d12: John Snow's Publications - Group 12 (# 88-102 )
Return to John Snow Publications
88.
"Chloroform in London and Edinburgh"
Source: Snow, John. Lancet 1, 27 January 1855, pp. 108-09, [Letter to Ed.].
To the Editor of the Lancet.
Sir,--I shall be much obliged if you will allow me to make a few brief remarks on the able lecture of Mr. Syme on the subject of chloroform in the Lancet of to-day. I have the happiness to agree with Mr. Syme in the most important points on which he has treated, and if that were all, I should not deem it necessary to address you, for I feel sure that the opinions of this able surgeon would have their due weight, without being endorsed with anything I have to say. It is because I differ from Mr. Syme in some particulars, and because I consider that, in speaking of London as a whole, he has unintentionally done an injustice to certain persons and certain institutions, that I take the liberty of addressing you.
In the first place, however, I wish to state, that I am very much gratified with the remarks of Mr. Syme respecting the disease of the heart. There has been for some time such a strong current of opinion, both in the profession and amongst the public, against the administration of chloroform where there is disease of the heart, that I have been almost deterred from repeating my convictions on the subject so strongly as I could wish, for fear of being thought rash and eccentric, and having my small sphere of usefulness thereby curtailed. If we leave out of view two patients who died suddenly whilst beginning to inhale, and before they could have been affected by the chloroform, and one or two others where the death was most likely unconnected with this agent, I believe that the patients who have died whilst inhaling chloroform have possessed, on the whole, as sound a state of the heart and other vital organs as those who have inhaled it without accident. Persons who require surgical operations are far from being of sound constitution; and this has been especially the case in my own practice, as patients are often sent to me by medical men who hesitate, or decline altogether, to sanction the use or chloroform on their own responsibility. I have found, by very careful observation, that the pain of an operation, disturbs the circulation much more, and puts a feeble heart to a much more severe test than chloroform when carefully administered. I have given chloroform, with the most satisfactory result, to very many patients offering all the symptoms of fatty degeneration of the heart in a very marked degree, as the arcus senilis of the cornea, a feeble, intermitting pulse, and liability to faint. The only patient I have had the misfortune to lose whilst inhaling chloroform, was, indeed, an old gentleman who exhibited the above symptoms in a marked degree. He died as I was proceeding to give a little fresh chloroform, on account of signs of returning sensibility; and I am far from being satisfied that this agent was the cause of his death. The heart was afterwards found to be more degenerated than in many cases where the patient dies suddenly from a very slight shock or exertion, or even without apparent cause.
If the induction of anæsthesia could only be adopted on the strong and robust, it would be a very lame discovery; for persons of feeble or damaged constitution, young children, and the aged and infirm are they who most require to be saved from pain; and, again, if the practice could only be advised for extremely painful operations, the patient would be necessarily impressed with an idea of its essential danger, and the greatest benefit connected with the discovery, that of preventing the anxiety and mental anguish arising from the anticipation of an operation, would be altogether lost.
In speaking of London as a place where deaths from chloroform have occurred, and Edinburgh as a place where they have not, Mr. Syme seems entirely to overlook the relative size and population of the two places. When these circumstances are taken into account, the mortality from this cause seems to be pretty equal. At the time the death in Edinburgh occurred, it rendered the mortality of that place higher than in London, and if another death were unfortunately now to occur in Edinburgh, that place would again have the undesirable pre-eminence. If we are reminded that patients go to Edinburgh from a distance, it must be recollected that private patients come here from the East and West Indies, Canada, and Australia, expressly for operation, and that hospital patients come from nearly all parts of England and Wales. Chloroform is also administered here in certain cases where the Edinburgh surgeons refrain from its use, as in lithotrity and the removal of tumours of the jaw.
If Mr. Syme alludes only to his own department of the Infirmary, he should not contrast that with the whole of London, for there is at least one hospital here, where a great number of operations are performed, and where no such approach to an accident has occurred as those which Mr. Syme speaks of as having happened in his own practice. In King's College Hospital the breathing of the patient never becomes difficult, or ceases, and it has never been necessary to pull out the tongue with the artery forceps. I have seen faintness in a few patients in this institution from loss of blood during the removal of large tumours with extensive vascular connexions, but I have never had reason to be alarmed on account of the effects of the chloroform. The dangers Mr. Syme has incurred have no doubt arisen from his maxim, that "the more rapidly the chloroform is given the better," and I feel certain that under this practice the artery forceps will not always avail to prevent accident. In St. George's Hospital a patient died suddenly whilst beginning to inhale, without being brought under the influence of chloroform, but I believe that there has been no approach to an accident in that institution from the real effects of chloroform. Mr. Syme attributes the supposed greater mortality from chloroform in London to a difference in the mode of its administration, but the real equality in the mortality in the two metropolitan towns is, I think, well explained by the general resemblances of the methods of exhibiting it in both places. In nearly all cases where accidents have happened in London, the Edinburgh method of exhibiting the chloroform was followed pretty closely. If a piece of lint has been used instead of a handkerchief, or the worsted glove of a dresser mentioned in Professor Miller's pamphlet, it was, no doubt, because such a slight deviation was not thought of importance.
It is quite true that in certain quarters too great a reliance has been placed on the state of the pulse in administering chloroform, but that is by no means universally the case in London. Indeed, I have only seen a single case in which the person administering the chloroform seemed to rely for his information chiefly on the pulse. I have never heard of an instance where the chloroform was continued when the breathing was stertorous, although of course such an event might occur in a place as large as London without my knowledge. Usually the inhalation is discontinued here as soon as the common sensibility is abolished, without the breathing being rendered stertorous at all. Mr. Syme says that chloroform is given in Edinburgh according to principle, and in London according to rule. It is my opinion that the rules of some of us here proceed from the principles we have taken great pains to ascertain and establish.
Besides the safety of chloroform when carefully administered, and its applicability in all cases of operation, whether there is chest disease or not, there is one other point on which I agree entirely with Mr. Syme--viz, that the vapour of chloroform should be largely diluted with air. I am a little particular and precise on this point, and say that there should never be less than ninety five parts of air to five parts of vapour. There are two circumstances which I have ascertained to my perfect satisfaction, by very numerous experiments on animals, and what I have observed and heard of the effects of chloroform on the human subject. The first is, that, if air containing not more than five per cent of vapour of chloroform is breathed till the respiration ceases, the heart continues to beat forcibly for some time afterwards. The second is, that, when air containing eight or ten per cent is breathed, it causes a sudden arrest of the action of the heart, by its direct effect on that organ.*
(*London Journal of Medicine, 1852.)
Now, although death might undoubtedly take place from a person disregarding the symptoms shown by the patient, and continuing the chloroform too long, such an event has not happened, and is not likely to happen, in the hands of medical men. All the accidents have been caused by the direct action on the heart of chloroform not sufficiently diluted with air. The pulse has either ceased before the respiration, or about the same time. If a person who has not experimented carefully with chloroform on animals, nor seen a fatal case of its administration, were to judge entirely by his own observation, he would probably conclude that danger began with the respiration, (because it is in that function that a very slight over-dose manifests its effects when the agent is well diluted with air,) but he would be in error.
The first principle in giving chloroform is to ensure that it shall be very largely diluted with air; but the means recommended by Mr. Syme for this purpose are, in my opinion, insufficient to effect it with certainty. The plan I adopt in practice, is to use an inhaler expressly contrived for insuring a very large admixture of air; but, I have found that many persons allow an apparatus to get out of order, or they are too careless to consider the express purpose for which it was contrived; therefore, if the use of a handkerchief can be rendered safe, it has many advantages. This can be accomplished in midwifery by putting only fifteen minims (equal to sixty-seven drops) on the handkerchief at a time, and waiting till it is used; but, in preparing for a surgical operation, where it is desirable to make the patient quite insensible in about four minutes, it is necessary to use a larger quantity of the agent, and to moisten a greater surface. The proper means to adopt is to dilute the chloroform with spirits of wine. Two parts of spirit and one of chloroform--constituting what Dr. Warren of Boston, United States, calls strong chloric ether--answers very well; but I prefer to use equal parts of chloroform and spirit. The object of the alcohol is not to be inhaled, for it nearly all remains in the handkerchief, but to cause the air to take up less vapour than it otherwise would do. Whilst air is capable of taking up fourteen per cent of vapour from pure chloroform, at 60º Fahr., it can only take up eight per cent from chloroform diluted with an equal measure of spirit; and, in the practice of inhalation, it would rarely take up more than four or five per cent from such a solution, and accidents would be avoided.
It has often been repeated, that chloroform is irritating to the air passages when mixed with spirit; but this is altogether a mistake. When chloroform was first administered in London, in 1847, it was inhaled from its solution, in about seven parts of spirit, under the name of chloric ether. It produced no irritation whatever, and was only left off on account of the uncertainty of its action in such a diluted form, and its expense. Dr. Simpson, as is well known, afterwards introduced its use in the undiluted state; but, except where persons are willing to use a proper apparatus, and take pains with it, it is desirable to return again to a solution of chloroform in spirit, which must be much stronger, however, than that first employed.
I am, Sir, your obedient servant,
John Snow, M.D.
Sackville-street Jan 1855.
Return to John Snow Publications
89.
"Testimony before the Parliamentary Select Committee on the Public Health Bill and Nuisances Removal Amendment Act on 5 March 1855."
Source: Snow, John. Published much later in British Parliamentary Papers 8, Shannon, Ireland: Irish University Press, 1970.
(5 March 1855)
Benjamin Hall, Member of Parliament and (at the time) President of the second General Board of Health, chaired this Select Committee.
Below, I've provided several excerpts in lieu of a complete transcription:
Para. 117. Chairman] [Benjamin Hall, concurrently the President of the General Board of Health] Do you practice as a medical man in the Metropolis?——(Italic - John Snow) Yes, in Sackville-street.
118 You wish to give some evidence upon the Nuisances Removal and Diseases Prevention Act?——I have been requested to give evidence on behalf of the tradespeople in the south districts of London more particularly.
119 Upon what point?——I received a request from Mr. Knight. I was asked if I would give evidence on behalf of the manufacturers whose interests are threatened by the Nuisances Removal Act. I have not seen the parties, nor learnt any particulars. From my printed publications they have learnt that my opinion is, that measures necessary to protect the public health would not interfere with useful trades; and I believe it is on that account that they have asked me to give evidence on their behalf, and I have expressed my willingness to do so.
