remedial agents, and that he ought, if possible, to be able to regulate their potency. The compound of ether vapour and of air is no exception to this rule, although it might be supposed to form one, as the practitioner stands by to watch its effects. For, in the first place these effects vary materially according to the proportion of vapour given with the air, and in the next place, there is a counter process going on with inhalation, viz. exhalation. This increases with the amount of ether absorbed into the blood, and there arrives a point at which the exhalation may equal and just balance the inhalation, if the vapour be very much diluted; and this may occur before insensibility is produced. It is to this circumstance that we are to attribute the origin of the opinion that there are some persons - hard drinkers, for instance, - who are proof against the influence of the vapour. There may be persons on whom it does not act favourably, but I believe that no sentient being is proof against its influence.
It occurred to my mind that by regulating the temperature of the air whilst it is exposed to the ether, we should have the means of ascertaining and adjusting the quantity of vapour that will be contained in it: for the proportion of vapour in any given volume of air saturated with it at any particular temperature, is to the whole volume as the elastic force of the vapour at that temperature is to the atmospheric pressure at the time and place.
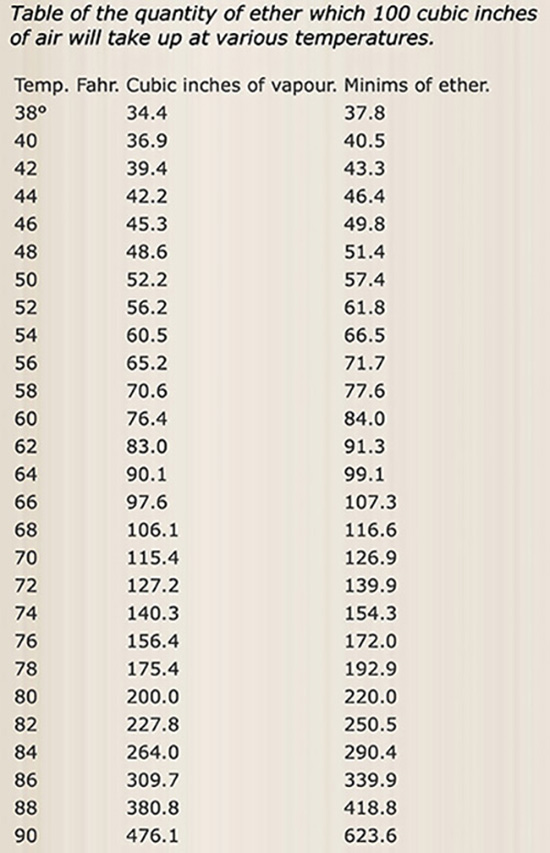
This is true of all vapours in contact with the liquid which gives them off. Now the elastic force of the vapour of ether has been investigated by Dalton and Ure. Imade some experiments with air and ether in graduated tubes over mercury, and found that the quantity of ether vapour taken up at various temperatures corresponded with calculations made according to the formula for the elastic force of the vapour of ether, given by Dr. Ure in his paper on Heat, in the Philosophical Transactions for 1818. I accordingly made use of his table and formula, as I stated at the Westminster Medical Society, in constructing the table published in the [London] Med. Gazette on Jan 29. The ether I used was not altogether free from alcohol, and I concluded this must have been the nature of the ether used by Dr. Ure in his experiments on the elastic force of its vapour; for on making observations afterwards on washed ether, and on every kind of ether over water, (for it then becomes washed,) I found the quantity taken up by air somewhat greater; but the geometrical ratio of increase in the quantity, according to temperature, is the same, as I have ascertained by very numerous observations at all the usual atmospheric temperatures. To make the table I constructed correct for washed ether, which is always used for inhaling, it is necessary to subtract four degrees from the various temperatures; for instance, the numbers opposite 40° are correct for 36° and so on. The ether I first used in my observation boiled at 104°. Washed ether boils at 100°, and if entirely deprived of its water by potash, at 98°. So long as ether contains no alcohol itsspecific gravity does not much influence the elastic force of its vapour, nor consequently the quantity that will mix with air; for water, having a much weaker affinity for ether than alcohol has, exerts less influence over its volatility.
The quantity of vapour of ether which air will take up at different temperatures, may be readily seen by introducing some ether to a measured quantity of air in a graduated receiver over the pneumatic trough, and noting the expansion which takesplace, and the temperature of the air within. The vapour may be washed out of the air by passing it through a quantity of water, and the air may be again measured,when the experiment will have been both synthetical and analytical. The most convenient and satisfactory way of investigating this subject, however, is over mercury, by means of a graduated tube, bent in the form of Dr. Ure's eudiometer, the open leg being the longest. Pass a portion of air into the sealed leg of the tube, about as much as will fill one fourth of it, the quantity being carefully noted, whilst the mercurial level is preserved in the two branches of the tube, andthe required temperature attained by immersing the syphon over its sealed branch,in water contained in a tall glass jar. A great portion of the mercury being withdrawn from the open leg by a long narrow tube, a few drops of ether may be introduced by means of the same tube through the mercury to the air in the sealed leg, by inclining the eudiometer a little, and using a little pressure with the breath on the surface of the ether.
By plunging the eudiometer in water at various temperatures, making a correction for the slight expansion and contraction which takes place in the air itself, from the increase and diminution of heat, and keeping the surface of the mercury level in the two legs, a number of observations may be made in a short space of time; and by washing the ether out of the air afterwards, and observing that the quantity of air is the same as at first, the whole of the observations will be verified.
The following table is suitable for washed ether which boils at 100°, and is quite free from alcohol but not altogether free from water; this being the kind of ether which is usually, and I think very properly, used for inhaling. The barometer is supposed tobe stationary, and at 30°. This table is formed on a different plan from the former, to shew the quantity of vapour that air will take up; and as the air is made a fixed quantity, and the variation of the ether all exhibited in one column, the influence which temperature exerts over it is rendered more apparent to those unaccustomed for a long period to arithmetical calculations. A table formed in this manner is the most correct way of exhibiting the subject, because, since the vapour of ether is absorbed as fast as it arrives at the pulmonary air cells, the quantity inhaled will be influenced rather by the volume of the air, than by that of the mixture of air and vapour, provided the patient's respiration is not obstructed, and it never should be, by the apparatus.
With the assistance of the above table we can determine the proportion of ether to air, and by measuring the ether consumed in an operation, the quantity of air, as well as of vapour, breathed per minute, or throughout the inhalation, can be easily determined by rule of three, and I shall state it in some of the cases I have to relate. This, however, can only be done when an apparatus is used which allows the temperature of the air passing through it to be accurately determined and regulated. The instruments at first used in America and in this country did not allow of any regulation of temperature, but were always used at that of the apartment, whatever it might be, and this afforded no index to the quantity of vapour taken up, for the evaporation of ether in a glass vessel containing sponges cools the air, more or less, according to the thickness of the glass and other circumstances, and it leaves the apparatus many degrees colder than it entered, as may be ascertained by passing air through an apparatus of this kind, and noting the temperature with a delicate thermometer. Glass and sponge being bad conductors of heat, the caloric required to convert the ether into vapour is taken in a great measure from the air passing through the apparatus, it stemperature being thereby reduced, and the quantity of ether which it will take up diminished. Instruments with compartments for warm or hot water, without the means of regulating the temperature of the whole apparatus, are still more objectionable than the former, for by them there is a risk of administering all vapour and no air. Hot water ought never to come near an apparatus for theinhalation of ether nor even warm water, and when its temperature approaches totepid it ought to be carefully regulated.
All that was required to regulate the temperature of both the ether and the air, and,consequently of the resulting mixture, was to bring them into proximity with substances having a good capacity for, and a good power of conducting, caloric.The first we have in water, and the second in the metals; therefore, by placing the ether in a metal vessel, and that vessel in a basin of water brought to the desired temperature by mixing cold and warm water together, the object was attained. Two or three pints of water supply the caloric abstracted in the evaporation of an ounce or two of ether without being much reduced in temperature; and, as the water never requires to be many degrees either above or below the heat of the apartment, its temperature is but little altered by the surrounding air during the short time of an operation.
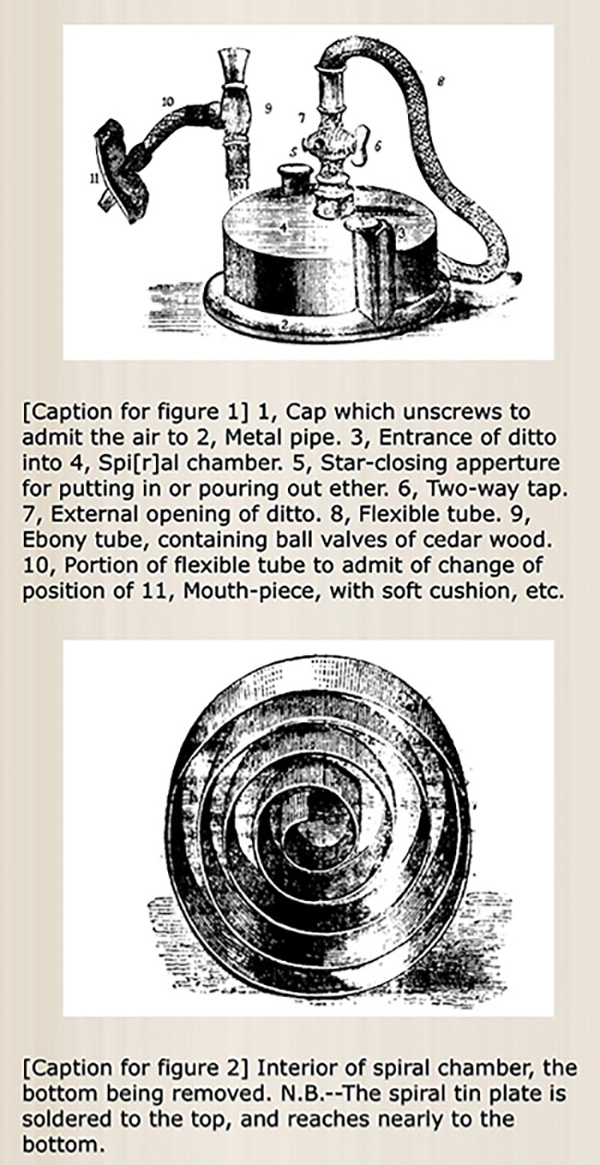
To ensure the saturation of air with the vapour of ether, all that is required is that the air should come in contact with the ether. The larger the surface of the ether exposed, the greater the evaporation, under ordinary circumstances, because it is exposed to more air, but the elastic force of the vapour of ether, at all temperatures above the freezing point of water, is such, that, to saturate the quantity of air which one person can breathe, requires no very great extent of surface. There is no necessity to make the air force its way through the ether, or pass with difficulty through sponges: the ether lies imprisoned in the liquid state only whilst kept down by air already saturated with its vapour, and it is ready to project itself immediately into every fresh portion of air that has access to it, as every one is well aware who has made any experiments with it in jars over the pneumatic trough. However, to insure that the air should come in contact with the ether, and to prevent its being cooled by the contact, I had the interior of the apparatus constructed on the principle of the inhaler of Mr. Jeffreys, described in the Med. Gaz. Feb. 1842, which I had always considered the best inhaler for aqueous vapour. The coils of the tin volute are not so numerous as in the latter but they are amply sufficient for so volatile a liquid as ether. The air has to pass through a pewter pipe before it enters the spiral chamber; by this means it gains the temperature we may wish, and the further advantage is attained, without the impediment of a valve, of preventing evaporation of ether into the room between the inspirations of the patient. In the other instruments that I have seen, there is either a waste of ether in this way, or else there is a valve to admit the air into the inhaler, which must be opened by means of the muscular effort of the patient. The vapour does not find its way in a retrograde direction through 18 inches of curved pipe between the inspirations of the patient; and consequently, whilst there is no impediment to the free passage of air through the apparatus, no ether escapes till it has been breathed by the patient. The mouth-piece I have adopted is furnished with the cushion and India-rubber described by Mr. Tracy in a recent number of the Med. azette. I use, however, the common, and not the vulcanized India rubber, as I understand that the latter frequently, if not always, contains sulphuret of arsenic. As the sudden access of air highly charged with ether produces irritation and cough in some persons, I was desirous ofhaving the means of diluting the vapour to any extent, and Mr. Ferguson, of Giltspur Street, who has taken great pains to carry my wishes into effect, got a tap cast of wide caliber, opening two ways, by means of which the patient can begin by breathing unmedicated air, and have this gradually turned off as the etherized air is admitted in its place. This tap [500/501] offers the further advantage of enabling the medical attendant to keep up the state of insensibility during an operation by a more diluted vapour than that which was necessary to produce that state. All the passages through the apparatus are not less than five-eights of an inch in diameter.