120 To what points would you desire to draw the attention of the Committee as regards the sanitary question?——I have paid a great deal of attention to epidemic diseases, more particularly to cholera, and in fact to the public health in general; and I have arrived at the conclusion with regard to what are called offensive trades, that many of them really do not assist in the propagation of epidemic diseases, and that in fact they are not injurious to the public health. I consider that if they were injurious to the public health they would be extremely so to the workmen engaged in those trades, and as far as I have been able to learn, that is not the case; and from the law of diffusion of gases, it follows, that if they are not injurious to those actually on the spot, where the trades are carried on, it is impossible they should be so to persons further removed from the spot.
121 Are the Committee to understand, taking the case of bone-boilers, that no matter how offensive to the sense of smell the effluvia that comes from bone-boiling establishments may be, yet you consider that it is not prejudicial in any way to the health of the inhabitants of the district?——That is my opinion.
122 Mr Greene.] Does that extend to all animal substances?——No; I believe that epidemic diseases are propagated by special animal poisons coming from diseased persons, and causing the same diseases to others, and that they are extremely injurious; but that substances belonging to animals, that is to say, ordinary decomposing animal matter, will not produce disease in the human subject.
123 Do you apply that, also, to decaying vegetable matter; do you consider that that will not be productive of disease?——I do not believe that decaying vegetable matter would be productive of disease; at least, it is a matter open for discussion whether certain decomposing vegetable substances, in marshy districts, may not produce ague; but in London, in any trade I am acquainted with, I do not believe that any decomposing vegetable or animal matters produce disease.
124 Chairman.] Take the case of a bone-boiling establishment, or a knacker's yard; assuming that there is a large number of horses in a state of decomposition, from which of course there would be very offensive effluvia, as far as the sense of smell is concerned, do you apprehend that that would not be prejudicial to the health of the inhabitants round?——I believe not.
125 Mr. Adderley.] Have you never known the blood poisoned by inhaling putrid matter?——No; but by dissection wounds the blood may be poisoned.
126 Never by inhaling putrid matter?——No; gases produced by decomposition, when very concentrated, will produce sudden death; but where the person is not killed, if the person recovers, he has no fever or illness.
127 Mr. Egerton.] You mean to say, that the fact of breathing air which is tainted by decomposing matter, either animal or vegetable, will not be highly prejudicial to health?——I am not aware that it is, unless it be in such quantities as to produce actually fatal effects at the moment; but to produce those effects it requires that it should be highly concentrated.
128 Do not you know that the effect of breathing such tainted air often is to produce violent sickness at the time?——Yes, when the gases are in a very large quantity, as in a cesspool.
129 Do you mean to tell the Committee that when the effect is to produce violent sickness there is no injury produced to the constitution or health of the individual?——No fever or special disease.
130 Mr. Greene.] Are you not aware that persons going into vaults where there are a number of dead bodies have suffered very severely, and that sometimes death has been produced by this cause?—— Yes, when those gases are extremely concentrated, they will actually poison a person and cause death, but not cause disease; those poisons do not reproduce themselves in the constitution.
.....
131 Mr. Egerton.] You say that the effluvia arising from living subjects are dangerous?——Or even from certain persons who have died from disease.
132 Mr. Wilkinson.] But not from the mere decay of animal matter?——Not from the mere decay of animal matter.
.....
133 Chairman.] I understand you to say that such effluvia, when highly concentrated, may produce vomiting, but that they are no injurious to health. How do you reconcile those two propositions?—— If the vomiting were repeatedly produced, it would certainly be injurious to health. If a person was constantly exposed to decomposing matter, so concentrated as to disturb the digestive organs, it must be admitted that that would be injurious to health; but I am not aware that, in following any useful trade or manufacture, the effect is ever experienced.
.....
134 [Mr. Wilkinson questioning] Have you turned your attention to the effects of the late outbreak of cholera in London?—— Yes, I have made special inquiries throughout Lambeth and Southwark and Newington.
135 Have you satisfied yourself by those inquiries of any particular results of that outbreak of cholera, so as to state your opinion if what has been the mode of propagation of the disease?——
Return to John Snow Publications
90.
"On the chief cause of the recent sickness and mortality in the Crimea"
Source: Snow, John. Medical Times and Gazette 10, 12 May 1855, pp. 457-58.
By John Snow, M.D.
The diseases which have been most prevalent and fatal in the Crimea have been Cholera, Dysentery, Diarrhœa, and Fever. The fever, according to what I can learn respecting it, has been typhoid, accompanied with ulceration of the small intestines, and consequently the whole of the diseases prevalent in the Crimea have consisted mainly of affections of the alimentary canal.
The communications which I made to the Medical Times and Gazette in September and October last, respecting the influence of the water-supply on the prevalence of cholera in the south districts of London, showed very clearly that this disease may be propagated by water containing the evacuations of cholera patients. The conditions were remarkably favourable for the inquiry I undertook; the circumstances and situation of a very large population were exactly the same in every particular, except that a part received a water supply containing the sewage of London, and another part, intimately mixed with it, had a water-supply quite free from such contamination. Whilst the former part of the population suffered excessively from cholera, the latter suffered no more than the population of London on the north of the Thames. The inquiries of the Registrar-General, taken up at the point at which I left off, and continued to the end of the epidemic, entirely confirmed these results.
That the water produces its effects by conveying the cholera poison, and not by its general impurity acting as an accessory or a predisposing cause, can be proved by a number of facts. In the first place the water may be very impure in time of cholera without influencing the disease, if it does not contain what comes from cholera patients. The impure water of many pump-wells and of neglected cisterns affords numerous proofs of this, and I may also mention that Dr. Glover states, as quoted by Dr. Sutherland,* that the water from the Kent Waterworks was very similar in its chemical characters to that supplied by the Southwark and Vauxhall Company, yet my inquiries and the reports of the Registrar-General show that whilst the population supplied with the latter water suffered excessively from cholera, that supplied from the Kent Waterworks suffered but very little, except in two streets at Deptford, where the water received a local contamination, which I described in the Medical Times and Gazette in September last. Now there is this great difference between the Southwark and Vauxhall water and that of the Kent Water Company–-the former is taken from the Thames, which receives the sewage of all London and the refuse of the shipping, while the latter is taken from the river Ravensbourne, which is contaminated only by the drainage of some parts of Lewisham, Eltham and Lea, where hardly any cholera existed.
(*Report on Cholera in 1854, p. 47.)
Another circumstance, which shows that impure water cannot be a mere predisposing cause of cholera is, that I met with several instances in the South Districts of London, in which persons were attacked by this disease within eight and forty hours after arriving from parts of the country not affected with cholera; these persons drank the water of the Southwark and Vauxhall Company after their arrival. Lastly, the fact of a number of persons being attacked at one time, after one or two cases of cholera have occurred amongst those whose evacuations habitually contaminate the ditch or pump-well from which they drink, shows that the water contains the real and efficient cause of the malady; for if the excess of cases was merely occasioned by the ordinary impurity of the water always present, it would be distributed over the whole time of the epidemic, instead of occurring in one sudden and intense outbreak.
The proof of the communication of cholera through the medium of water, of course completely confirms the fact of its propagation in a more direct way, by swallowing the morbid poison without the water, in the crowded dwellings of the poor, in coal pits, and other situations.
The proof of the manner of communication of the other diseases which have been prevalent in the Crimea is not so conclusive as that which regards cholera, but the evidence which can be collected on the subject tends to show that they are propagated in the same way as cholera. Dysentery has often been noticed to be occasioned, or kept up, by the use of water containing human excrement. This was observed by Mr. Bell, of Cork, in the old barracks at that town.*
(*Dr. Cheyne on Dysentery, Dublin Hospital Reports. Vol III.)
The prevalence of dysentery among the crews of ships stationed in the great rivers of India and China has been noticed by nearly all writers on the diseases which prevail in tropical climates, and Dr. Bryson has related a number of instances in which both dysentery and fever seemed to be occasioned by drinking the water of the Yang-tse-Kiang, the Canton river, and other rivers of China.†
(†Statistical Reports on the Health of the Navy. Part II. 1853.)
Along with other impurities the great rivers of India and China contain the fæces of a large population, amongst whom dysentery always prevails more or less. One circumstance worthy of remark is, that Dr. Bryson and several other writers have alluded to the great frequency of intestinal worms, chiefly lumbrici, in the cases of dysentery and fever in the above situations. I do not, of course, consider there is any connexion between the other diseases and the worms, but the existence of these creatures proves that the patients have been exposed to swallow matters which have come from the bowels of other persons; as the worms can only arise from the ova of their own species, produced by the animal in its proper habitat. In the Medical Times of March 31, p. 318, Mr. Prentice relates how he contracted dysentery by drinking the water of a pool in the half-formed course of a stream in Australia. That colony was once, like California and many new countries, famous for the healthiness of the new settlers, which was erroneously attributed to the climate. Its reputation for health has been gradually dispelled as one fresh disease after another has been imported, and the diggings are infested with some of the bowel complaints which infest camps and other places where persons reside together in great numbers, without the appliances for drainage and water-supply which usually exist in a town.
The production of diarrhœa by water containing sewage matters is well known. I have been informed by many persons that they were attacked with diarrhœa on first going to live in some of the southern suburbs of London, and drinking the impure water of the Thames, supplied to them by the Southwark and Vauxhall Company. Sailors often suffer in the same way, from drinking the Thames water before it has spontaneously purified itself; and I was lately informed by a Medical man, who has lived in St. Petersburg, that strangers are nearly always attacked with diarrhœa and colic on first drinking the water of the Neva, which receives the sewage of the town. In the autumn of 1853 diarrhœa was very prevalent in Croydon, and Mr. Carpenter, Surgeon, of that town, found that it was caused by the impure water of the pump-wells. Nine-tenths of the people of Croydon were drinking the new water supplied by the Board of Health; but, out of thirty-two patients with diarrhœa who came under the care of Mr. Carpenter, twenty-five were drinking well-water entirely; five drank water from both sources, and the other two could not say decidedly that they had not drunk well-water.‡
(‡Association Journal, Oct 6, 1854.)
Mr. Carpenter has also traced the great epidemic of typhoid fever which prevailed in Croydon in the previous year, to contamination of the water of the pump wells, occasioned by the disturbance of the ground and of many old cesspools in the new drainage operations which preceded that outbreak.*
(*Loc, cit.)