Those cases of administration of ether are generally most successful in which the insensibility is produced in a short space of time; forinstance, from a minute and a half to three or four minutes after the process is fully begun. This we might expect for various reasons; amongst the rest,that no process of inhaling can be carried on without interfering somewhat with the natural state of the respiration and embarrassing to some extent thecirculation; therefore the shorter the process the better.
Although the patient may begin by breathing air, and the ether may be introduced by degrees, yet, by turning the tap a little at each inspiration, the transition may be effected in from a quarter to half a minute. It is necessary to the success of the process that the nostrils and mouth be carefully closed. The patient should have plenty of air, it is true, but it should all come charged with the vapour, otherwise there can be no certainty about the process, and the patient will be more likely to become inebriated than insensible. The temperature I have nearly always applied has been from 65° to 70°, between which points the proportion of vapour and of air does not differ much from equality (to be continued in Part 2).
PART 2
In those instances in which I have watched the pupil of the eye narrowly, I have observed it to dilate, as the patient is getting under the influence ofthe vapour. This dilation is, however, but transitory, and the pupil usually becomes somewhat contracted, and the eye turned up as in sleep, as soon as the patient becomes insensible to pain. The breathing at the same time becomes deep, slow, and regular, and there is an absence of voluntary motion and a relaxation of the muscles, the orbicularis muscle ceasing to contract again on the eyelids being raised by the finger. An operation maybe commenced in this condition of the patient, with confidence that he will remain as passive as a dead subject. This having been found to be the case, in order to maintain the insensibility without further increasing it, I am inthe habit of partly turning the two-way tap to dilute the vapour; and it has seemed to me that by turning it about half way, so as to admit an equal quantity of external air, and reduce the vapour to about 25 per cent, that object has been attained: but a more extensive experience is required on this point, and perhaps the proportion required may vary in different patients. This method of continuing a more diluted vapour I have found to keep up the insensibility better than leaving off the process and resuming it by turns. But if the respiration becomes too slow, or at all stertorous, or if the pulse becomes very small or feeble, the nostrils should be at once liberated, and the admission of fresh air will afford immediate relief. I should think it unsafe to fasten a mask on the face, by means that would interfere with the instantaneous admission of air, for on one occasion I saw an animal killed by ether by a momentary delay. It was placed in a small glass jar, and when it appeared to have had as much of the vapour as it could bear, I attempted to take it out, but could not reach it with my fingers, and whilst turning round for some means of extricating it, it expired.
In nineteen cases out of twenty in which the pulse was carefully noticed, it increase in frequency during the inhalation, often very much, becoming as frequent as 180 in the minute in some patients in whom, from debility, it was frequent before the process began. Generally the pulse has also become smaller and more feeble. In one instance, that of a lady reduced in strength by malignant disease, it became smaller, but not more frequent; and as soon as the inhalation was discontinued, it became fuller and stronger than before the inhalation began. The pulse generally recovers its volume almost directly the inhalation is discontinued; in several instances, as in the above,becoming stronger than before: but it remains frequent for some minutes.The immediate effect on the circulation, of the absorption of the vapour in the lungs, appears to be an impediment to the flow of blood through the pulmonary capillaries. Less blood reaches the left side of the heart to be sent into the arteries, which diminish in caliber, but the heart contracts more frequently in order to keep up a supply. The escape of the vapour from the blood again seems to exert a contrary effect on the circulation, as evidenced, in general, by the pulse. I may perhaps be allowed to make a quotation bearing on this subject from a paper of mine in the Med. Gaz., vol. Xxxi.: - "As safreetida, ether, various essential oils, camphor, and other volatile medicines, relieve difficult and impeded respiration.... They are all separated from the blood in the lungs, and escape with the breath ... increasing very much the quantity of vapour which exhales from the pulmonary capillaries, and thus giving additional impetus to the blood: in this way lessening congestion and relieving its distressing symptoms. As this class of medicines promote the function of respiration, I will venture to call them diapnetics, from ??? and ????."
I have seen two cases in which the depressing effect of the inhalation was considerable, and was not followed by reaction directly it was discontinued.As this appears to have been the case in the instance attended with fatal result at Colchester, and related in the Medical Gazette of the 5th inst.,it may be desirable to enter into the particulars of one of these. A lady, 41 years of age, in pretty good health, the patient of Dr. Fredrick Bird, inhaled ether on the occasion of having a tumor removed connected with the external generative organs. She inhaled for eight minutes, during which time it was observed that the respiration was feeble and slow. The pulse, however, which had been about natural before the inhalation, became feeble and very frequent, and the patient began to struggle as if suffering from want ofbreath; the process was discontinued although she did not appear insensible, and the operation was commenced. She flinched and cried out at the first incision, although she did not afterwards remember the pain. She becamevery faint during the operation, although there was but little loss of blood,and it was necessary to give brandy, and lower the head to the horizontal posture. Consciousness soon returned, and as some sutures were made inthe skin, she spoke coolly of beginning to feel a little pain. The feeling of faintness continued more or less all night, but her recovery was very good. The apparatus in this instance was placed in water at 70°, being lower than the temperature of the room. Two fluid ounces of ether were put in, and three drachms remained; consequently 13 drachms were inhaled, equal to about 709 cubic inches of vapour; and as it was washed ether, each 115 cubic inches would be combined with 100 cubic inches of air; consequently only about 616 cubic inches of air were breathed, making 1325 cubic inches of airand vapour: but in eight minutes the patient ought to have breathed about 2400 cubic inches of air alone. The ether in this instance appeared to act as a sedative to the function of respiration, and the small amount of air breathed may perhaps account for the depressing effects.
In two or three instances there have been some struggling and a distended state of the superficial veins, the skin being rather purple, and the conjunctiv somewhat injected. In one instance this seemed to arise from cough being excited by the vapour, on account of the bronchial membrane being in an irritable state, and in the others I believe it arose from obstructed respiration, which in future may be avoided, rather than from the direct effect of the vapour. By the kindness of the surgeons to St.George's Hospital, I have had the honour of giving the vapour of ether at thirteen surgical operations - most of them important ones - in the hospital during the last six weeks, having the valuable advice of the surgeons, and occasionally also of one or two of the physicians to the hospital, to aid me in so giving it. It has been successful in altogether preventing pain in all the cases but one or two, and even in these there was but very little of the pain that there otherwise would have been; and there have been no ill effects of any kind following the inhalation of the ether. I allude to these cases toremark that five of the patients were children of various ages, from the fifth year upwards, and that they inhaled more easily than the adults generally did; that they were more quickly affected, generally becoming quite insensible in less than two minutes, and always without any struggling which sometimes occurred in the adults.
For a variety of reasons, and from close observations, I have arrived at the conclusion, that this difference has not arisen strictly from a different effect of ether on subjects ofdifferent ages, but from a cause within our control. The same inhaler was used in all, consequently the tubes were wider in proportion for children than for adults. I have described all the passages of the apparatus as not less than five-eights of an inch in diameter; but such is the description rather of what I wanted than of any instrument Ihave used. Valves and tubes such as were already in existence have been made use of, and the caliber in some part of its extent has always been contracted to half an inch, and this I consider only enough for a child, but not for the adult. As only half, and often not so much as half, of what is inhaled is air, it is particularly requisite that the [540/541] tubes should be wide. I am now getting elastic tubes, valves and mouth-tubes, made purposely for the apparatus three quarters of an inch in diameter, as wide, in fact, as the barrel of a fowling piece, and intend to give ether as fair a trial in adults as hitherto, I believe, it has had in children only.* (*Since the above was written, I have used these large tubes, and found them to answer my expectation.) The pipe admitting air to the ether will be five-eights, and all the passages for the air expanded by vapour, three-quarters of an inch in diameter. It may be supposed that there is no occasion tomake the tubes larger than the trachea, but something ought to be allowed for the friction of the air against the interior of the tubes.
With the assistance of the above table we can determine the proportion of ether to air, and by measuring the ether consumed in an operation, the quantity of air, as well as of vapour, breathed per minute, or throughout the inhalation, can be easily determined by rule of three, and I shall state it in some of the cases I have to relate. This, however, can only be done when an apparatus is used which allowsthe temperature of the air passing through it to be accurately determined and regulated. The instruments at first used in America and in this country did notallow of any regulation of temperature, but were always used at that of the apartment, whatever it might be, and this afforded no index to the quantity of vapour taken up, for the evaporation of ether in a glass vessel containing sponges cools the air, more or less, according to the thickness of the glass and other circumstances, and it leaves the apparatus many degrees colder than it entered, as may be ascertained by passing air through an apparatus of this kind, and noting the temperature with a delicate thermometer. Glass and sponge being bad conductors of heat, the caloric required to convert the ether into vapour istaken in a great measure from the air passing through the apparatus, its temperature being thereby reduced, and the quantity of ether which it will take up diminished. Instruments with compartments for warm or hot water, without the means of regulating the temperature of the whole apparatus, are still more objectionable than the former, for by them there is a risk of administering all vapour and no air. Hot water ought never to come near an apparatus for the inhalation of ether nor even warm water, and when its temperature approaches to tepid it ought to be carefully regulated.
All that was required to regulate the temperature of both the ether and the air, and,consequently of the resulting mixture, was to bring them into proximity with substances having a good capacity for, and a good power of conducting, caloric.The first we have in water, and the second in the metals; therefore, by placing the ether in a metal vessel, and that vessel in a basin of water brought to the desired temperature by mixing cold and warm water together, the object was attained. Two or three pints of water supply the caloric abstracted in the evaporation of an ounce or two of ether without being much reduced in temperature; and, as the water never requires to be many degrees either above or below the heat of the apartment, its temperature is but little altered by the surrounding air during the short time of an operation.
With respect to the psychological phenomena produced by ether, I have observed that consciousness seems to be lost before the sensibility to pain, and if an operation is commenced [i]n this stage, the patient will flinch, and even utter cries, and give expressions of pain, but will not remember it, and will assert that he has felt none.
Metaphysicians have distinguished between sensibility and perception - between mere sensation and the consciousness or knowledge of that sensation, though the two functions have, as they supposed, always been combined. Ether seems to decompose mental phenomena as galvanism decomposes chemical compounds, allowing us to analyse them, and showing that the metaphysicians were right. During the recovery of the patient, consciousness, which first departed generally returns first, and the curious phenomenon is witnessed of a patient talking, often quite rationally, about the most indifferent matters, whilst his body is being cut or stitched by the surgeon. I have never seen this insensibility to pain during the conscious state except where consciousness had been previously suspended. In the paper on the capillary circulation, in the Medical Gazette, to which I have alluded above, I offered the opinion that the pain of inflammation depended on a great increase of the natural sensibility of the inflamed part. Under the influence of ether we sometimes see the converse of this, viz. what would be pain reduced to an ordinary sensation; thus, some patients,whilst recovering their consciousness, feel the cuts of the surgeon without the smart. A nobleman, the patient of Mr. Tracy, of Hill Street, Berkeley Square, described the lancing of an abscess as the sensation of something cold touching the part; the manipulation of the abscess, which at another time would have been painful, he did not feel at all.
If the patient will remain silent during his recovery from the effects of ether, as he generally will, it is better not to trouble him with questions till he has perfectly regained his faculties, as conversation seems to increase the tendency to excitement of the mind that sometimes exists for a few minutes as the patient is recovering from the effects of ether. This kind of inebriation is sometimes amusing, but is not a desirable part of the effects of ether, more especially on so grave an occasion as a serious surgical operation; and therefore anything that may prevent or diminish it is worthy of attention. The children have all appeared to recover their consciousness very quickly, and without any kind of aberration of mind.