The stoppage of many of the porcelain pipes, and the consequent leakage from them into the ground soon after they were laid down, must have greatly assisted in the propagation of the disease through the pump water. Dr. Flint of America relates an instance occurring at North Boston, Erie County, New York, in which typhoid fever was apparently communicated to a number of families by the contamination of the water of a pump-well which they were using,† and Ihave been informed of some other instances of the same kind.
(†Clinical Reports of Continued Fevers. Buffalo. 1852.)
The diseases which have prevailed among the troops in the Crimea were all present, with the exception of scurvy, before they left Varna, as soldiers ill of cholera, dysentery, and diarrhœa were sent from the latter place to the Bosphorus at the time the expedition sailed to the Crimea. The French when at Varna suffered from cholera much more then the English, but after the allied armies removed to the Crimea the sickness and mortality from cholera and other diseases was much greater amongst the British troops than the French. The chief cause of this circumstance probably is that the French, soon after sitting down before Sebastopol, laid down iron pipes to convey water to the army from the hills above the camp, whilst the English adopted no such measure.
I find from a leading article in the Medical Times and Gazette of March 10, that "the water which many of them (the soldiers) drank was impregnated with the most disgusting filth, for it seems that almost the only water used for drinking in the vicinity of Balaklava is that of a small stream which flows from the adjacent mountains, and in its whole course receives the remains of dead horses, the offal of the slaughtered oxen, and even sometimes bodies of dead men." This stream must also have received the excrement of the troops, for any measures which would have defended it from this latter kind of pollution would also have saved it from those which are mentioned above.
There are some springs which supply water to part of the British army before Sebastopol. The ground, however, consists of limestone and clay, neither of which has the property which is possessed by sandstone and gravel of oxidizing and destroying organic matter. It is extremely probable, therefore, that the springs are also contaminated with the excreta of the troops. A proper examination of the situation of the springs and of the nature of the water might help to decide this, for though neither chemistry nor the microscope can do anything towards detecting morbid poisons, they may be used to determine whether or not the animal matters which percolate the soil are entirely changed into nitrates and other mineral substances before they reach the water.
The distribution of rum to the army has probably been a great cause of the propagation of disease through the medium of polluted water. Malt liquors do not require to be diluted, and tea, coffee, and cocoa are always prepared with boiled water; whilst on the other hand distilled spirits require to be diluted with water, which generally is not boiled.
It is quite obvious that every disease which can be communicated through the medium of water may also be communicated by swallowing the morbid matter without the water. It is, therefore, probable that the want of water for washing the hands must have assisted in the propagation of the various maladies amongst the soldiers, several of whom live together in a small tent. This is most likely one of the reasons why the common soldiers have suffered a greater mortality from disease than the officers; another reason probably is that the officers would be more particular about the water they drank; I have been informed of some who sent their servants a great distance for it, as early as four o’clock in the morning, before the horses should come to drink and render the stream muddy. As the officers suffered less from fatigue and exposure to the weather than the soldiers, they would also be in a better condition to recover from any disease with which they might be attacked.
Since all the chief diseases which have been so fatal in the Crimea were present in the army before it left Varna, we do not require to look for their causes in the former place, but only for the means of their propagation, which appear to have been abundant enough, as I have endeavoured to show above. The overwork, the exposure to cold, and the occasional privation which the men have suffered would lessen chances of recovery from the diseases with which they were attacked. These circumstances could not produce a case of specific disease, like cholera or fever; it is very doubtful whether they could produce dysentery, and the only one out of the four chief diseases which have prevailed in the Crimea that might be caused by any of the above circumstances is diarrhœa. The indigestible food sometimes served out, and the extreme exposure to the weather might cause this latter complaint, but that extreme labour, cold, and privation do not of themselves occasion epidemic diseases is shown in the history of the expeditions to the Arctic regions, where the adventurers die only from accident or absolute starvation.
At a time when the chemistry of gaseous substances did not exist, and when certain fevers, dysentery, and some other diseases were attributed to a putrefaction of the fluids of the living body, these diseases were supposed to be occasioned by the effluvia given off during ordinary putrefaction. These opinions have still a certain number of adherents, even in official quarters, and it is worthy of the attention of those individuals that the greatest mortality in the Crimea took place at a time when the temperature was too low for putrefaction to go on, and when it was especially noticed that though many dead horses were lying about they emitted no smell.
The chief means of preserving the health of troops in a camp is to have water conveyed in pipes or otherwise from some place where it is out of the reach of contamination, and until such a measure can be taken no water should be drunk that has not first been boiled. As regards the drainage at a camp, it should be borne in mind that it is chiefly useful in preventing the pollution of the water. When this rule is not considered, drainage may become a source of the propagation of disease, as recently at Croydon, Sandgate, and other places, instead of being its prevention. The advice of Sir John Pringle that the men should be compelled to make use of the camp privies on all occasions ought to be attended to, and the privies should be so constructed and kept that the hands would not be liable to get soiled by them.
Sir John Pringle insisted more than a hundred years ago on the advantage of having a number of small hospitals instead of one of greater extent, in order to check as much as possible the spread of disease by contagion. Our Allies have acted on this advice in preparing a number of small hospitals along the shores of the Bosphorus; but the authorities of Sir John Pringle’s own country have totally disregarded it in forming an hospital of gigantic dimensions at Scutari, with a result that is too well known to require comment. Official persons in this country have generally acted of late years as if there were no such thing as the communication of disease; but the great mortality amongst Medical men and nurses at Scutari ought to convince them of their error.
18, Sackville-street, April, 1855.
Return to John Snow Publications
91.
" 'Dr. Snow's Report,' in the Report on the Cholera Outbreak in the Parish of St. James, Westminster, during the Autumn of 1854"
Source: Snow, John. London: Churchill, July 1855, pp. 97-120.
Snow dated his report, 12 December 1854, the day he submitted it to the Cholera Inquiry Committee (at their request) recently established by the Vestry of St. James, Westminster parish. This report contained the most expansive discussion of his findings whilst investigating the Golden Square outbreak, including the addition of a new feature to the map already published in On the mode of communication of cholera." 2nd edition, much enlarged, 1855.
Dr. Snow's Report.
[Constituting part 3 of the Cholera Inquiry Committee's Report to the Vestry of St. James, Westminster parish]
Having been requested by this Committee to draw up a Report on the water used in the locality so severely visited by Cholera, I beg to lay the following statement before you:--
The water supply of the district consists of that of the water companies and that of the street-pumps. The sub-district of Golden Square is supplied by the Grand Junction Company, with water from the Thames, facing Brentford, at Kew, which is almost entirely freed from animal and vegetable impurities before it is distributed. The sub-district of Berwick Street is supplied by the New River Company; the division between the companies being exactly that between the two sub-districts of the parish just named. The remaining districts supplied by the Grand Junction Company have been remarkably free from Cholera, both during the present year and in 1849; and most of the districts supplied by the New River Company have also been lightly visited by the malady on both occasions; there is, therefore, in my opinion, no reason to suppose that the water of either of these companies contributed to the late outbreak of Cholera. One circumstance which remarkably confirms this view is, that the outbreak commenced on the same day, and almost at the same hour, in both sub-districts; and if it were possible that any pollution of the water supply of the two companies could have taken place, we cannot suppose that it would have occurred at the same time, and at two adjoining spots, in two systems of pipes in which the supply is derived from such very different sources.
With respect to the pump wells, I found some impurities in the water of each of those which I examined in the first week of September, in the Golden Square district, except the one in Vigo Street. The water of the pumps in Broad Street, Warwick Street, and Bridle Lane, all contained impurities visible to the naked eye on close inspection, in the form of minute, whitish, flocculent particles. The water of the pump in Marlborough Street contained a still larger quantity of organic impurities than the others, and most of the people in its neighbourhood avoided using the water, and sent to Broad Street. In my opinion, mere impurity in the water would not cause Cholera, unless it were of a special kind--unless, in fact, the impurity had proceeded from a Cholera patient. Dr. Lankester has, I believe, particularly examined [98/99] the water of the pump in Broad Street, which is situated in the centre of the area in which the mortality from Cholera occurred; and he will, no doubt, inform the Committee of the result of his researches. Dr. Hassall was good enough to examine some of this water, at my request, with the microscope, and he informed me that the particles I have mentioned above had no organized structure, and that he thought they probably resulted from the decomposition of other matter. He found a great number of very minute, oval animalculæ in the water, which are of no importance, except as an additional proof that the water contained organic matter on which they lived. I found that the water also contained a large quantity of chlorides--indicating, no doubt, the impure sources from which the spring is supplied. Mr. Eley of 38, Broad Street, informed me that he had long noticed that the water became offensive, both to the smell and taste, after it had been kept about two days. A person, at 6, Poland Street, also informed that he had noticed, for months, that a film formed on the surface of the water after it had been kept a few hours. These are characters of water which is contaminated with sewage.
I inquired of many persons whether they had observed any change in the character of the water about the time of the outbreak of Cholera, and was answered in the negative. I afterwards, however, met with the following important information on this point:--Mr. Gould, the eminent ornithologist, lives near the pump in Broad Street, and was in the habit of drinking the water. He was out of town at the commencement of the outbreak of Cholera, but came home on Saturday morning, the 2nd of September, and sent for some of the water almost immediately, when he was much surprised to find that it had an offensive smell, although perfectly transparent, and fresh from the pump. He drank scarcely any of it. Mr. Gould's assistant, Mr. Prince, had his attention directed to the water, and perceived its offensive smell.
Whether the impurities of the water were derived from the sewers, the drains, or the cesspools, of which latter there are, I believe, a number in the neighbourhood, I cannot tell. I have been informed, by an eminent engineer, that whilst a cesspool in a clay soil requires to be emptied every six or eight months, one sunk in the gravel will often go for twenty years without being emptied, owing to the soluble matters passing away into the land-springs by percolation.
I requested permission, on the 5th of September, to take a list, at the General Register Office, of the deaths from Cholera registered during the week ending the 2nd of September, in the sub-districts of Golden Square and Berwick Street, St. James's, and St. Anne's Soho, which was kindly granted. Eighty-nine deaths from Cholera were registered during the week, in the three sub-districts. Of [100/101] these only six occurred on the first four days of the week; four occurred on Thursday the 31st of August; and the remaining 79 on Friday and Saturday. I considered, therefore, that the outbreak commenced on the Thursday; and I made inquiry in detail respecting the 83 deaths registered as having taken place during the last three days of the week.