Any organic disease which impedes the flow of blood through the heart and lungs would seem to contraindicate the exhibition of ether by inhalation, and I should consider a hurried state of the circulation, such as that induced by strong labour pains, likewise to offer an objection to the process.
It was my intention to make some remarks on the probable way in which ether acts in suspending sensibility; but, as what I have already written is probably sufficient for one article, I will reserve that part of the subject for a future communication, and will be content, at present, to refer to a short abstract of some of my experiments and opinions which appeared in the number for Feb., 26.
In concluding, however, I should wish to observe that I am inclined to look upon the new application of ether as the most valuable discovery in medical science since that of vaccination. From what I have seen, I feel justified in the conclusion that ether may be inhaled for nearly all surgical operations, with the effect of preventing pain, not only with safety and without ill-consequences, where due care is taken, but in many cases with [541/542] the further advantage of improving the patient's prospect of recovery; the pain of an operation forming often a considerable part of what renders it dangerous, and many patients after ether, having seemed to recover better than might, without it,have been expected.
In the amputations performed at St. George's Hospital whilst the patients were under the influence of ether, it has been remarked, as was stated by Mr. Cutler, on Feb. 11th, that there has been an absence of the painful spasmodic starting of the stump, which usually renders it necessary for a nurse to sit and hold it for some hours after the operation.
54, Frith Street, Soho.
Return to John Snow Publications
23. "On the inhalation of the vapour of ether"
Source: Snow, John. British and Foreign Medical Review 23 (April 1847) pp. 573-576.
The full title of this periodical is the British and Foreign Medical Review or Quarterly Journal of Practical Medicine and Surgery, Vol. 23 is dated January - April 1847. [Note: contains extracts from article #22, i.e. in LMG 39, 26 March 1847, 539-542.]
By John Snow, M.D.
"In those instances in which I have watched the pupil of the eye narrowly, I have observed it to dilate, as the patient is getting under the influence of the vapour. This dilation is, however, but transitory, and the pupil usually becomes somewhat contracted, and the eye turned up as in sleep, as soon as the patient becomes insensible to pain. The breathing at the same time becomes deep, slow, and regular, and there is an absence of voluntary motion and a relaxation of the muscles, the orbicularis muscle ceasing to contract again on the eyelids being raised by the finger. An operation may be commenced in this condition of the patient, with confidence that he will remain as passive as a dead subject. This having been found to be the case, in order to maintain the insensibility without further increasing it, I am in the habit of partly turning the two-way tap to dilute the vapour; and it has seemed to me that by turning it about half way, so as to admit an equal quantity of external air, and reduce the vapour to about 25 per cent, that object has been attained: but . . . more extensive experience is required on this point, and perhaps the proportion required may vary in different patients. This method of continuing a more diluted vapour I have found to keep up the insensibility better than leaving off the process and resuming it by turns. But if the respiration becomes too slow, or at all stertorous, or if the pulse becomes very small or feeble, the nostrils should be at once liberated, and the admission of fresh air will afford immediate relief. I should think it unsafe to fasten a mask on the face, by means that would interfere with the instantaneous admission of air, for on one occasion I saw an animal killed by ether by a momentary delay. It was placed in a small glass jar, and when it appeared to have had as much of the vapour as it could bear, I attempted to take it out, but could not reach it with my fingers, and whilst turning round for some means of extricating it, it expired.
"In nineteen cases out of twenty in which the pulse was carefully noticed, it increase in frequency during the inhalation, often very much, becoming as frequent as 180 in the minute in some patients in whom, from debility, it was frequent before the process began. Generally the pulse has also become smaller and more feeble. In one instance, that of a lady reduced in strength by malignant disease, it became smaller, but not more frequent; and as soon as the inhalation was discontinued, it became fuller and stronger than before the inhalation began. The pulse generally recovers its volume almost directly the inhalation is discontinued; in several instances, as in the above, becoming stronger than before: but it remains frequent for some minutes. . . .
"I have seen two cases in which the depressing effect of the inhalation was considerable, and was not followed by reaction directly it was discontinued. . . . A lady, 41 years of age, in pretty good health, the patient of Dr. Fredrick Bird, inhaled ether on the occasion of having a tumor removed connected with the external generative organs. She inhaled for eight minutes, during which time it was observed that the respiration was feeble and slow. The pulse, however, which had been about natural before the inhalation, became feeble and very frequent, and the patient began to struggle as if suffering from want of breath; the process was discontinued although she did not appear insensible, and the operation was commenced. She flinched and cried out at the first incision, although she did not afterwards remember the pain. She became very faint during the operation, although there was but little loss of blood, and it was necessary to give brandy, and lower the head to the horizontal posture. Consciousness soon returned, and as some sutures were made in the skin, she spoke coolly of beginning to feel a little pain. The feeling of faintness continued more or less all night, but her recovery was very good. The apparatus in this instance was placed in water at 70°, being lower than the temperature of the room. Two fluid ounces of ether were put in, and three drachms remained; consequently 13 drachms were inhaled, equal to about 709 cubic inches of vapour; and as it was washed ether, each 115 cubic inches would be combined with 100 cubic inches of air; consequently only about 616 cubic inches of air were breathed, making 1325 cubic inches of air and vapour: but in eight minutes the patient ought to have breathed about 2400 cubic inches of air alone. The ether in this instance appeared to act as a sedative to the function of respiration, and the small amount of air breathed may perhaps account for the depressing effects.
"In two or three instances there have been some struggling and a distended state of the superficial veins, the skin being rather purple, and the conjunctivæ somewhat injected. In one instance this seemed to arise from cough being excited by the vapour, on account of the bronchial membrane being in an irritable state, and in the others I believe it arose from obstructed respiration, which in future may be avoided, rather than from the direct effect of the vapour. By the [574/575] kindness of the surgeons to St. George's Hospital, I have had the honour of giving the vapour of ether at thirteen surgical operations--most of them important ones--in the hospital during the last six weeks, having the valuable advice of the surgeons, and occasionally also of one or two of the physicians to the hospital, to aid me in so giving it. It has been successful in altogether preventing pain in all the cases but one or two, and even in these there was but very little of the pain that there otherwise would have been; and there have been no ill effects of any kind following the inhalation of the ether. I allude to these cases to remark that five of the patients were children of various ages, from the fifth year upwards, and that they inhaled more easily than the adults generally did; that they were more quickly affected, generally becoming quite insensible in less than two minutes, and always without any struggling which sometimes occurred in the adults. For a variety of reasons, and from close observations, I have arrived at the conclusion, that this difference has not arisen strictly from a different effect of ether on subjects of different ages, but from a cause within our control. The same inhaler was used in all, consequently the tubes were wider in proportion for children than for adults. I have described all the passages of the apparatus as not less than five-eights of an inch in diameter; but such is the description rather of what I wanted than of any instrument I have used. Valves and tubes such as were already in existence have been made use of, and the caliber in some part of its extent has always been contracted to half an inch, and this I consider only enough for a child, but not for the adult. As only half, and often not so much as half, of what is inhaled is air, it is particularly requisite that the tubes should be wide. I am now getting elastic tubes, valves and mouth-tubes, made purposely for the apparatus three quarters of an inch in diameter, as wide, in fact, as the barrel of a fowling piece, and intend to give ether as fair a trial in adults as hitherto, I believe, it has had in children only. [*footnote excluded from extract] The pipe admitting air to the ether will be five-eights, and all the passages for the air expanded by vapour, three-quarters of an inch in diameter. It may be supposed that there is no occasion to make the tubes larger than the trachea, but something ought to be allowed for the friction of the air against the interior of the tubes.
"With respect to the psychological phenomena produced by ether, I have observed that consciousness seems to be lost before the sensibility to pain, and if an operation is commenced [i]n this stage, the patient will flinch, and even utter cries, and give expressions of pain, but will not remember it, and will assert that he has felt none. Metaphysicians have distinguished between sensibility and perception--between mere sensation and the consciousness or knowledge of that sensation, though the two functions have, as they supposed, always been combined. Ether seems to decompose mental phenomena as galvanism decomposes chemical compounds, allowing us to analyse them, and showing that the metaphysicians were right. During the recovery of the patient, consciousness, which first departed generally returns first, and the curious phenomenon is witnessed of a patient talking, often quite rationally, about the most indifferent maters, whilst his body is being cut or stitched by the surgeon. I have never seen this insensibility to pain during the conscious state except where consciousness had been previously suspended. In the paper on the capillary circulation, in the Medical Gazette, to which I have alluded above, I offered the opinion that the pain of inflammation depended on a great increase of the natural sensibility of the inflamed part. Under the influence of ether we sometimes see the converse of this, viz. what would be pain reduced to an ordinary sensation; thus, some patients, whilst recovering their consciousness, feel the cuts of the surgeon without the smart. A nobleman, the patient of Mr. Tracy, of Hill Street, Berkeley Square, described the lancing of an abscess as the sensation of something cold touching the part; the manipulation of the abscess, which at another time would have been painful, he did not feel at all.
"If the patient will remain silent during his recovery from the effects of ether, as he generally will, it is better not to trouble him with questions till he has perfectly regained his faculties, as conversation seems to increase the tendency to excitement of the mind that sometimes exists for a few minutes as the patient is recovering from the effects of ether. This kind of inebriation is sometimes amusing, but is not a desirable part of the effects of ether, more especially on so grave an occasion as a serious surgical operation; and therefore anything that may prevent or diminish it is worthy of attention. The children have all appeared to recover their consciousness very quickly, and without any kind of aberration of mind.
"Any organic disease which impedes the flow of blood through the heart and lungs would seem to contraindicate the exhibition of ether by inhalation, and I should consider a hurried state of the circulation, such as that induced by strong labour pains, likewise to offer an objection to the process.
. . . . . . . . . . . . . . .
"In concluding, however, I should wish to observe that I am inclined to look upon the new application of ether as the most valuable discovery in medical science since that of vaccination. From what I have seen, I feel justified in the conclusion that ether may be inhaled for nearly all surgical operations, with the effect of preventing pain, not only with safety and without ill consequences, where due care is taken, but in many cases with the further advantage of improving the patient's prospect of recovery; the pain of an operation forming often a considerable part of what renders it dangerous, and many patients after ether, having seemed to recover better than might, without it, have been expected. In the amputations performed at St. George's Hospital whilst the patients were under the influence of ether, it has been remarked, as was stated by Mr. Cutler, on Feb. 11th, that there has been an absence of the painful spasmodic starting of the stump, which usually renders it necessary for a nurse to sit and hold it for some hours after the operation.
(London Med. Gazette, March 26th, 1847.)
Return to John Snow Publications
24. "To the editor of the Pharmaceutical Journal"
Source: Snow, John. The Pharmaceutical Journal 6, 1 April 1847, pp. 474-475 [Letter to Ed.].
To the Editor of the Pharmaceutical Journal.
Sir,--I shall be obliged if you will allow me, in reply to an observation in the last number of your journal, to state that the resemblance between the inhaler of Mr. Jeffreys, and that I have introduced for the vapour of ether, is not a coincidence, but is the result of my previous acquaintance with the former, and approval of it; and that I have never failed to mention the circumstance when saying or writing anything about the apparatus. The first notice of it in print appeared simultaneously in two medical journals, and contained the following words: "The instrument which Mr. Ferguson, of Smithfield, was making for him, was on the plan of the inhaler of Mr. Jeffreys, with some alterations and additions." (Med. Gaz. Jan. 22, p. 156, and Lancet, Jan. 23, p. 99.)
The object of the apparatus is to regulate the proportion of vapour in the air by regulating the temperature; and to effect this, I take advantage of the capacity for caloric which there is in two or three pints of water, and of the conducting power of metal of which the instrument is formed. The form I have adopted, is a matter of detail to enlarge the surface of ether exposed to the air.