On proceeding to the spot, I found that nearly all the deaths had taken place within a short distance of the pump in Broad Street. There were only ten deaths in houses situated decidedly nearer to another street-pump. In five of these cases, the families of the deceased persons told me that they always sent to the pump in Broad Street, as they preferred the water to that of the pump which was nearer. In three other cases, the deceased were children who went to school near the pump in Broad Street. Two of them were known to have drunk the water, and the parents of the third think it probable that it did so. The other two deaths, beyond the district which this pump supplies, represent only the amount of mortality from Cholera that was occurring before the eruption took place.
With regard to the 73 deaths occurring in the locality belonging as it were to the pump, there were 61 instances in which I was informed that the deceased persons used to drink the water from the pump in Broad Street, either constantly or occasionally. In six instances I could get no information, owing to the death or departure of every one connected with the deceased individuals; and in six cases I was informed that the deceased persons did not drink the pump water before their illness.
The result of the inquiry consequently was, that there had been no particular outbreak or increase of Cholera, in this part of London, except among the persons who were in the habit of drinking the water of the above-mentioned pump well.
I had an interview with the Board of Guardians of St. James's parish on the evening of Thursday, 7th September, and represented the above circumstances to them. In consequence of what I said, the handle of the pump was removed on the following day.
Besides the 83 deaths mentioned above, as occurring on the three last days of the week ending September 2nd, and being registered during that week in the sub-districts in which the attacks occurred, there was a number of persons who died in the Middlesex and other hospitals, and a great number of deaths which took place in the locality during the two last days of the week, were not registered till the week following. The deaths altogether on the 1st and 2nd of September, which have been ascertained to belong to this outbreak of Cholera, were 197, and many persons who were attacked about the same time as these, died afterwards. I should have been glad to inquire respecting the use of the water from Broad Street pump in all these instances; but I was engaged at the time in an inquiry in the south districts of London; and when I began to make fresh inquiries in the neighbourhood of Golden Square, after two or three weeks had elapsed, I found that there had been such a distribution of the remaining population, that it would be impossible to arrive at a complete account of the circumstances. There is no reason to suppose, however, that a more extended inquiry would have yielded a different result from that which was obtained respecting the 83 deaths which happened to be registered within the district of the outbreak, before the end of the week in which it commenced.
The additional facts that I have been able to ascertain, are in accordance with those above related; and as regards the small number of those attacked, who were believed not to have drunk the water from Broad Street pump, it must be obvious that there are various ways in which the deceased persons may have taken it without the knowledge of their friends. The water was used for mixing with spirits in some of the public houses around. It was used, likewise, at dining rooms and coffee shops. The keeper of a coffee shop which was frequented by mechanics, and where the pump water was supplied at dinner time, informed me on the 6th of September, that she was already aware of nine of her customers who were dead! The water of this pump was also sold in various little shops with a tea-spoonful of effervescing powder in it, under the name of sherbet, and it may have been distributed in various other ways with which I am unacquainted. The pump was frequented much more than is usual, even for a London pump in a populous neighbourhood.
There are certain circumstances bearing on the question which deserve to be mentioned. The workhouse in Poland Street is more than three-fourths surrounded by houses in which deaths from Cholera occurred; yet, out of 535 inmates, only five died of Cholera - the other deaths which took place being those of persons admitted after they were attacked. The workhouse has a pump on the premises in addition to the supply from the Grand Junction Water Works, and the inmates never sent to Broad Street for water. If the mortality in the workhouse had been equal to that in the streets immediately surrounding it on three sides, upwards of 50 inmates would have died. There is a brewery in Broad Street near to the pump, and on perceiving that no brewer's men were registered as being dead of Cholera, I called on Mr. Huggins the proprietor. He informed me that there were above 70 workmen employed in the brewery, and that none of them had suffered from Cholera, at least in a severe form, only two having been indisposed, and that not seriously, at the time the disease prevailed. The men are allowed a certain quantity of malt liquor, and Mr. Huggins believes they do not drink water at all, and he is quite certain that they never obtained water from the pump in the street. There is a deep well in the brewery in addition to the New River water.
At the wire cartridge and percussion cap manufactory, 38, Broad Street, where I understand about 200 work people were employed, two tubs were kept on the premises always supplied with water from the pump in the street for those to drink who wished, and 18 of those work people died of Cholera at their own houses - sixteen women and two men. Mr. Peter Marshall, surgeon, No. 53, Greek Street, was kind enough to inquire respecting seven workmen, who had been employed in the manufacture of dentists' materials at Nos. 8 and 9, Broad Street, and who died at their own homes. He learned that they were all in the habit of drinking water from the pump, generally drinking about half a pint once or twice a day, while two persons who reside constantly on the premises, but do not drink the pump water, had only diarrhea. Mr. P. Marshall also informed me of the case of an officer in the army who lived at St. John's Wood but came to dine in Wardour Street, where he drank the water from Broad Street pump at dinner. He was attacked with Cholera and died in a few hours.
Dr. Fraser of Oakley Square, St. Pancras, kindly informed me of the following circumstance: - A gentleman in delicate health was sent for from Brighton to see his brother at No. 6, Poland Street, who was attacked with Cholera and died in twelve hours on the 1st of September. The gentleman arrived after his brother's death and did not see the body. He only staid about twenty minutes in the house, where he took a hasty and scanty luncheon of rump steak, taking with it a small tumbler of cold brandy and water, the water being from Broad Street pump. He went to Pentonville, and was attacked with Cholera on the evening of the following day, September the 2nd, and died the next evening.
The deaths of Mrs. E--- and her niece, who drank the water from Broad Street at West End, Hampstead, deserve especially to be noticed. I was informed by Mrs. E---'s son that his mother had not been in the neighbourhood of Broad Street for many months. A cart went from Broad Street to West End every day, and it was the custom to take out a large bottle of the water from the pump in Broad Street as she preferred it. The water was taken out on Thursday the 31st of August, and she drank of it in the evening, and also on Friday. She was seized with Cholera on the evening of the latter day, and died on Saturday. A niece who was on a visit to this lady also drank of the water; she returned to her residence, a high and healthy part of Islington, was attacked with Cholera and died also. There was not Cholera at the time, either at West End or in the neighbourhood where the niece died. Besides these two persons only one servant partook of the water at West End, Hampstead, and she did not suffer, or, at least, not severely. She had diarrhea.
[Detail of the map enclosed with the original report. The Broad Street pump is indicated by a smudged area, center-left. The stippled line is "the inner dotted line" mentioned below that demarcates equal walking distances between the pump in Broad Street and the nearest rival pump at every point.]
There were some persons who drank the water from Broad Street pump about the time of the outbreak without being attacked with Cholera, but this does not diminish the evidence respecting the influence of the water, for various reasons.
The deaths which occurred during the fatal outbreak of Cholera are indicated in the accompanying map, as far as I could ascertain them. There are necessarily some deficiencies, for in a few of the instances of persons who died in the hospitals after their removal from the neighbourhood of Broad Street, the numbers of the houses from which they had been removed were not registered. The address of those who died after their removal to St. James's Workhouse was not registered, and I was only able to obtain it in a part of the cases, on application at the Master's office, for many of the persons were too ill when admitted to give any account of themselves. In the case also of some of the work people and others who contracted the cholera in this neighbourhood, and died in different parts of London, the precise house from which they removed is not stated in the return of deaths. I have heard of some persons who died in the country shortly after removing from the neighbourhood of Broad Street, and there must no doubt be several cases of this kind that I have not heard of. The deficiencies I have mentioned, however, do not detract from the correctness of the map, as a diagram of the topography of the outbreak; for, if the locality of the additional cases could be ascertained, they would probably be distributed over the district of the outbreak in the same proportion as the large number which are known.
The outerdotted line on the map surrounds the sub-districts of Golden Square and Berwick Street, St. James's together with the adjoining portion of the sub-district of St. Anne's, Soho, extending from Wardour Street to Dean Street, and a small part of the sub-district of St. James's Square, enclosed by Marylebone Street, Tichborne Street, Great Windmill Street, and Brewer Street. All the deaths from Cholera which were registered in the six weeks from August the 19th to September the 30th within this locality, as well as those of persons removed into Middlesex Hospital, are shewn by black lines in the situation of the houses in which they occurred, or in which the fatal attacks were contracted. In addition to these the deaths of persons removed to University College, St. George's, Charring Cross, and other hospitals, and to various parts of London, are indicated in the map where the exact address was given in the Weekly Return of Deaths, or when I could learn it by private inquiry.
The pump in Broad Street is indicated on the map, as well as all the surrounding pumps to which the public had access at the time of the outbreak of Cholera. It requires to be stated that the water of the pump in Marlborough Street, at the end of Carnaby Street, was so impure that many persons avoided using it; and I found that the persons who died near this pump, in the beginning of September, had water from the Broad Street pump. The inner dotted line on the map shews the various points which have been found by careful measurement to be at an equal distance by the nearest road from the pump in Broad Street and the surrounding pumps; and, if allowance be made for the circumstance just mentioned respecting the pump in Marlborough Street, it will be observed that the deaths either very much diminish, or cease altogether, at every point where it becomes decidedly nearer to send to another pump than to the one in Broad Street. At these points I ascertained that the people did generally send to the pump which was nearer. It may be noticed the deaths are most numerous near to the pump in Broad Street, where the water could be more readily obtained. The wide open street in which the pump is situated suffered most, and next the streets branching from it, especially those parts of them which are nearest to Broad Street. If there have been fewer deaths in the south half of Poland Street than in some other streets leading from Broad Street, it is no doubt because this street is less densely inhabited.
I have made a distinct inquiry respecting the greater number of fatal cases of Cholera that occurred, at the time of the outbreak, within the outer boundary marked on the map, but in a situation very decidedly nearer to another public pump than to that in Broad Street, and the following are the results:--
On the 4th of September, a female, aged 42, died at 32, Great Marlborough Street. I learned from the persons with whom she lived that she habitually drank pump water, but did not get it from the pump opposite. She had it principally from Broad Street, but occasionally from Vigo Street. There were three deaths at 7, Great Marlborough Street, on the 2nd, 3rd, and 5th of September. This house is rather nearer to two other pumps than to the one in Broad Street, but water had been fetched from the latter pump, and had been drank at dinner for a fortnight previous to the attacks of Cholera.
On the 1st of September, a girl aged 8 years, died at 29, Carnaby Street. On calling a few days afterwards I was informed by other members of the family that they were in the habit of having water from Broad Street, and that deceased drank of it on the days preceding her illness. On the same day, a female, aged 34, died at 31, Carnaby Street. I was informed, on making inquiry, that she used to send to Broad Street two or three times a-day for water to drink. On the 1st also, a female, aged 35, died at 40, Carnaby Street. I was informed that she sent nearly always to Broad Street for drinking water.