The table you honoured me by publishing in the February number, is correct for ether, which is not free from alcohol, and boils at 104°. To make it correct for washed ether, which boils at 100° four degrees must be deducted; for instance, for 40° read 36°, and so on, and for washed ether deprived of its water by potash, and boiling at 98°, six degrees must be deducted. As I have stated elsewhere, I made use in constructing that table, of the formula for the elastic force of the vapour of ether, by Dr. Ure, in his paper on Heat, in the Philosophical Transactions for 1818; having ascertained by experiments, that it could be used with correctness for that purpose.
I remain, Sir, your obedient servant,
John Snow, M.D.
54, Frith Street, Soho, March 5th, 1847.
[We regret the observation we made last month, which, from Dr. Snow's statement, appears to have been erroneous.--Ed.]
Return to John Snow Publications
25. "A lecture on the inhalation of vapour of ether in surgical operations"
Source: Snow, John. Lancet 1, 29 May 1847, pp. 551-54.
By John Snow, M.D.,
Lecturer on Forensic Medicine.
If a medical man had been asked, this time last year, whether it were possible to perform a severe surgical operation without the patient's feeling or showing any sign of pain, he would have answered in the affirmative. Such occurrences have taken place in profound insensibility arising from injuries of the head. In a state of imminent suffocation, from inflammation of the windpipe, that tube has been cut open in the throat without the patient being sensible of what was done; and operations might be performed in the deep insensibility of apoplexy and of epilepsy, without the sufferers feeling them. But if any one had been asked last year, whether it would be safe and practicable to induce such a state of insensibility as would prevent the most serious surgical operations being felt, and that without any ill consequences, he would, I think, undoubtedly have considered it an impossibility. Sir Humphry Davy, indeed, nearly fifty years ago, expressed an opinion that nitrous oxide gas might probably be used to prevent pain during surgical operations, but the laughing gas, as it is called, continued to be inhaled in small quantities for amusement only, and the suggestion of Davy was unattended to, at least till recently; for it appears that it was in some measure by following out the researches of Sir Humphry Davy, that Dr. Jackson was led to the recent brilliant, important, and most valuable discovery.
The inhalation of ether for the prevention of pain during surgical operations, was, as all are aware, introduced by Drs. Jackson and Morton, of Boston, U.S., at the end of last year. Another medical man, indeed, in America, is claiming the merit of the discovery, but a little time, no doubt, will suffice to decide to whom the merit is due, or how it should be apportioned. The only way in which I can exhibit the influence of ether on the present occasion, is on animals; they show the effects of it, however, in a very striking manner, and will illustrate what I have to say afterwards.
The ether I pour into this jar is sufficient to make as much vapour as will one-third fill the jar; it is already converted into vapour, and the jar contains a mixture of two-thirds air and one-third vapour of ether. I have a thrush which I shall put in, just sliding the plate-glass which covers it enough to admit the bird, which will be very quickly insensible. The vapour of ether acts in a very uniform manner on the various classes of animals. The difference in the time they take to become affected and to recover, depends on the difference in the activity of the respiratory and circulating functions. Birds enjoy these functions in the highest perfection, and they are most quickly brought under the influence of ether; they breathe more air in proportion to their size than other animals, and, consequently, inhale the vapour more quickly. This thrush was only in the vapour for about a minute, and it is dead. It has ceased to breathe before I took it out of the jar. It is a result I did not intend, and it has arisen from my going on with the lecture, and looking at my notes, instead of directing my whole attention to the animal. This accident shows the power of the agent, but it does not follow that there is any danger in giving the vapour to a patient; for of course the medical man directs the whole of his attention to what he is doing; he understands his own species better than a bird, and can feel the pulse, and make many observations which I could not on the bird, even if I had attended to it. Besides, the vapour acts much less rapidly on human beings and on quadrupeds than on birds. The large jar in which I am placing this guinea-pig is occupied with an atmosphere of one-half vapour of ether, and the remainder air. It will be quite insensible in two or three minutes--voluntary motion has ceased, and there is no visible movement in it except that of respiration. If I take it out now, I shall probably be able to prick it without causing it to move. That is the case. It now, however, moves its foot on being pricked; it is quickly recovering its sensibility in the air. I shall put it in the jar for a minute longer--it is not deeply insensible, but will recover completely in five or ten minutes.
I shall pour some ether into this dish placed over the water in which you see these gold fishes; I enclose the whole in a bell-glass, and as the ether evaporates, the vapour will be absorbed by the water, and the fishes will breathe it by their gills. They will become insensible towards the end of the lecture, will turn on the side, and exhibit no motion except a slow movement of the gills, and on being put into fresh water they will gradually recover. Quadrupeds of warm blood are affected much less quickly than birds, by vapour of the same strength, reptiles still less quickly, and fishes, which get the air they breathe only at second-hand through the water, are much longer in coming under the influence of ether, and, also, in recovering from its effects.
The same relation of the effects of the inhalation of ether to the breathing, and circulation of the blood, holds good in various individuals of the human species, as well as in different classes of animals. In children, the breathing and circulation of the blood are more rapid than in adults, and children and youths are put sooner and more easily under the influence of ether than persons of the middle period of life, and these again sooner than old people, in whom the respiration and circulation are slow. Children under fifteen I have generally found to become sufficiently insensible for an operation to be commenced on them in two minutes after commencing to breathe vapour of the same strength, although there have been exceptions, some of them becoming insensible in two minutes. Elderly people are usually five to six minutes.
The apparatus at first used in America and in this country for the inhalation of ether were glass vessels, and generally contained sponges. They were not provided with any means of regulating the proportions of vapour of ether and of air, and they had a worse fault--that of being cooled by the evaporation of the ether taking place within. The air was cooled in passing through, and took up less and less vapour as the process went on, and sometimes when the patient was on the point of becoming insensible, no further effect was produced, or when seemingly insensible, he was roused up by the surgeon's knife. An opinion began to be entertained, that there were some persons, especially hard drinkers, who could not be rendered insensible by ether; but I believe that no sentient being is proof against its effects, and I no more mistrust the power of the ether than the surgeon mistrusts that of his knife. Several patients to whom I have administered vapour of ether have been habitual hard drinkers, and I have not remarked that there was any difficulty with them. One man who had his forearm amputated by Mr. Cæsar Hawkins, at St. George's Hospital, had been in the habit of drinking a pint of rum before breakfast, yet the operation was commenced in four minutes after he began to inhale, without his showing any signs of feeling it, or remembering anything of it afterwards.
Ether possesses, in an eminent degree, the property of becoming converted into vapour. When in contact with the air, its vapour mixes with, and expands it. The quantity of vapour that will thus mix with the air, increasing with the temperature in a certain geometrical ratio,--the same ratio which the elastic force of the vapour of ether bears to the temperature. The boiling point of the ether most suitable for inhaling is 100°, and this table shows the quantity of such ether that 100 cubic inches of air will take up when saturated with it at various temperatures at a mean barometric pressure of thirty inches:--
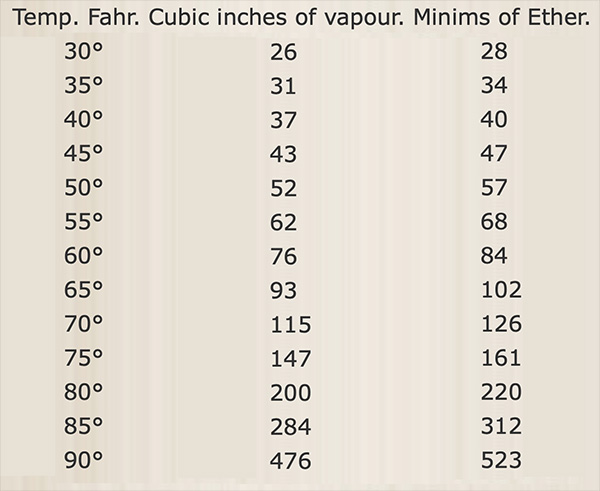
Thus, at 30°, 100 cubic inches of air take up 26 cubic inches of vapour, and become 126 cubic inches; at about 67° they take up 100, and are expanded to 200 cubic inches; above this temperature, the quantity of vapour increases with enormous rapidity, till, at 100°, it excludes the air entirely. The same quantity of air was introduced into each of these graduated tubes, and into this some ether was passed up, and it has expanded the air to about twice its bulk. As I drop a little ether on the muslin which covers the tube, the diminution of heat produced by its evaporation causes the vapour within to be little more than its original space; but by grasping the tube with my hand, the ether is again converted into vapour, and the space within increases as rapidly as it diminished, showing how readily air becomes saturated with vapour of ether.
By taking advantage of this law, of the quantity of ether-vapour that will mix with air at different temperatures, we are enabled to regulate the proportion of vapour and of air that a person breathes. In order to do this, it is only necessary to bring the air and ether sufficiently in contact, and to regulate their temperature. To do this, I took advantage of the capacity for heat that there is in water, and of the power of conducting it possessed by the metals. By making the inhaler of metal, and placing it in water, the ether it contains, and the air passing through it, are kept of the temperature of the water, which can be regulated by the thermometer. Two or three pints of water supply the heat necessary to the evaporation of an ounce or two of ether, without being much lowered in temperature. The water in which I place the apparatus does not differ much in temperature from the patients' room. In winter I added a little hot water to the cold, but since the weather became mild, that is not always required. The temperature I nearly always employ is between 60° and 70°, and consequently the air and vapour are about in equal quantity. I think it preferable that the air should exceed the vapour, rather than the reverse, and any temperature not lower than 60° I believe to be sufficient. Care should be taken not to bring hot, or even warm, water in contact with an ether inhaler, otherwise the patient will be prevented from obtaining any air with the vapour. Placing the apparatus in a quantity of water prevents the cooling of it by the evaporation of the ether within and maintains the process steady and equable throughout.*
(*For a description and an engraving of Dr. Snow's apparatus, see the Lancet, Jan. 30. In that exhibited at the lecture, there was a two-way tap, and one or two alterations since made.)
In order that the inhaler should not stand in the way of the surgeon and his assistants, who want all the room they can get, it is necessary to have an elastic tube between the inhaler and the patient's mouth, and it is of great importance that the tube should be of sufficient capacity. The tube I first used was half an inch in internal diameter, that being the widest to be met with, and wider than those still used with many inhalers: but I found reason to suspect it was not wide enough, and I tried it by breathing through it myself without any ether, and found that I got out of breath in three minutes. The friction of the air against the interior of a tube causes considerable resistance; to obviate this it becomes necessary to have the tube much wider than the windpipe. The elastic tube I always use for the adult is three-quarters of an inch in internal diameter, and by it the patient can fill and empty his chest as rapidly as he likes, without labour. The other apertures, through which the air and vapour have to pass, are not less than five-eights of an inch in diameter. The spherical valves are of cedar wood, and are therefore very light and easily moved. It is of great importance to take care that nothing of suffocation is blended with the exhibition of ether. Asphyxia, it is true, produces insensibility to pain, as I have ascertained by experiments on animals, but the insensibility of a state of suffocation is painful to produce, is of short duration before it ends either in recovery or death, and is attended with great danger, not only present but subsequent. Partial suffocation is often followed by illness, of which a person may expire in a day or two, but I believe that no such result need be apprehended from ether, if the patient has sufficient air with it. If the animals I have placed in ether vapour have not ceased to breathe before they were withdrawn from it, they have always completely recovered, and been as well as before, however nearly dying they might be when taken out, except, indeed, a bird which was put into oxygen gas, and did not recover.
It is necessary to the success of the process that the mouth and nostrils be carefully closed against the admission of air except that which comes charged with vapour of ether from the apparatus; for if the air can gain admittance by any shorter method, it does so, and we cannot tell how much vapour the patient is inhaling. An intelligent patient can begin, it is true, by breathing voluntarily just as we wish him, but he loses his voluntary power before he is sufficiently insensible to bear an operation without being roused. I have used different kinds of mouth-pieces, and have only lately got one which fulfils its intention completely. It has been invented and sent to me by Mr. Sibson, of the Nottingham General Hospital. It encloses the mouth and nostrils both, fitting over the bony bridge of the nose, and permitting respiration to go on by the nostrils or mouth, as the patient's wish or instinct leads. This I consider a great desideratum, for the nostrils are the natural channel of the breath, and closing them during inhalation causes apparent uneasiness and struggling in some persons. This face-piece contains flexible sheet-lead in its border, and can be moulded to the peculiarities of any kind of features, and retains the form into which it is moulded. I have used it several times, and have found it to answer completely.
I let the patient begin by inhaling only air, and then turn the two-way tap a little at each inspiration, till the etherized air is admitted, to the exclusion of the other. This prevents the coughing which the sudden access of the vapour occasions in some persons. The air passages rapidly get a tolerance of the vapour, when admitted gradually. I usually get the tap quite turned in a quarter of a minute. I find that consciousness and the power of voluntary motion are soon lost, generally in the first minutes, and for some time before a surgical operation could be commenced without causing pain, and awaking the patient. I am aware that different accounts have been given from this, of the effect of ether, and the effect may be different when the vapour is of a different strength, and given in a different manner, but I have stated what I have always observed, from vapour diluted with an equal quantity, or rather more, of air. As the patient gets under the influence of ether, the limbs become relaxed, and drop down, if not supported, but the eyelids still retain their sensibility, and close again on being opened by the finger, but in a little time they cease to do so, or else close feebly; the breathing becomes deep, regular, and as it were, mechanical; and the eyes generally turn upwards, as in sleep. When these phenomena take place, an operation may be commenced, without fear of its causing cries or struggles, or being felt by the patient. I do not always wait for the whole of the above symptoms to show themselves, but take into account, also, the length of time the patient has been inhaling, and the depth and number of inspirations; and I may remark, that I have not once been mistaken, with respect to the time when the operation might be commenced, without causing pain; consequently, an observant medical man will have no difficulty on this point. As soon as the operation is begun, I reduce the strength of the vapour very much, by turning the two-way tap to a certain extent. From what I have observed, I believe that from five to ten per cent of vapour in the air will keep up insensibility when it is once produced. So I turn the tap till the strength of the vapour is reduced to about twenty per cent, and let the patient breathe this diluted vapour and external air by turns, for a quarter or half a minute at a time, being guided all the time by the signs of returning sensibility, or of deeper insensibility, exhibited by the patient. This I consider preferable to making the patient breathe continuously from the apparatus. Towards the conclusion of the operation, the inhalation should be altogether discontinued. The administration of ether should never be delegated to non-medical person; consequently, if the operator has no medical assistant, as might happen in a small brig or schooner, which carries but one medical man, he must give the ether to the patient himself, having first got everything ready for the operation, and placed his patient in a position for it. Whilst giving the ether, he must direct his whole attention to it, and when the patient is made insensible, he will have to discontinue the ether, and transfer his attention entirely to the operation. When a person is rendered quite insensible by ether, he will usually remain totally incapable of feeling pain for three minutes, and sensation continues much blunted for some time longer. Now, a great number of surgical operations do not last longer than three minutes, and the most painful part of those that do last longer, is generally over within that time, so that, under these circumstances, the pain would generally be in a great measure prevented. in operations on the mouth, the ether has always to discontinued before they are commenced, yet the insensibility usually continues till they are completed: this was the case in an operation for hare-lip, in a little girl, to whom I gave the vapour of ether lately.
The pulse is generally accelerated during the inhalation of ether, often becoming very frequent; sometimes, however, it is but little altered. The pupil of the eye, in the earlier cases, frequently became dilated; but I have not observed this since I used the wide tubes, and I am therefore inclined to think that it depended on deficiency of air. There is sometimes struggling as the ether begins to take effect; but [552/553] this, when it does occur, passes off as the patient becomes totally insensible. During recovery, consciousness and ability to answer questions often returns before the sensibility to pain; and the patient will remark, perhaps, that he did not feel the operation, at the time that it is still going on, if he does not see it.
Common rectified sulphuric ether is unsuited for being inhaled, as it contains alcohol, which would irritate the air-passages. To prepare it for being inhaled, the spirit has therefore to be washed out, by s[h]aking it with water. When so prepared, it has a specific gravity of .720, that of distilled water being 1.000, and it boils at 100° at the usual pressure of the atmosphere. In this state it contains about one-tenth of its volume of water. This water can be separated by carbonate of potash, or by distilling it from quick lime, when its boiling point and specific gravity would be still further diminished; but I consider that it is more suitable for inhalation whilst it contains the water; since, if the air be dry, as it always is in frosty weather, and frequently also, under other circumstances, it will become saturated with aqueous vapour, from the water contained in the ether, as it passes over it, and will thereby be rendered less irritating to the lungs. For tropical climates, also, it is undesirable to diminish further the boiling point of the ether, as it will be sufficiently difficult to preserve it, even when it boils at 100°.
I have found the vapour of ether to succeed completely in preventing the pain in every instance in which I have administered it, and there have been no ill consequences of any kind attributed to the ether. On the contrary, the patients have generally recovered extremely well. The only disagreeable effects of any kind attributable to the ether, have been a little sickness or headach[e], and this only in a very few cases, although I have given the ether for a great number of operations in private practice, in addition to twenty-eight operations, most of them serious ones, in St. George's Hospital.
The pain endured by the bleeding sailor or soldier, wounded in fighting the battles of his country, is deeply deplored by every feeling mind; and a discovery which can prevent so much of it, as depends on the operations necessary to save his life, must be hailed as a great blessing, if it were for his sake alone; for the pain of a surgical operation is greater than that of the wound itself. Whilst the latter is instantaneous, and its approach unknown, the approach of an operation is seen, and its cuts are necessarily deliberate; and though ever so expeditiously performed, it seems of immense duration to the patient. The blessing would be great of merely preventing this pain, but I am firmly convinced that the exhibition of ether will be attended with the still greater advantage of saving many lives. A great part of the danger of an operation consists in the pain of it, which gives a shock to the system from which it is sometimes unable to recover. If an operation is performed during or immediately after an action, the wounded man suffers two shocks together--that of his wound and that of the operation, which although, singly, his frame might sustain, united, perhaps it cannot. If, on the other hand, a secondary operation, as it is called, has to be performed some time afterwards in the hospital, he is rendered nervous and more susceptible of pain by his illness and suffering. His wonted courage has perhaps been lost with his bodily strength; for the most courageous become often like children in illness, and the operation is looked forward to with dread, and the depression which he suffers from it is great. I believe that ether will give the surgeon a greater choice in selecting between cases for immediate and subsequent operation, for dread of the knife helps to cause and keep up the faintness and collapse, which often prevent the surgeon from operating at once. The ether and its apparatus will not add anything to the necessary baggage, for it will stand in the stead of a much greater weight of brandy. Before the operation, the knowledge of it will supply the cordial of hope. During the operation it will prevent faintness, which arises more from pain than loss of blood, which is seldom great. It usually acts, also, as a stimulant in itself; and I do not remember to have seen wine or brandy given in the operating theatre of St. George's Hospital more than once since January.
This opinion, that ether will save life, as well as prevent pain, is founded on experience; so far, at least, as experience has hitherto extended. Ether has been given in thirty-nine surgical operations at St. George's Hospital, nearly all serious ones; yet only two of the patients died; the remainder either left the hospital well, or are progressing favourably towards recovery; although besides the two that died, there were one or two others, concerning whom, at the time of the operation, but little hope was entertained of their recovery, the operation being undertaken to give them a slight prospect of cure, without it there being none. I have had the advantage of giving the ether in those of the operations, since the latter part of January, which have been performed at the usual hour for operations, amounting to twenty -- eight in number; and I will enumerate such of these as resemble the operations most frequent in the army and navy. Amputations are very numerous in the United Service. Of these there have been twelve-eight of the thigh, two of the leg, and two of the forearm. The two deaths which I mentioned were after amputation of the thigh; they took place some days after the operations. The patients were extremely weak and emaciated at the time they were performed; and I may observe, that two out of eight is below the usual number of deaths after this operation. Operations for necrosis somewhat resemble several undertaken for the removal of bullets and other extraneous bodies. Of these there have been four in the hospital, and the patients did extremely well.
Feigned diseases are a source of great anxiety to medical men, more especially to those of the United Service. It is humiliating to the medical officer, and a loss to the country, for him to be deceived by a man who is only pretending illness; yet to charge with feigning a man who is really ill would be a much more serious error; and the difficulties of distinguishing between real and pretended disease are sometimes very great. Lameness and deformities are diseases that are often feigned. Ether has solved the difficulty in which the medical men were placed in two such instances on the Continent. In one instance a man was suspected to pretend a deformity with projection of the spine. He was put under the influence of ether: his muscles became relaxed, and the deformity disappeared. In the other instance the man was suspected to feign stiffness of the hip-joint; but being rendered insensible, and his limbs quite relaxed, the joint was found to be anchylosed, and of course as immovable as before.
It has been stated in the medical journals, and I have frequently heard it in conversation, that oxygen gas is useful, and is sometimes required, to resuscitate persons under the influence of ether. Now, the trouble and care to be taken in the making of a gas are so great, that if oxygen gas, or any other gas, were required to remove the effects of ether, this agent would be effectually excluded from the field of battle, and indeed from practice altogether; except, perhaps, amongst the affluent, and the patients of large public institutions; but nothing of the kind is required; and if they were, I feel convinced that oxygen would not be the agent to remove the real effects of ether. In the beginning of February, I found that oxygen did not counteract the effects of ether on animals. In order to ascertain whether the effects of vapour of ether were due to its excluding, by the space it occupies, part of the oxygen of the air, I supplied, artificially, the oxygen displaced--and even placed animals in oxygen gas, mixed with vapour--and I found that etherisation took place quite as rapidly.* (*See the Lancet, Feb. 27th [which gave an account of Snow's presentation at the February 13, 1847 meeting of the Westminster Medical Society].) I was somewhat surprised, therefore, to find it stated in March, that oxygen gas was an antidote to ether; and I undertook fresh experiments, and found, that making animals breathe oxygen, after they had been rendered insensible by ether, did not restore them any sooner; that, indeed, they were often longer in recovering; and that one bird, very much under the influence of the vapour, died in the oxygen--an occurrence I never found to take place in the open air. Dr. Gull has arrived at the same result with respect to oxygen given after ether.
I may very properly be asked, how it is that oxygen is reported to have actually been found of service in restoring patients from the effects of ether. I can only explain it by suggesting that such patients are under the influence of asphyxia rather than of ether, since for a state of partial suffocation, oxygen is an antidote. Inhaling for a length of time, in the way practised with ether, without being allowed any external air, is perfectly new, and the caliber of tubes required for easy respiration in this way is greater than was supposed. But many of the ether inhalers offer such difficulties to the passage of air, by narrow tubes, valves, and orifices, and by obstruction from sponges or ether, that a person could not be made to breathe merely air through them, in the absence of ether, without being put in danger of suffocation in a few minutes.
A great deal that is very interesting might be said with respect to the way in which the vapour of ether probably produces insensibility. But I thought it better to confine my remarks to chiefly to practical points connected with the administration of it, in order that I might impart, as well as I should be able, to the medical officers of the United Service who might be present, all that I have been able to learn from the experience I have had on the subject; and in so doing, I trust that I have acted in accordance with the wish of the Council.
Return to John Snow Publications
26. "On deformity of the chest in children"
Source: Snow, John. Lancet 2, 31 July 1847, p. 137.[Letter to Ed.]
Snow's letter to the Editor bears on the following statements by George A. Rees, M.D., made in his paper, "On deformity of the chest in children." Lancet 2 (10 July 1847): 37-38.
"In the report of the proceedings of the Westminster Medical Society, contained in the Lancet of May 1st [1847], mention is made of a paper, read by Mr. Hird, "On Deformity of the Chest in Children, accompanied with altered Movement of the Ribs in Respiration," which is, though, most probably, without the author being aware of it, a transcript, to some extent, of a paper I sent, some years since, (1839) to the Medical Gazette.