The houses in which the above three cases occurred are in that part of Carnaby Street which is near to the pump in Marlborough Street; and Tyler Street, in which the following cases occurred is also very near to the same pump.
Two widows who lived in the kitchen at No. 9, Tyler Street, were attacked with Cholera on the 2nd of September, and were taken to Middlesex Hospital, where they both died. The daughter of one of the deceased women, a girl aged 15, told me that she used to fetch water from Broad Street pump, as her mother did not like the water in Marlborough Street. Both the deceased persons used to drink the water up to the time of their illness. My informant also drank of it; she had a Diarrhea, but was not seriously ill. On the 2nd of September, a man and his wife died of Cholera at 8, Tyler Street. The landlord of the house made an inquiry of the grown-up children of the deceased persons for me, and I learned that they used to have water from the pump in Broad Street, as they considered the water in Marlborough Street not fit to drink.
On the 1st of September, a tailor, aged 50, and his son, aged 12, died of Cholera, at 10, Cross Street, and within three days afterwards four more of his children died, two of them being grown up. This family were great drinkers of pump water, and used to send for it every day, but more especially to drink during the night, as they were thirsty in the warm weather, owing to the great number sleeping in one room. The children fetched the water from various pumps, but frequently from Broad Street. On the 2nd of September, a boy, aged 7 years, died at 4, Cross Street. This family sent frequently for pump water, both to Broad Street and Warwick Street.
On the 2nd of September, a carpenter, aged 30, died at 7, Upper John Street, Golden Square. He was a foreigner, and used to drink wine and water to his dinner. The water was procured by the people who kept the house, and they got it from Broad Street pump, as they thought the water better than that in Warwick Street, which is much nearer. Two other persons, who also drank the water, were taken ill at the same time as deceased, but recovered. One was the servant of the house, and the other was a young man in the family. My informants were the widow of the deceased man and the sister of the young man who recovered. It is worthy of notice, that the servant had an attack of Cholera a fortnight previous to the last one.)
A girl, aged 5 years, died at 42, Ham Yard, on the 8th of September, having been attacked with Cholera on September the 2nd. Deceased went to school in Dufour's Place, and a brother, a little older than herself, told me in the presence of his mother that he had seen his sister drink the water from the ladle at the pump in Broad Street. A girl, aged 7 years, at 3, Angel Court, Great Windmill Street, was attacked with Cholera on the 1st of September, and died on the 8th. She also went to school in Dufour's Place, and her parents think it probable that she drank the water of Broad Street pump. A boy, aged 9 years, died on the 2nd of September, at 9, Great Crown Court. He went to school near the pump in Broad Street, and was in the habit of drinking a good deal of the water.)
At 13, Wardour Street, near to Oxford Street, the wife of a tradesman died on the 2nd of September. Her husband informed me that they used to have pump water which deceased used to drink. The boy was always directed to fetch it from Broad Street. The son of a chemist at 115, Wardour Street, which is about a dozen doors from Oxford Street, was attacked with Cholera, and went to Willesden, where he died on the 2nd or 3rd of September. He dined on the days preceding his attack at some dining-rooms in Wardour Street, where the water from Broad Street pump always stood on the table. He drank malt liquor with his dinner, but frequently took some water with the pastry or sweet pudding with which he concluded it. His father was my informant.)
The wife of a tailor at 2, Great Chapel Street, Soho, was attacked with Cholera on the 4th, and died on the 8th of September. I was informed by the person with whom she lodged, that she was a great drinker of pump water, and that she used to drink a good deal of cold water at the Baths and Wash-houses in Dufour's Place, where she had been at work on the days preceding her illness. On going to the Wash-houses I learned that some persons drank the water of the cistern there, and others that of the Broad Street Pump. The child of this woman was attacked on the 7th and died on the 11th of September.)
There were three deaths at 14, Noel Street; two on the 1st of September, after a few hours' illness, and one on the 6th, after an illness of four days. Pump water was constantly drunk in this house. I saw the boy who fetched it in the presence of the family. He generally got it from Berner's Street, or Newman Street, but had occasionally obtained it from Broad Street, and had done so about two months before my inquiry, which was made at the end of October, but he could not remember the day or week when he last obtained it from Broad Street.)
A young woman died at 39, Rupert Street, on the 5th of September, but she was taken ill in St. Anne's Court, where three other members of her family died. She was about to call in Rupert Street, but dropped down at the door; she was carried into the house, where she expired. )
On the 10th of September, a girl, aged eight years, died of Cholera after an illness of three days, at 7, Naylor's Yard, Silver Street; she went to the National School facing the end of Broad Street, and used to drink the water.)
There were four fatal attacks of Cholera at No. 1, Brewer Street, in the beginning of September. One of the deceased persons was the master of the house, who used to send constantly to Broad Street for drinking water, and the others who were attacked were also in the habit of drinking it.)
A cabinet-maker, who was removed from Philips' Court, Noel Street, to Middlesex Hospital, worked in Broad Street. A boy also who died in Noel Street went to the National School at the end of Broad Street, and having to pass the pump probably drank of the water.)
A tailor who died at 6, Heddon Court, Regent Street, spent most of his time in Broad Street. A woman removed to the hospital from 10, Heddon Court, had been nursing a person who died of Cholera in Marshall Street.)
There were eight fatal attacks at a considerable distance from the pump in Broad Street, but within the external boundary marked on the map, respecting which, I did not, on inquiry, trace any connection with the water of that pump.)
Of the above 48 persons, it will be observed that 28 were ascertained to have drunk the water of Broad Street pump shortly before they were attacked, whilst there is a greater or less probability that 10 of the others also drank it, and 2 more had been exposed to the malady, by residing in the same room with a patient who died of it. As regards the 8 cases in which I could trace no connection with the water of the pump in Broad Street, it may be observed that they form but a slight mortality for the large area in which they happened; a mortality not greater than was occurring in surrounding parishes, and probably not greater than would have taken place in this district if the great outbreak had not occurred.)
I ought to mention, that in all the cases I have alluded to throughout the Report, the water from Broad Street was drunk cold, without having been boiled. It is the custom in this district, as elsewhere, always to use the cistern water for making tea, and other purposes where heat is employed, and to send for pump water only for the purpose of drinking it cold.*
(* I should like to mention here, a fact that I met with in making a part of the house-to-house inquiry, which the Committee undertook in the winter. Out of the 14 houses in Cambridge Street, there were four in which I was distinctly told that none of the inmates ever sent to Broad Street for water, and that they did not do so in August last. There was no case of Cholera in any of these houses. In the other 10 houses, the water from the pump in Broad Street was more or less used by the inmates last August, and there was Cholera in all of them but one, and in that house there was Diarrhea--J. S., June 14, 1855.)
The following Table exhibits the chronological features of this terrible outbreak of Cholera:-- )
The deaths in the above Table are compiled from the sources mentioned in describing the map; but some deaths which were omitted from the map, on account of the numbers of the houses not being known, are included in the Table. As regards the date of attack, I was able to obtain it with great precision, through the kindness of Mr. Sibley, in upwards of 80 deaths which occurred in Middlesex Hospital; for the hour of admission was entered in the hospital books, as well as the previous duration of the illness. In a few other cases also I had exact information of the hour of attack; and in the remainder I have calculated the date of attack by subtracting the duration of the illness from the date of death. There are 45 cases in which the duration of the illness was not certified to the registrars, and where I had no means of ascertaining it. The time of the attack in these cases is consequently unknown. These persons nearly all died on the first days of September, in the height of the calamity; and it is almost certain that they were cut off very quickly, like the others who died at this time.
It will be observed that the daily number of fatal attacks was already much diminished by September the 8th, the day when the handle of the pump in Broad Street was removed; and it is not improbable that the water had, from some cause or other, ceased to contain the cholera poison. At all events, the few attacks which took place after September the 10th or 12th must have been occasioned in the usual manner, and not through the medium of the water.
I wish it to be understood that I do not attribute every case of Cholera to the use of polluted water. It is my opinion that every case is caused by swallowing the peculiar poison or morbid matter of Cholera, which has proceeded from a previous patient sick of the same malady; but this morbid matter need not be in water, and there are facilities for its being accidentally swallowed, and propagating the disease, without the aid of water. This is more especially the case in the crowded dwellings of the poor, where a number of persons live, sleep, cook, and eat in one room. I do not, therefore, attribute every case of Cholera in the parish to the water of the pump well in Broad Street, but certainly those which constitute the great outbreak which took place at the end of August, and which suddenly raised the mortality of this disease from about five in a week to nearly 500.
The reason why the water of this pump produced the great outbreak is, I feel confident, that the evacuations of one or more Cholera patients found their way, by some means, into the well. There were fatal cases of Cholera, a few days before the great outbreak, not far from the well, and there may have been other cases, not fatal, which are not recorded.
I published several instances, in 1849, of sudden and severe outbreaks of Cholera arising from the pollution of tanks, wells, and other local supplies of water, by the contents of cesspools and house-drains. In the outbreak at Albion Terrace, Wandsworth Road, in that year, the night soil was from six to nine inches deep at the bottom of the tanks that were examined. In some instances, in Horsleydown and Rotherhithe, the contamination of the water was equally well proved. In these instances, the dejections of a patient ill of Cholera entered the water before the great outbreak.
I have been making inquiries during the autumn just passed, in the South districts of London, which shew that the dejections of Cholera can reproduce the disease after passing down the sewers into the Thames, and being afterwards distributed through some miles of the pipes of a water company. Under these circumstances, the cases of Cholera are scattered over the whole of the districts supplied by the company; and become gradually more numerous, as each set of cases, the dejections of which pass into the river, produces new ones. In the instances, on the other hand, in which a pump well, or some other local supply of water is thus contaminated, the outbreak is always sudden and violent.
John Snow, M.D.
12th December 1854.
Return to John Snow Publications
92."The case of fissure of the sternum"
Source: Snow, John. Lancet 2, 7 July 1855, p.17 [Letter to Ed.].
To the Editor of the Lancet.