It is singular that a paper was read before the Westminster Medical Society in 1841, by Dr. Snow, on the same subject, to which paper he referred at the late meeting, when speaking of Mr. Hird's cases, and which paper contained exact quotations from mine in the Medical Gazette; but without any mention of the source whence the quotations were derived--an omission I complained of at the time. I think Dr. Snow, when referring to Mr. Hird's cases, should have made the amende honorable by stating who really did first point out these cases, and not have been content with the statement, 'that this kind of deformity had been noticed by writers in this country' It is true, priority of remark in so simple an affair is little to boast of, nevertheless, it is well to cultivate in trifles that strict sense of liberality and justice which should be the guide of professional conduct--a want of which I believe has mainly contributed to the present disorganized state of the profession; and it is necessary to remember, that they who have made no great discoveries are the more captious about what they may really call their own.
. . . . . . . . . . . .
Dr. Snow is perfectly correct in stating that these cases are usually combined with more or less abdominal enlargement; but in considering the deformity, the result of such enlargement, he has, in my opinion, mistaken the effect for the cause" (37).
Snow responded as follows:
To the Editor of the Lancet.
Sir,--I feel it my duty to reply to a very grave, though totally unfounded, charge made against me by Dr. G. A. Rees in the last number of the Lancet [actually, three issues previous to this one, which permits us to date the composition of his letter sometime during week of 10-16 July]. He [Rees] says that a paper read by me to the Westminster Medical Society in 1841 contained exact quotations from a paper of his in the Medical Gazette, but without any mention of the source whence the quotations were derived. The very reverse of all this is true. I referred to his paper in the most handsome manner, stating his name, and the date and place of it, but made no quotations from it, as any one may ascertain. My paper was published in the Medical Gazette [vol. 28] of April 9th, 1841. The title of it was, "On Distortions of the Chest and Spine in Children, from Enlargement of the Abdomen" [see p. 115 on Rees]. Dr. Rees' communication was entitled, "On Deformity of the Chest in Young Children, from Disease of the Lungs." How any extract from his paper could have served my purpose it is not easy to conceive. In his former complaint to which he alludes, he did not accuse me of making exact quotations, but chiefly confined himself to endeavouring to show that my cases were of the same nature as his own, and that they did not depend on enlargement of the abdomen. He did, indeed, make an insinuation, for which he ought to have apologized after my reply, which appeared in the following number of the Lancet -- that of April 10th, 1841, at page 112. As Dr. Rees has withdrawn his opinion, that the change which he met with in the lungs was the result of inflammation, and as he now admits that there is usually abdominal enlargement, I am inclined to believe that his cases are of the same nature as those which I described. In the case detailed in my paper, the greater part of the lungs was collapsed, and void of air. I offered no explanation then of the cause of this, but I now consider that the deformity in question, after it attains a certain degree, may cause compression of the lungs, and have the same effect on them as a pleuritic effusion would have, and thus terminate life. In my opinion, then, the condition of the lungs, which Dr. Rees considers to be the cause of the deformity, is an occasional consequence of it. When deformity is the result of disease of the lungs, it does not affect both sides of the chest alike.
On the late occasion I alluded again, in the Society, to Dr. Rees' paper, and stated his opinions, previous to mentioning my own paper, although if I had not done so, but had included him amongst authors in this country in the abbreviated language of the report, and had so passed from Dupuytren to my paper in the Society, on which I was speaking, he would have had no ground for complaint. As to my stating who really did first point out these cases, Mr. Hird had already done that in mentioning Dupuytren, whose cases, now that Dr. Rees has just alluded to them for the first time, he tries to show differ from his own, though to me that is not apparent.
The letter I am now answering commences by a statement, that Mr. Hird's paper was a transcript, to some extent, of one by Dr. Rees. I feel assured that Mr. Hird knew nothing of that paper till I alluded to it. Dr. Rees, indeed, says, a transcript, "most probably without the author being aware of it." Now, it so happens that Mr. Hird wrote nothing, and read nothing, but only related a case or two, and made some remarks on them. But supposing that he had really written and read a paper, as he said that he had intended, and that, in some peculiar state of unconsciousness, he had made a "transcript to some extent" of Dr. Rees' paper, how could that gentleman be aware of such transcription, as the supposed paper has not been published, but only, as he says himself, "mentioned?"
I shall be much obliged by the early insertion of this reply; and I remain Sir, your obedient servant,
Frith-street, Soho-square, July, 1847.
John Snow.
 27. On the inhalation of the vapor of ether in surgical operations: containing a description of the various stages of etherization and a statement of the result of nearly eighty operations in which ether has been employed in St. George's and University College Hospitals.
27. On the inhalation of the vapor of ether in surgical operations: containing a description of the various stages of etherization and a statement of the result of nearly eighty operations in which ether has been employed in St. George's and University College Hospitals.
Source: Snow, John. London, J. Churchill, Oct. 1847, 88 pages. (PDF only)
Return to John Snow Publications
28. "Dr. Snow on the effects of ether vapour"
Source: Snow, John. London Medical Gazette 40, 12 November 1847, p.859, [Letter to Ed.].
Sir,--I shall be obliged if you will correct an error in a quotation from my work "On the Inhalation of Ether," in the review of it which you have done me the honour of making in your last number. At page 813, in the first column, quoting from page 39 of the book, you have omitted the word "always." Instead of "It is not possible to avoid having the breathing somewhat stertorous," it should be, "It is not always possible," [etc.]
That the omission is an important one, is evident from the circumstance that it has caused you in the sentence immediately following the quotation to give an account of the efficacy of ether directly opposed to the facts I endeavoured to explain. For, whilst in the cases in which ether is well administered the patients show no signs whatever of sensation, much less of "perception of pain," yet in these cases simple snoring is quite an exception, and a state of breathing that can be called stertorous is still more rare.
In the first quotation, taken from page 2, there is an omission of nearly two lines; but this mistake is of less consequence.
Your obedient servant,
John Snow.
Frith Street, 8th November.
Return to John Snow Publications
29. "On the inhalation of chloroform and ether, with description of an apparatus"
Source: Snow, John. Lancet 1, 12 February 1848, pp. 177-180.
By John Snow, M.D.
In January last I laid before the Westminster Medical Society an apparatus which supplied the means of regulating the proportions of ether vapour and of air during inhalation. By means of this inhaler, it was, I believe, first ascertained that every patient might be rendered insensible by ether, and that all failure must arise from inefficient means of administering the vapour, and not from any idiosyncrasy of the patient. After observations for a few months of the exhibition of ether in this uniform way, I was enabled in the course of last autumn to submit to the profession a description of etherisation divided into degrees, which I still consider to be correct, and to be equally applicable to the effects of chloroform, and other agents of a similar kind.
I divide etherization into five degrees, which may be called degrees of narcotism. The division was made according to symptoms which may be observed before an operation begins, leaving out of the classification the immunity from pain, which can only be ascertained during the operation, and which, curiously, does not correspond uniformly with the state of the patient in other respects. In what I called the first degree, there is exhilaration, or altered emotions and sensations of some kind; but the patient still retains consciousness and volition. In the second degree, the mental functions may still be performed, but only in an irregular manner; there may be ideas of a dreaming kind, and voluntary efforts in accordance with them, or the patient may be passive. When mental excitement occurs, it is chiefly in this degree, in which the functions of the cerebral hemispheres seem to be impaired, but not yet abolished. In the third degree, those functions appear to be totally suspended, but those of the spinal cord and its nerves still continue to some extent; the orbicularis palpebrarum may contract when the eyelids are touched; there may be other involuntary motions resulting from external impressions, and groans or cries may occur, but no sounds of an articulate kind. There are also sometimes, in this degree, involuntary muscular contractions as an effect of the vapour--apparently a kind of excitement of the spinal cord. In the fourth degree, no movement is [177/178] obvious, except that of respiration, which is unaffected by external impressions, and goes on regularly, though often with snoring or even some degree of stertor. It would seem that the whole of the nervous centers are paralyzed by the vapour except the medulla oblongata. In killing animals with vapours, I have observed the breathing to be difficult, or feeble, or otherwise impaired, before it finally ceased; this stage I call the fifth degree. There can be no doubt that these degrees of narcotism correspond with different proportions of vapour which are dissolved in the blood at the time--proportions which I hope to be able to determine. A certain quantity of vapour disturbs the functions of the cerebral hemispheres; an additional quantity appears altogether to suspend these functions, and to impair those of the spinal cord, and probably of the cerebellum; a still larger quantity to suspend their latter functions, but to leave the medulla oblongata more or less unaffected. As the vapour escapes from the blood by the lungs, its effects go off, the patient passes from the fourth degree to the third, from that to the second, and so on, if the inhalation be not renewed.
It is seldom possible to perform an operation without signs of pain unless the narcotism is carried as far as the third degree, although, if performed in the second degree, the patient, being unconscious, might not remember the pain, memory being the continuance or revival of knowledge or consciousness, which is something superadded to mere sensation, and not the same thing. Some cases have indeed been met with, in which it is stated that patients felt no pain, although they had never lost their consciousness. I have not seen any such case. I do not, however, deny the possibility of it, but I am inclined to think it a mistake, and to believe that in these cases the patients had been unconscious without knowing they had been so, and had recovered their consciousness whilst still inhaling, before the operation began. My reasons for believing so are, that as vapours are often administered, the strength of them diminishes as the process goes on, by the cooling of the sponge or other apparatus, or by the liquid becoming exhausted, thus affording the patient an opportunity to recover; that on recovering, even after a long operation, the patient often asserts that he is not yet insensible, until he finds proof of his error; and that I have often known patients to be conscious during some part of an operation without feeling it, after they had been unconscious previously.
It is, then, generally necessary to carry the effects of chloroform or ether to the third degree, and sometimes to the fourth degree, to be certain of avoiding the pain of an operation; but whilst patients are recovering from the effects of the vapour, there is a greater immunity from pain, with the same degree of narcotism, than when they are first getting under its influence--consequently, it is seldom necessary to keep up the effect even to the third degree, especially with ether, which I consider has on an average a greater anæsthetic effect, in proportion to the narcotism, than chloroform. If some persons consider the anaesthetic effects of the new agent which Dr. Simpson has introduced to be superior to those of ether, it is probably because they have carried its effects further than they did those of ether--perhaps further than they had the power of carrying the latter with the means they employed. After narcotism has been carried to the fourth degree, the patient is nearly always insensible to the operation in the third degree; and when insensible in the third degree, generally remains so when narcotism has diminished to the second degree. With ether, indeed, it was frequently observed that the patient remained insensible to the knife after he had recovered his consciousness of surrounding objects, and could even talk rationally. This I have never yet observed with chloroform, although I have taken notes of fifty cases. This curious circumstance in the effects of ether has, I believe, never been explained. I have an hypothesis to offer in explanation of it. I have looked over my notes of cases of etherisation, and have found that the instances in which the insensibility to the operation outlasted the unconscious state, with only one exception, occurred in subjects under twenty-five years of age.
This peculiarity, then, must depend on something in which the young differ from or exceed the old. Let us take the first characteristic difference between the opposite periods of life,--the rotundity and smooth-flowing outline to which youth owes its beauty and its chief feature: On what do they depend? They depend on the greater quantity of extra vascular liquor-sanguinis or lymph in the cellular tissue, connected with the more active nutrition which is going on. Next let us consider what are the parts whose functions are necessary to sensation,--doubtless the trunks and peripheral expansion of the nerves as well as the nervous centers. Now, M. Flourens, I think it is, has ascertained that ether applied directly to the nerves paralyzes them. The following is the way, then, in which I explain this curious enigma: --
The narcotic vapour dissolved first in the blood passes in a little time by exosmose through the coats of the capillaries into the extra vascular fluid, immediately bathing the nervous fibrillæ, so as to establish an equilibrium between the quantity in the blood and that in the lymph of the tissues. On the other hand, whilst the vapour is leaving the blood by the lungs, the current is greatest in the opposite direction--namely, into the vessels; but this process must occupy some time, especially in young subjects, in whom the quantity of liquor sanguinis, free in the tissues, is considerable. Now there is but very little lymph in the brain, cerebellum, and grey matter of the cord; the blood, both liquid and globules, in these parts is chiefly contained in the vessels in the young as well as in the old. Therefore, as the vapour leaves the blood, the central nervous matter, and particularly the cerebral hemispheres, escape from its paralyzing influence at a time when the peripheral expansion of the nerves, bathed in the not yet de-vaporized liquor sanguinis,--especially in the young,--remain incapable of receiving the impressions which constitute the first link in the changes necessary to constitute a sensation.
Chloroform, which is but very little soluble in water, probably does not permeate the coats of the capillaries by exosmose so readily as ether, and hence, perhaps, the reason why it never exercises its anæsthetic effects after the nervous centres have altogether escaped from its influence. The complete recovery of the mental functions before the return of common sensibility is but an extension, to a greater degree, of the almost constant phenomenon of the insensibility being greatest during recovery, as compared to the narcotism, and consequently the above explanation applies to ordinary cases in a minor degree, and to chloroform as well as ether.
Chloroform has certainly the advantage over ether of being less pungent, and of being, therefore, more readily inhaled. It has also one or two advantages not named by Dr. Simpson; it occupies less space, and therefore excludes less of the air that the patient breathes, as I stated in November. It has another advantage, in not exciting a profuse flow of saliva, as ether sometimes does, which is very troublesome; and when the patient is on his back, as is the case usually in important operations, the saliva, coming in contact with the glottis, causes coughing at a time when the patient would not cough from the pungency of the vapour. But some of the properties of chloroform which Dr. Simpson calls advantages as compared to ether I do not appreciate altogether as such. One is its greater rapidity of action. Ether required four or five minutes on an average to produce the full chirurgical degree of its effects on the adult. Now it might be desirable to shorten this time to a certain extent, but not, in my opinion, to less than two minutes, not only to give ample time to observe its effects, but also on account of a property in the action of this class of vapours, which has not, that I am aware, been alluded to; I mean, the cumulative property they have. They act, it is true, with great rapidity, yet, to become imbibed by the blood, to pass through the heart, and reach the nervous centres, must occupy a little time, and I have often observed the insensibility to increase for twenty seconds after the inhalation has been left off. I have experienced this cumulative property myself to extend to twenty seconds, by taking a few inspirations of vapour, leaving off, and looking at a watch; consequently, I like to have about six times this period, or two minutes, for producing complete insensibility; but when administered in the way Dr. Simpson recommends, chloroform often produces its full effects in much less time than this. He himself observes that he has seen a strong person rendered completely insensible by six or seven inspirations of thirty drops of it. Danger, it is true, may probably be avoided by putting a limited quantity on the sponge or handkerchief, but then the full effect might not be reached, especially as it cannot be determined how muxh the patient inhales of what is put on, and the dose would have to be repeated, so that this plan is not very applicable in surgery; and Dr. Simpson himself recommends that "one or two teaspoonfuls of the chloroform should be at once placed upon the hollow of a handkerchief, and immediately held to the face of the patient." He adds that "generally a snoring sleep speedily supervenes."
What he is pleased to call a snoring sleep I should denominate the fourth degree of narcotism, which is separated only by one degree more from a total cessation of respiration. I do not consider that snoring, or even some degree of stertor, is alarming or injurious, but I think it advisable not to induce this state with such great rapidity, lest the narcotism should [178/179] proceed a degree further on account of the cumulative property of the vapour after it is discontinued. Let us look at this matter in another point of view. 100 cubic inches of the vapour of chloroform contain 128 grains of the liquid. Half of this quantity is enough, if inhaled within a minute or two, to produce the most complete insensibility; the whole quantity, if inhaled rapidly, might undoubtedly cause death; for I have observed that animals may generally be killed by half as much more vapour than will produce narcotism to the fourth degree. If, for instance, an animal is rendered completely powerless in two minutes by vapour of a certain kind and strength, death takes place by continuing it for another minute; if rendered powerless in one minute, then it dies in about half a minute more. Now 100 cubic inches of vapour of chloroform may be contained in 800 or even in 500 cubic inches or air. When air is saturated with the vapour of chloroform at 60°, 800 cubic inches contain 100 of vapour, at 70°, 500 cubic inches contain the same quantity; so that the 128 grains of chloroform might all be inhaled in four or five deep inspirations, and, consequently, a person breathing deeply might inhale a fatal dose of chloroform in a quarter of a minute. This should be borne in mind, especially by those who recommend that patients should breathe deeply when inhaling. I always tell persons to breathe quietly, and when I find, during the inhalation of chloroform, that the inspirations are deep, I open the valve for admitting the external air to further dilate the vapour. I seldom induce total insensibility in less than two minutes, and occasionally take three minutes. The exhibition of the chloroform requires great care when it has to be repeated to keep up insensibility in a patient already under its influence, during an operation; and under all circumstances, it will require additional care in summer, except an apparatus with a cold water bath is used.
I for some weeks employed the same apparatus in the exhibition of chloroform which I had used for ether; but afterwards I contrived a more portable one, still employing this face-piece, which I have used with ether since June last. The sides are composed of thin sheet lead, which can be moulded to fit the patient's features; and the expiratory valve turns on a pivot, so that it can be moved aside from the opening it covers, and external air admitted at the beginning of the inhalation, and at any other time if required.
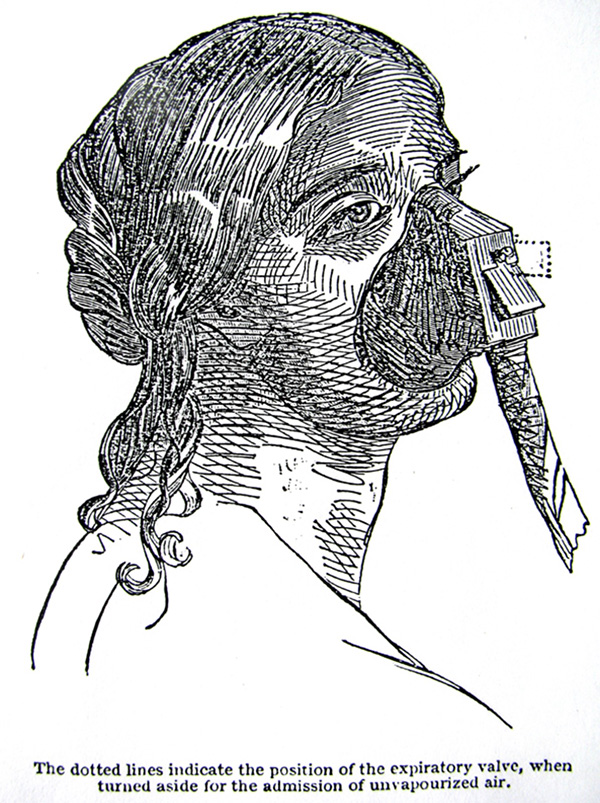
Mr. Hawkesley was, I understand, the first to invent a face-piece containing flexible metal, and including both the mouth and nostrils, admitting of respiration by both; but a face-piece contrived by Mr. Sibson, of the Nottingham Infirmary, was the one which suggested this, and I got it to its present form by several successive alterations, and in this shape it is extensively used. Mr. Robinson had it adapted to his ether inhaler, and since chloroform was introduced, he has put a sponge into it, and made some alterations in the valves, and thus formed an inhaler out of it for chloroform, which very properly goes by his name. One contrived by Mr. Coxeter, also consists of this face-piece with some additions.* (*It was described in the last Lancet, p. 114.) In this inhaler, which I now use, I retain the water-bath, but of smaller dimensions, the caloric absorbed in the evaporation of chloroform being very much less than in the case of ether. I never employ water of a higher temperature than 60°. The inhaler is suspended to the face-piece by a short piece of elastic tube, merely to allow of its being applied in all positions of the patient. The bibulous paper which absorbs and gives out the chloroform, only extends half-way up the cylinder, so that there is little or no loss by spontaneous evaporation, the air saturated with vapour being rather heavier that the air above.
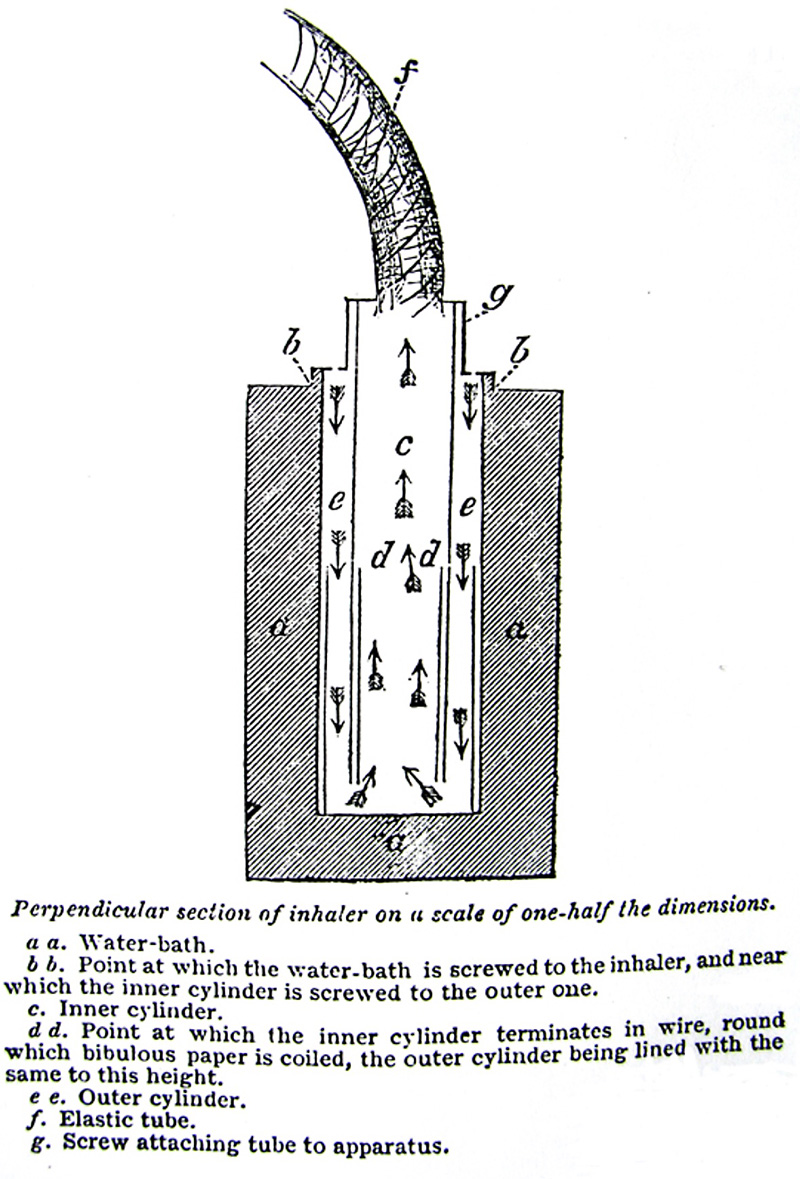
I consider that, on the whole, chloroform is superior to ether for adults, and that we are greatly indebted to Dr. Simpson for the introduction of its use. For children I prefer ether to chloroform, when the choice is left to me, on account of the greater rapidity of action of these vapours on them, as I stated to the Society a month ago, although I have administered chloroform several times to young children--one of them aged only ten months--and with perfect ease, safety, and success. I consider the less powerful agent of the two, however, sufficiently strong for very young patients, and this chloroform inhaler serves very well with the small face-piece for exhibiting it to them.
Children are brought under the influence of ether, sufficiently for an operation, in two minutes, and I think it impossible for the imagination to conceive any anæsthetic agent more mild and efficient than ether is in its effects on children--a less degree of narcotism than in the adult producing an immunity from pain, and the liability to excitement being absent. The ether, however, requires to be given to them with an apparatus, by which the vapour can be introduced into the air they are breathing, in the most gradual way; otherwise the pungency of the vapour can be introduced into the air they are breathing, in the most gradual way; otherwise the pungency of the vapour, when suddenly admitted makes them hold their breath, which is the case with chloroform also when given to children on a sponge or handkerchief. If it is desirable, as I believe it to be, that we should have an agent which can be safely and generally [179/180] administered in this way to children, to women in natural labour, and for tooth-drawing, and minor operations, by persons of no special experience in the matter, it should be something much less powerful than chloroform, and less pungent than either of these vapours.