Sir,--I shall be obliged if you will allow me to make a few remarks on the case of fissure of the sternum, to which you have called the attention of the profession in the last two numbers of the Lancet. This case has been under the notice of several medical men of eminence in Paris and Strasbourg, who have expressed their opinions in the medical journals of those towns. These opinions, however, differ widely from each other; for whilst M. Forget and M. Jules Béclard consider that the phenomena connected with the heart in this case support the ancient and usual doctrine of the action of that organ, Dr. F. A. Aran believes that they confirm the extra-ordinary doctrine that the impulse of the heart against the walls of the chest is caused by the penetration of the blood from the auricles into the ventricles, and that, in fact, what is considered to be the systole of the ventricles is the diastole. All the observers agree, however, in believing that the pulsation which is seen through the integuments, in the centre of the fissure, is caused by the alternate dilation and contraction of the right auricle--that is to say, by its being alternately filled with blood from the two venæ cavæ, and emptied by its own contraction.
When M. Groux, the subject of the malformation, called on me, on the 18th ult., I formed a very different opinion respecting the cause of the pulsation; and on seeing him again, on the 28th, I became confirmed in my conclusion, which is as follows: When the ventricles contract, the portion of blood which is at their entrance is necessarily driven back into the auricles before the closing auriculo-ventricular valves, and the moment the ventricles become relaxed the blood in the auricles is drawn onwards again into them. It is the wave of blood so driven back into the right auricle by the tricuspid valve, as it is closed by the contraction of the right ventricle, which causes the pulsation seen and felt in the situation of the right auricle, in the case of M. Groux; whilst the relaxation of the ventricle causes the sudden subsidence of the tumour.
The following circumstances, as I consider, prove the above view of the case:--When the hand is placed over the situation of the right auricle, it is felt to pulsate with a force nearly equal to that of the aorta, which can be found by pressing deeply a little higher up in the fissure; but it is impossible that the blood should be propelled from the cavæ into the auricle with a force of this kind. Again, the pulsation, or filling out of the tumour, takes place from below upwards, and slightly from the left side towards the right, whether M. Groux be upright or lying, but this is exactly the direction from the ventricle into the auricle, and not that from the two cavæ. The subsidence of the tumour takes place of course exactly in the opposite direction. Thirdly, the filling of the tumour caused by the right auricle seems to be exactly synchronous with the first sound of the heart and the pulsation of the aorta.
I believe the contraction of the right auricle is not apparent in the case under consideration. I did, indeed, on one occasion, observe a slight motion for a few moments in the intervals between the greater and more apparent ones; but this slight motion, which might have been caused by the contraction of the auricle, disappeared, and I could not again observe it.
It is somewhat curious that there is a difference of opinion amongst the observers of this case, on the other side of the Channel, respecting the exact time when the rise and subsidence of the tumour in the situation of the right auricle takes place; some of the observers stating that the subsidence of the tumour coincides with the impulse of the heart against the wall of the thorax; and Professor Forget stating that the dilation or impulse of the tumour coincides with the impulse of the heart. It is difficult to appreciate a small part of a second of time whilst observing two distinct phenomena at once; but according to the best of my observation, the truth lies between the two opinions. It appeared to me that the impulse or dilation of the tumour occurred just before the impulse of the heart, and the subsidence of the tumour directly after that impulse. The explanation of this is as follows:--the contraction of the ventricles occupies an appreciable part of a second. The closing of the auriculo-ventricular valves, and the impulse in the right auricle above described take place at the beginning of the ventricular contraction, and the impulse of the apex of the heart against the ribs near its conclusion, when the ventricles have injected their blood into the large arteries, and have consequently altered their shape, and are just on the point of relaxing.
There are many interesting points connected with the case of fissure of the sternum that I have not thought it necessary to allude to, as there appears to be no difference of opinion about them. I believe the explanation I have offered above, respecting the chief feature of the case, will remove the cause of disagreement that previously existed, and will show that the phenomena presented by the heart, in this instance, are quite in accordance with the physiology of that organ which is usually taught and received.
I am Sir, your obedient servant,
John Snow, M.D.
Sacksville-street, July, 1855.
Return to John Snow Publications
93."Letter to the right honourable Sir Benjamin Hall, Bart., President of the General Board of Health"
Source: Snow, John. London: Churchill, 12 July 1855.
By John Snow, M.D.
Member of the Royal College of Physicians, and President of the Medical Society of London.
I was ordered, as you are aware, to give evidence before the Select Committee on Public Health Bill and Nuisances Removal Amendment Bill, Of which Committee you were the Chairman. I stated my opinion that certain useful though offensive trades do not cause, or in any way promote the prevalence and mortality of cholera, fevers, and other diseases, which are communicated from person to person, and which, on account of the property of being so communicated, take on very often the form of epidemics. I explained the grounds of my opinions as well as the opportunity permitted. Although I had published the same opinions on more than one previous occasion, and they had received no notice except of approval, I have been subjected since expressing them to the Select Committee to some rather severe attacks, commencing in the newspaper press, and continued in the medical journals.
The writers of these attacks have assumed and asserted that the opinions I have expressed on the subject of offensive trades are altogether new and peculiar. This error might be excused in the editor of a newspaper, but in the editors of the two medical journals who have given a leader on my evidence it is altogether unpardonable. It is only necessary to quote the following passage from page 635 of Dr. Bancroft's work on Yellow Fever, published in 1811, in order to show that my opinions on this point are at all events not new.
"The following statement is extracted from a letter written to the author by Mr. Lawrence, Anatomical Demonstrator at St. Bartholomew's Hospital; whose character, talents, and professional acquirements, have already, at an early period of his life, greatly and justly advanced him on the road to eminence.
"'In a constant attendance at the dissecting room of St. Bartholomew's Hospital, for more than ten years, I have never seen any illness produced by the closest attention to anatomical pursuits, except such as might be expected to follow from a similar confinement and application to any other employment.
"'When it is considered that most of the students come from the country, and that many spend much time in dissection, being employed also in writing, reading, etc., during the rest of the day, it will not be a matter of surprise that their health should occasionally suffer: but the indisposition has never appeared to derive any peculiar character from the exposure of the subject to putrid effluvia. Of course you will except from this observation, the effects which may arise from the absorption of noxious matter from wounds received in dissection. It has not appeared to me that ill consequences of that description follow more frequently from the dissection of the most putrid, than from that of recent bodies. The following particulars will afford the most complete proof, that the exhalations from decomposing animal substances are not necessarily injurious to the human body. John Gilmore, together with his wife, and two sons, lived for ten years in a room under the anatomical buildings of St. Bartholomew's Hospital. The whole family slept, as well as spent the day, in this apartment, which received a very small quantity of light, inconsequence of its single window opening against a high wall. The room was at the end of a passage, in which several tubs containing bones in a state of maceration were generally placed, and with which other divisions of the cellars communicated, continuing large excavations for receiving the refuse of the anatomical rooms. The latter were not separated from the passage by any door.
"'The animal matters thrown into the receptacles last mentioned, are, I believe, converted into adipocere, and the fetor is consequently not so offensive as if they went through the putrefactive process; but the whole place was constantly filled with a close cadaverous smell, very disagreeable to any persons who went down from the fresh air. During the whole day, Gilmore was employed about the dissecting room, in removing the offals, in cleaning macerated bones; in short, in an almost constant handling of putrid matters. He always enjoyed good health, was fat, and possessed very great bodily strength. He left his situation in consequence of an apoplectic attack, and died lately, at the age of 69, after two other similar affections. His wife survives, enjoying a good state of health. Neither of his sons appears to have suffered from any unwholesomeness of their abode. They are both hearty and strong, although they have been employed some years in attending the dissecting room. But the whole family left the cellar soon after the father's first attack.'"
The above facts, detailed by Mr. Lawrence, agree with the experience of all medical men regarding dissection, and the bearing of these facts on the mischief alleged to arise from other occupations connected with decomposing animal matters must be very evident. I could, indeed, if I had time, quote many passages from trustworthy authorities to prove that skin dressing, bone crushing, and other offensive trades are not perceptibly injurious to health; but I have preferred to select the above passage, because the experience and opinion of Mr. Lawrence, who is well known to you as an eminent member of the Medical Council of the General Board of Health, will naturally have more weight with you, than the opinions and evidence of others who might be strangers.
It is hardly necessary to remark that occupations which are not injurious to those who follow them, cannot, by any stretch of the imagination, be considered to do harm to those who merely live in the neighbourhood in which the occupations are pursued. As the gases given off from putrefying substances become diffused in the air, the quantity of them in a given Space is inversely as the square of the distance. Thus, a man working with his face one yard from offensive substances, would breathe ten thousand times as much of the gases given off as a person living a hundred yards from the spot. Currents of air would make a difference; but this would be the average proportion of the gases inhaled respectively by the two individuals. Therefore, if these gases are supposed to act as ordinary poisons, the health of the workman ought to be injured ten thousand times as much as that of the inhabitant a hundred yards from the factory; or if they are supposed to act as specific poisons, having the power of reproduction, so that the smallest quantity might suffice to set up disease, then the chances of contracting such disease would be ten thousand times greater amongst the workmen, than amongst those living at a distance of one hundred yards.
It is sometimes asserted that workmen become inured by habit to offensive trades, and thus escape the diseases which attack others at a distance; but they who use this argument forget that those at a distance ought by habit to become inured to their minute dose as well as the workmen to the larger quantity; and also that the workmen are not inured by habit when they first enter on their trades, and ought then to be affected by their occupation if it really produced fevers and other epidemic diseases; but this is contrary to experience.
The gases which result from the putrefaction of animal substances are capable of causing death, when they are breathed in a concentrated form, and it is often assumed that this of itself proves that they must be more or less injurious in the most minute quantities. This, however, by no means follows, for carbonic acid gas causes instant death when not much diluted, and yet it is a natural constituent of the atmosphere, and is constantly breathed in all parts of the world. Carbonic acid gas is not so powerful a poison as some of the gases resulting from putrefaction; but then the amount of it always present the air is far greater than that in which the gases from putrefying substances are ever met with in the streets and houses nearest to any kind of offensive factory.
The editors who have attacked me have apparently copied each other's sentiments, and they have assumed that my opinions respecting offensive trades are the consequence of the principles I have endeavoured to establish concerning the mode of communication of cholera, typhoid fever, and some other diseases. But this is an error, for I held the sentiments that I now hold respecting offensive trades, for many years before my opinions were formed, on the mode of communication of cholera, at the latter part of 1848; and in this respect I was in no way singular. One of the most approved and largely circulated works on the Practice of Physic, is Dr. Watson's Lectures, which appeared in the Medical Gazette in 1841-2. The following passage will show Dr. Watson's opinions with respect to the alleged connection between fever and offensive effluvia.
"Again, continued fever has been attributed, with great confidence, to a vitiated state of the air, from the putrefaction of dead animal and vegetable substances. Dr. Bancroft deals with and demolishes this error also, showing that neither the putrid atmosphere of the dissecting-rooms (respecting which you must have some personal experience), nor the noisome effluvia from full and ill-conditioned burial grounds, nor those to which tallow-chandlers, soap-boilers, glue and catgut makers, and the melters of whale-blubber, are exposed, nor the foul air of sewers and privies, have ever been known to produce anything like continued fever. In some parts of Essex, near the coast, where the farmers are in the habit of manuring their fields with shoals of sprats, I have seen large tracts covered with these fish in a state of putrefaction. The stench they occasion is horrible; but no disease results. Dr. Chisholm, in a paper to which I can only refer, but which I would recommend you to look at, in the sixth volume of the Edinburgh Medical and Surgical Journal, brings forward other, and very satisfactory, instances, to the same purpose: from a bone manufactory, near Bitton, in Gloucestershire; from an establishment (now relinquished) on the banks of the Avon, for converting the flesh of dead animals into adipocere; from manufactories for refining sugar, where the blood of slaughtered animals is kept for that use by butchers; from the leather-dressing business; all tending, I say, to the conclusion, that air, contaminated by the decomposition of animal substances, is not necessarily noxious to life; still less productive of that specific disease which we are now considering. The old belief, therefore, was unfounded, that the exhalations from the dead and putrefying bodies of men and horses, lying unburied on the field of battle, are capable of producing a pestilence. Many instances to the contrary are on record; one, of an early date, is thus stated by Diemerbroek:--'Anno 1642, in agro Juliacensi maxima strages facta est, et ad minimum 8,000 militum occisa fuerunt, præter majorem adhuc famulorum, etc., numerum: corpora inhumata sub dio computruerunt, nulla tamen pestis insecuta est.'" [In 1642, the greatest massacre took place in the territory of Juliacensi, and at least 8,000 soldiers were killed, besides a still greater number of servants, etc.: the unburied bodies rotted under the sun, but no plague followed.]--Medical Gazette, 1842, Vol.xxx., p.791.
Although there is sufficient direct evidence to prove that cholera is neither caused nor increased by offensive trades,* that circumstance is very much confirmed by the facts which I have been able to collect in illustration of the mode of propagation of cholera; for it is not reasonable to seek for additional causes of any phenomenon, when a real and adequate cause is known. Thus the itch, owing to its being almost exclusively confined to the poor and dirty, is more confined to neighbourhoods where offensive smells prevail, than typhoid fever is, and very much more so than cholera is; yet no one attributes the itch to the gases given off by decomposing animal or vegetable matters, for the simple reason that the real and sufficient cause of that complaint is known.
(*The Registrar-General's sub-district of Lambeth Church, first part, which extends by the river side from Westminster Bridge to Vauxhall Bridge, and contains most of the manufactories that are Complained of in Lambeth, suffered only a mortality of 29 persons in 10,000, in the epidemic of cholera in 1854, whilst the more genteel, open, and thinly peopled sub-districts of Clapham and Kennington, in which few factories are situated, suffered as follows: Clapham, 103; Kennington, first part, 125; and Kennington, second part,76 deaths from cholera to each 10,000 inhabitants. The sub-district of Saffron Hill, with the open Fleet Ditch flowing through it, and the slaughter-houses, knackers' yards, and cat-gut factories of Sharp's Alley, on its eastern boundary, suffered the lowest mortality from cholera in 1854 of any sub-district in London except one. The mortality of the Saffron Hill sub-district was only 5 in 10,000, whilst that of London altogether was 45, and that of the fashionable Belgrave sub-district was 60 in 10,000.)
It appeared to me that you were not sufficiently aware of the bearing that any facts, which should establish a distinct and adequate cause of cholera, would have on the alleged effect of offensive trades in promoting that malady; for when a member of the Select Committee--Mr. Wilkinson, I think--put a question to me respecting the cause of the outbreak of cholera near Golden-square, you did not allow it to be answered, although, undoubtedly, the late epidemic of cholera was the cause of the bills being framed which are now before Parliament.
The absence or defect of drainage, undoubtedly, assists very much in the propagation of many epidemic diseases, and as defective drainage very often occasions offensive smells, the editors of whom I complain have arrived at the short and easy conclusion that any trade or manufacture, which gives rise to an offensive odour, must also promote disease. The matters, which it is the purpose of drainage to remove, contain all that comes from the sick, as well as the healthy part of the community, and, when they are not properly removed, they permeate the ground, and pollute the pump-wells and other supplies of water and, in this way, as I have elsewhere adduced a good deal of evidence to prove,* several epidemic diseases may be propagated; the morbid matter of each disease reproducing its own specific malady.
(*On the Mode of Communication of Cholera.)
There are also other ways more gross and material than a mere odour, by which the absence of proper drainage aids in the spread of disease. On the other hand, occupations connected with the skins, bones, or fat of dead animals, cannot in any way assist in conveying the morbid matter of disease from the sick to the healthy.
I am, of course, no defender of nuisances, but I consider that if a trade is more offensive than it ought to be, or is conducted in a place where it has no right to be, it might be proceeded against by the ordinary laws as a nuisance, without using the word pestiferous, or otherwise dragging in and distorting the science of medicine.
Some of the manufacturing processes which give rise to offensive smells, are not only a source of wealth in themselves, but are highly useful to agriculture. These are circumstances that would, at one time, have been thought worthy of consideration, but, however desirable it may be that commerce and agriculture should not be injured on mistaken grounds, it is still more important that the real causes which affect the health of the community should be ascertained, and that epidemics should not be attributed to a wrong cause, for I have previously shown that great increase of disease has several times been occasioned by presumed sanitary measures.
I have of course not written this letter in the way of personal complaint against the editors by whom I have been attacked. My reason for writing it is, that I have an impression that the editors in question have really expressed the sentiments of the majority of the persons who have paid little attention to the subject, but are more likely to influence legislation than careful and industrious observers.
I have the honour to be, Sir,
Your obedient servant,
John Snow, M.D.
Sackville Street, July 12th, 1855.
Return to John Snow Publications
94."Further remarks on the mode of communication of cholera; including some comments on the recent reports on cholera by the General Board of Health"
Source: Snow, John. Medical Times and Gazette 11, 14 July 1855, pp.31-35. Part 1.
A substantial portion of this essay was first read at the Epidemiological Society of London in May and June, 1855.
Part 1
In a paper which I had the honour to read to this Society in 1851,* I enumerated various circumstances connected with the pathology of Cholera, and with its progress as an epidemic, which led me to the conclusion that it is propagated by the morbid poison which produces it being accidentally swallowed; that this morbid poison becomes multiplied and increased in quantity on the interior surface of the alimentary canal and that it passes off in the ejections and dejections to produce fresh cases of the disease in those who happen to take the morbid matter into the stomach. I explained what great facilities there are for the cholera evacuations being accidentally swallowed in the crowded habitations of the poor, where the inmates cook, eat, live, and sleep in the same apartment, and pay little regard to washing the hands, since these evacuations are almost devoid of colour and odour, and are usually passed involuntarily in the latter stages of the disease. It is in the families of the poor that cholera is often observed to pass from one individual to another, while in cleanly dwellings, where the hand-basin and towel are in constant use, and where the rooms for cooking, eating, and sleeping are distinct from each other, the communication of cholera from person to person is rarely observed. In the houses of the poor, also, the disease is hardly ever contracted by medical, clerical, and other visitors, who do not eat or drink in the sick-room, while it often fares differently with the social visitor, who comes either to see the patient or attend his funeral.
(*Published in Medical Times and Gazette, 1851, Vol. II.)
The cholera has visited the mining districts of this country with unusual severity, in each of the epidemics we have had. The following is the explanation of this circumstance:--The pits are without any privies, and the excrement of the workmen lies about almost everywhere, so that the hands are liable to be soiled with it. The pitmen remain under ground eight or nine hours at a time, and invariably take food down with them into the pits, which they eat with unwashed hands, and without knife and fork; therefore, as soon as a case of cholera occurs among any of the pitman, the disease has unusual facilities of spreading in the way I have pointed out.
In my former paper I also showed that the cholera evacuations have the property of communicating the disease after being mixed with the drinking-water of the people, and I related a number of instances in which sudden and severe outbreaks of the malady occurred in the epidemics of 1832 and 1849 among persons using the water of ditches and pump-wells contaminated with excrementitious matters. It is particularly to be remarked that, in those instances, there were one or two cases of cholera in the community where evacuations polluted the water, just before the great out-break. I also related a number of facts to show that cholera was communicated through the water supplied to many districts of London, and to several other towns where the water was obtained from a river receiving the sewage of the town. This division of my views on cholera which refers to its communication through the medium of drinking water, has apparently obtained a greater amount of attention from the Profession, than my views respecting its more immediate communication by the cholera poison being swallowed without the water. While I speak on this division of the subject, however, I must beg the Society to bear in mind also the other part of my views, first alluded to, for I am well aware that the part which relates to polluted water will not of itself explain the whole progress of the disease as an epidemic.
The epidemics of 1853 and 1854 have furnished numerous examples of the communication of cholera by means of water quite as striking as those which I related in my former paper; but I shall be content on the present occasion to describe only a single example which occurred on a large scale, and shall merely make such remarks on some other instances, as may be necessary to elucidate the way in which the water produces its effects.
The whole of the south districts of London, with the exception of the Greenwich district, and part of the Lewisham and Rotherhithe districts, are supplied with water by two water companies, one called the Lambeth Company, and the other the Southwark and Vauxhall Company. The population of the districts supplied by these two water companies, amounted in 1851 to nearly half-a-million. Now throughout the greater part of the districts supplied by these two water companies, the supply is intimately mixed, the pipes of both companies going down all the streets, and into almost all the courts and alleys. The water companies were at one time in active competition, and any person paying the rates, whether landlord or tenant, could change his water company as easily as his butcher or baker, and although this state of things has long since ceased, and the companies have come to such an arrangement that the people cannot change their supply, yet the result of the former competition remains. There is here and there a row of houses having the same supply, but very often two contiguous houses are supplied differently. There is no difference in the circumstances of the people supplied by the two companies; each company supplies both rich and poor alike.