On account of its being in rapidity of action between chloroform and ether, I requested permission to give benzin in St. George's Hospital lately. It was made for me by Mr. Bullock, by distilling benzoic acid with slaked lime; it consists of six atoms of carbon and three atoms of hydrogen, and is the same thing as the bicarburet of hydrogen discovered by Dr. Faraday, and obtained by him from condensed oil gas. It succeeded very well in four cases of tooth-drawing without any disagreeable effects, and in an amputation below the knee it totally prevented the pain, and was followed by no ill effects: but being pushed rather further than in the other four cases, the patient, a women, had some convulsive tremors for about a minute, which I consider as a peculiar result of the vapour when its effects reach the third degree, as the same vapour caused the same symptoms in two white mice and in some guinea pigs, and I never saw similar effects from ether or chloroform. Benzin, consequently, does not seem suited for severe operations. It has an aromatic odour; about the same quantity is consumed as of chloroform. About one drachm was used in the case of tooth-drawing, and two drachms in the amputation, but being less volatile it does not act so quickly.
The property of totally preventing pain in severe operations, and on other occasions of acute suffering, is most valuable and important, yet these anæsthetic vapours sometimes confer still greater benefits.
I administered the chloroform, several weeks ago, to a gentleman, aged fifty-eight, on whom Mr. Coulson performed the operation of lithotomy. This patient had been suffering from diseased bladder for more than twelve months, and the operation was recommended and submitted to as the only means of affording a prospect--and that but a doubtful one--of recovery. He was so nervous and irritable, and the bladder so sensitive, that he could be sounded only with the greatest difficulty. Sir B. Brodie and Mr. Sams, of Blackheath, the usual attendant of the patient, were present at the operation, which was extremely difficult and protracted on account of the calculus, which was of the fusible variety, being large and breaking whenever it was grasped with the forceps. It occupied three quarters of an hour, the patient, of course, being kept perfectly insensible the whole time. Sir B. Brodie remarked that he had only seen one case of lithotomy so difficult, and he, Mr. Coulson, and Mr. Sams, expressed their conviction that the operation could not have been performed except for the insensibility produced by the chloroform.
The patient gradually and quietly recovered his consciousness in the course of a quarter of an hour after the operation was completed, and is going on well, but requires to have his bladder washed out, on account of phosphates and mucus in the urine, and he inhales the chloroform at his own request on these occasions.
I administered the chloroform also lately to a gentleman, to enable Mr. Henry Charles Johnson to reduce a compound dislocation, backwards, of the last phalanx of the thumb, which he had previously endeavoured to reduce without success, as the patient could not bear the attempt to be continued. When insensible, the dislocation was speedily reduced. Mr. Gaisford, of Brompton, was present.
I am not aware that any disease, or any state of the general health, forbids the inhalation of ether or chloroform, and it is fortunate that the least favourable subjects for inhalation are those least likely to require it--viz., persons in robust health. There is not, however, any serious objection to it in such persons; but there is occasionally a little difficulty, as they are more liable to excitement in the second degree, and to rigidity and struggling in the third degree of vaporous narcotism. It has been said, and I stated the same opinion myself in the Medical Gazette in March of last, that disease of the heart or lungs, to any notable amount, contraindicated inhalation. I do not now deny this, but I am of opinion, that when persons so situated require a painful operation, inhalation of the vapour would be less liable to do mischief than the pain, or even the anticipation of it. The inhalation of chloroform quickens the circulation somewhat; that of ether, still more; and therefore I think the former would be preferable when there is any affection of the heart or lungs. I have given both vapours to patients with diseases of these organs, and have seen no ill consequences.
Mr. Thomas Wakley, after detailing an extensive series of experiments in the Lancet, (present vol. No.1,) draws the conclusion, that ether, and more especially chloroform, cause congestion of the heart and lungs during inhalation, and therefore would be dangerous in affections of these organs. He arrives at this opinion from the congestion found in some of the animals which were killed. I have met with the same congestion in animals destroyed by these vapours, under certain circumstances, but I do not consider it any proof that congestion exists during inhalation, confined within safe bounds. The arteries are nearly always found empty after death, but we do not conclude that they are empty during life. The congestion of which I am speaking arises from the circumstance, that in many instances in which animals are destroyed by these vapours the respiration ceases whilst the circulation is still vigorous: they die, in fact, as if by asphyxia; and it is on this account that, to avoid danger in exhibiting vapours, we should attend to the state of the respiration, rather than the pulse.
Frith-street, Soho. Jan 1848.
Return to John Snow Publications
30. Remarks on the fatal case of inhalation of chloroform; including additional explanations from Dr. Meggison"
Source: Snow, John. London Med. Gazette 41, 18 February 1848, pp. 277-278.
BY John Snow, M.D.
An instance having occurred in which the application of chloroform has ended fatally, it is highly desirable to arrive at a correct knowledge of the cause of this unfortunate result, as well that a repetition of it may if possible be avoided, as for the satisfaction of scientific inquiry. And since the opinion I have formed differs from that of the medical gentlemen who gave their evidence at the adjourned inquest, I have thought it necessary to state my views of the case.
Sir John Fife attributes the fatal effect of the chloroform to peculiarity in the constitution of the young woman, which could not previously have been foreseen. This would necessarily invest the inhalation with some degree of danger, however small, and would entail some anxiety on both the operator and the patient. My view of the matter holds out more hope for the future. I look on the result as only what was to be apprehended from the over-rapid action of chloroform when administered on a handkerchief, as recommended by the greatest authority respecting it--Dr. Simpson, the author of its use,[--] and consider that danger may be avoided by adopting another method. I have observed that the effects of the vapour may accumulate for about twenty seconds after the inhalation is discontinued;* and this accumulation will be the more formidable in proportion to the quantity of vapour that is being inhaled at the moment, and the velocity with which the symptoms are being induced. (*See Med. Gaz., Jan. 14. Two days after I made the statement respecting the cumulative property of vapours in the Westminster Medical Society, viz. Jan. 10, M. Sédillot remarked, in the Academy of Sciences, that with chloroform the pallor, smallness of pulse, weakness of respiration, and coldness of the skin, sometimes increase after the inhaler has been removed, in an alarming manner.) The entire effects of the vapour, when carried to a fatal issue, might be divided into five pretty equal portions, according to the degrees of narcotism I suggested. Now, in the case under consideration, when the girl had inhaled for about half a minute, there was rigidity of the arms; this would indicate that she was in the third degree; and supposing that the cloth was removed at that very instant, if the chloroform was not previously expended, and if the vapour was inhaled of the same strength during the thirty seconds, its effects might increase at the same pace for twenty seconds longer; and at the end of fifty seconds from the commencement she would be in the fifth degree of narcotism, in which "respiratory movements are more or less paralysed and become difficult, feeble, or irregular."
I wrote to Dr. Meggison for additional information to that given in the report of the inquest on one or two points. He has obligingly answered my inquires, and also given me leave to make use of his reply. The following is part of his note: --
"With respect to your queries,--1st, As to the nature of the breathing after the inhalation was stopped? 2d, How long did the patient breathe after the removal of the cloth? 3d, As to the moan spoken of. The 1st I can reply to satisfactorily. The breathing was at first somewhat quicker and stronger; then, immediately preceding the moan spoken of, it became very rapid, and ended in what the witness Rayne called a moan, which was a prolonged forced expiration, or rather splutter,--breath, saliva, and tongue, being forced out at once, as it were. The sound was similar to the expiration in epilepsy or hysteria. The remaining expirations and inspirations were exceedingly feeble and few; but I could not speak confidently on the subject, being very much agitated at the time. 2d, The breathing after the removal of the cloth continued upwards of half a minute, but how much I cannot say, having put my watch in my pocket on seeing her move. 3d, The moan, as I have said before, did not appear to me such, but a splutter."
The above explanation make it still more evident that the effect of the chloroform greatly increased after the inhalation was discontinued.
The quantity employed -- about a fluid drachm -- was, in my opinion, sufficient to account for the result, even supposing that one-half evaporated into the apartment and only the other half was inhaled; for, in using an inhaler by which little or no vapour escapes except to enter the lungs, I find that a fluid drachm is sufficient to induce narcotism to the fourth degree in a shout man, when the exhibition of it occupies two or three minutes, and about half as much in a young person of the probable size of this patient; but when the vapour is inhaled rapidily, a given quantity produces a greater effect; and Dr. Simpson remarks, that he has "seen a strong person rendered completely insensible by six or seven inspirations of thirty drops of the liquid."
Whenever I have had the opportunity, for the last two months, I have cautioned the profession against the too rapid action of chloroform when given on a handkerchief or sponge. In objection to what I am saying, the numerous cases in which it has been safely administered in thus way may be pleaded, notwithstanding one fatal case. I may mention, however, that I have been privately informed of three or four cases in which the medical man was greatly alarmed for the life of his patient. One case also of this kind occurred in Guy's Hospital, and was related by Dr. Gull in the Medical Gazette, in the latter part of last year; and I believe that many patients have owed their safety to the rapid loss of the chloroform by evaporation.
If it were correct that some individuals require to inhale several drachms before becoming insensible, there would be reason to believe that others would be unusually sensitive to its effects; but with chloroform, as with ether, I have met with no such exceptions, and I have not heard of any when the vapour has been so administered that it was inhaled without loss. Under these circumstances, the quantity consumed in producing insensibility always appears proportionate to the size and probable weight of the patient, if the inhalation is not interrupted; and the time required to induce insensibility proportionate to the strength of the vapour and the activity of the respirations.
Although many of the inhalers in use are very faulty, I consider that they are safer than the handkerchief. They are liable to the objection that they obstruct the respiration, by causing the air to pass through sponges; but with a limited supply of air the chloroform is necessarily limited also, as its vapour, having no existence in a separate state at common temperatures, can only be inhaled with the air. To give chloroform in surgical operations, an instrument should be used which offers no obstruction to respiration, and by which the proportion of vapour in the air can be regulated; and those who have but a handkerchief or sponge had better use ether, which I consider has not yet been known to cause death, until other narcotic vapours may be introduced.
In the case under consideration, the fatal result should be attributed to the action of the chloroform on the nervous centres having extended so far as to put a stop to respiration; and I cannot agree in the opinion of Sir John Fife, that the immediate cause of death was congestion of the lungs, an affection which could only have caused death in a somewhat tedious and not in a sudden manner, and which ought undoubtedly to be looked on merely as a consequence of the mode of dying, and as an indication that the heart continued to inject blood into the lungs after oxygen was no longer admitted to facilitate its passage through the capillaries. In certain instances this is the case in animals killed by chloroform, whilst in other instances, which I shall endeavour to explain in a future communication, the respiration and circulation seem to cease together.
Unless when the patient coughs or holds his breath, there is no tendency to congestion of the lungs during the inhalation of chloroform judiciously administered; for the free respiration and undiminished volume of the pulse, shew that the blood passes freely through these organs. Dr. Glover, I am aware, detected obstruction to the pulmonary circulation during life, by the hæmadynamometer placed in one of the arteries of an animal under chloroform; but in that instance the chloroform had been injected into the veins; and any substance that will not dissolve in the blood causes mechanical obstruction to its passage through the lungs: atmospheric air, the presence of which in the lungs is necessary to their circulation, when injected into the veins arrests it.
I would observe in conclusion, that I attribute the blame to no one; for Dr. Simpson cannot be blamed if, in conferring on us the benefit of chloroform, his instructions did not issue, like Minerva from the head of Jupiter, perfect and incapable of improvement.
Frith Street, Soho, Feb. 18th.
Go to Group 3  (# 31-45)
(# 31-45)
Click to return to Stream 1 - d: John Snow's Publications
Click to continue to Stream 1 - e: Memoir of his friend Benjamin Ward Richardson"