In 1849 the water supplied by the two companies was nearly the same; that of the Lambeth Company was obtained from the Thames, close to Hungerford Suspension Bridge; and that of the Southwark and Vauxhall Company at Battersea-fields: each kind of water contained the sewage of London, and was distributed with very little attempt at purification, as the most superficial examination was enough to show. The cholera in 1849 was almost equally severe in the districts which were entirely supplied by the Southwark and Vauxhall Company, and those which were partly or chiefly supplied by the Lambeth Company. This latter company had no district, or even sub-district, exclusively to itself, and although it has since extended its supply to the sub-districts of Streatham, Norwood, Dulwich, and Sydenham, these villages are chiefly supplied by pump-wells.
Between the epidemic of 1849, and that of 1853, a very important change was made in the water supply of a great portion of the south districts of London. The Lambeth Company removed their works in 1852 from the neighbourhood of Hungerford Bridge to Thames Ditton, which is situated above Teddington Lock, and is, therefore, beyond the influence of the tide, and out of reach of the sewage of London.
Dr. Farr turned his attention to the influence of the water-supply on the mortality from cholera in London soon after my pamphlet, containing remarks on the subject, appeared in 1849. He returned to the subject in the latter part of 1853, and the weekly returns of that time contain some tables, showing that the districts, partly supplied with the improved water from Thames Ditton, suffered a lower mortality than those supplied exclusively with the water from Battersea-fields. It was desirable, however, to investigate this matter more in detail, and to find out, if possible, what was the actual water-supply in the houses in which fatal attacks occurred. I was unable to do this in the epidemic in the last quarter of 1853, but when the cholera returned to London in the following summer, I resolved to call myself at the houses in which deaths might occur, in the districts where the water-supply is intermingled in the way I have explained. The addresses of the persons who died of cholera during the first four weeks of the epidemic of 1854 were published in the weekly returns, and on applying to Dr. Farr, I was kindly permitted to copy those of the persons whose deaths were registered during the next three weeks. My inquiries thus extended over the first seven weeks of the epidemic, that is, from the 8th of July to the 26th of August. The number of deaths I inquired after personally amounted to 658; but as the water companies make no return of the number of houses they supply in particular parishes or districts, it was necessary, in order to find out the exact influence of the water, to extend the inquiry to all the districts to which the water of either company is distributed, in order that the number of fatal attacks might be compared with the entire number of houses supplied by each company, as shown by their returns to Parliament at the conclusion of l853, namely, 40,046 by the Southwark and Vauxhall Company, and 26,107 by the Lambeth Company.
I was assisted by a Medical man, Mr. Whiting, in making the inquiries respecting the water-supply in certain districts supplied only by the Southwark and Vauxhall Company; but I made the inquiry myself in all the districts to which the water of the Lambeth Company extends; so that Mr. Whiting's part of the inquiry, which he conducted very carefully, was merely to ascertain whether the houses, in which fatal attacks took place, were supplied by the Southwark and Vauxhall Company, or by a pump-well, or some other local supply. In the case where persons died in an hospital or a workhouse, to which they had been removed after the attack, the water-supply of the houses from which they had been removed was ascertained.
In stating the results of these inquiries, I shall divide the seven weeks over which they extended into two periods, giving the result of the first four weeks of the epidemic first, and then that of the succeeding three weeks, as the cholera was more exclusively caused by the water in the beginning of the epidemic than afterwards, for reasons that I shall state. I shall also treat separately of the groups of districts, according as they were supplied by only one of the companies, or by the two combined.
In the first four weeks of the epidemic there was not a single death from cholera registered in the sub-districts supplied by the Lambeth Company, and not supplied by the other company. In the sub-districts, in which the supply of the two companies intermingled, in the way I have explained, there were 134 deaths from cholera registered during this period, and I ascertained, by calling at the respective houses in which the fatal attacks occurred that the water supply in 115 of the cases was that of the Southwark and Vauxhall Company, in 14 cases that of the Lambeth Company, in 2 cases from pump-wells, and 1 direct from the river, and in 2 instances it was not ascertained, as the place of attack was unknown. In the sub-districts which are supplied solely by the Southwark and Vauxhall Company, there were 200 deaths during the first four weeks of the epidemic, of which 171 had the supply of that company, and the rest had water direct from the river, or from pump-wells, or ditches.
In the next three weeks of the epidemic, from the 5th to the 26th of August, 18 deaths from cholera were registered in the sub-districts supplied by the Lambeth Company alone; of these 4 occurred in houses having the supply of that company, and the houses in which the others occurred were supplied from pump-wells or other sources. In the sub-districts in which the supply was intermixed, 518 of the fatal attacks of cholera occurred in these three weeks, of which I ascertained that 410 took place in houses having the supply of the Southwark and Vauxhall Company, and 80 in houses having the supply of the Lambeth Company, while the remaining 28 occurred in houses not supplied by either company, or of which the address was not known. During this period 644 fatal attacks occurred in the sub-districts supplied exclusively by the Southwark and Vauxhall Company, of which 567 happened to persons having the supply of the company, and the remaining 77 to persons obtaining water direct from the river, or from some other source.
It is to be regretted that we have not yet the exact number of houses supplied by each water company respectively, in those sub-districts in which the supply is intimately mixed up, as it is there that the investigation approaches completely to a crucial experiment. Dr. Farr has all the data for ascertaining this point, and I hope it will soon be worked out. In the mean time, however, we can arrive very nearly at the truth by the help of the Census tables. The entire number of inhabited houses in the sub-districts in which the water supply is intermixed was 44,686 at the time of the last census, and there were 3079 houses in the sub-districts which were supplied by the Lambeth Company to the exclusion of the other. These latter sub-districts, namely, Streatham, Norwood, Dulwich, and Sydenham, are chiefly supplied by private pump-wells, not more than one house in five at the utmost being supplied by the company; therefore, if we deduct one-fifth of the above from the entire number of houses which the Lambeth Company supplies, we shall have 25,491 as the number of houses which that company supplies out the 44,686 which were contained in the districts and sub-districts where the supply is intermixed; leaving 20,555 as the number supplied by the Southwark and Vauxhall Company. Some houses were built in a few of the less crowded sub-districts, between the time of the Census and the epidemic of 1854, but these are probably quite counterbalanced by a certain number of houses in Kennington and Brixton, which have a pump-well, and are not supplied by either company.
The 115 fatal attacks which occurred during the first four weeks of the epidemic in the 20,555 houses we have calculated to be supplied by the Southwark and Vauxhall Company, give 55 to every 10,000 houses, and the 14 fatal attacks which occurred in the 25,491 houses supplied by the Lambeth Company give 5 to each 10,000 houses; the cholera was therefore eleven times as fatal in the houses having one supply as the other. If we make a similar calculation with regard to the fatal attacks which occurred in the next three weeks in the sub-districts in which the water supply is intimately mixed, we find that the mortality of cholera was at the rate of 199 to each 10,000 houses supplied by the Southwark and Vauxhall Company, and 31 to each 10,000 houses supplied by the Lambeth Company. It was, therefore, between six and seven times as great during this period, to the population having one supply as to that having the other.
I will now state the results when the whole of the districts supplied by each of the companies are taken together, and compared with the entire number of houses supplied by each. In this way we get figures that are perfectly correct, and not merely a close approximation to the truth.
In the first four weeks of the epidemic there were 334 deaths from cholera in the districts to which the supply of the two water companies extends. Of these 286 were attacked while living in houses supplied by the Southwark and Vauxhall Company with water from the Thames at Battersea-fields, and only 14 in houses supplied with water from Thames Ditton. In 4 cases the houses were supplied with water from pump-wells, in 26 cases the water was drawn directly from the river or from ditches, and in 4 cases the supply could not be ascertained, as the place of attack was unknown. When the number of houses supplied by each of the companies respectively is taken into account, it is found that the cholera was 14 times as fatal in the houses receiving the water from Battersea-fields, and containing whatever might come down the sewers or over the side of a ship from cholera patients, as it was in the houses receiving the water from Thames Ditton.
I published the address of the houses in which the whole of the above 334 fatal attacks took place, appending the particulars of the water supply, and I have not heard that the correctness of the report has been called in question in a single instance.
The 286 cases occurring in the houses supplied with the water of the Southwark and Vauxhall Company were distributed over the whole area to which the water extends, reaching from Wandsworth to Rotherhithe inclusive; and this continued to be the case throughout the epidemic.
It is worthy of remark that while only 563 fatal cases of cholera occurred in the whole of this metropolis, containing over 300,000 houses, during the four weeks ending August 5th, 1854, 286, or more than one-half of the entire number, occurred in the 40,046 houses supplied by the Southwark and Vauxhall Company, while a great number of the remaining cases occurred in persons employed on the river, and drawing their drinking water from alongside the ship or barge. In the next three weeks of the epidemic, from the 5th to the 26th of August, 1180 deaths from cholera were registered in the districts of which I am treating. Of these fatal attacks, 977 took place in houses supplied with the water of the Southwark and Vauxhall Company, and 84 in houses supplied with the improved water of the Lambeth Company; there were 25 fatal attacks in houses supplied merely by pump-wells; in 76 cases, the water was obtained from the Thames, or from ditches, and in 18 cases the supply could not be ascertained, for the reason stated before.
When the number of houses supplied by each company respectively, is taken into account, it is found that in those three weeks, from the 5th to the 26th of August, the cholera was eight times as fatal in the houses supplied with water from Battersea-fields as in those supplied with the more pure water from Thames Ditton, the proportions being 241 fatal attacks in each 10,000 houses supplied with the former water, and 32 fatal cases in each 10,000 houses supplied with the latter.
An inquiry respecting the water supply in the house of attack, in all fatal eases of cholera, was made by the Registrar-General, through the district Registrars of all the south districts of London, beginning from the 26th of August, the day when my inquiry was left off. There were a considerable number of cases in which the supply could not be ascertained from the person registering the death, owing chiefly to the water-rates being "farmed," as the term is, but there is no reason to doubt that the returns were correct, so far as they went, and showed the same proportion as they would have shown if more complete. From the 26th of August to [33/34] the end of the epidemic, a period of ten weeks, 2443 cases were returned to the Registrar-General, in which the water supply in the house of fatal attack was that of the Southwark and Vauxhall Company, and 313 cases in which the supply was from the Lambeth Company; consequently, during this period, there were 610 fatal attacks in each 10,000 houses supplied by the former company, and 119 in each 10,000 houses supplied by the latter, and the malady was, therefore, more than five times as fatal to the population having water from the Thames at Battersea-fields, as to the population having the new supply, free from the sewage of London. (*[33]In my inquiries, I made use of a chemical examination of the water in all cases where the other evidence was not quite conclusive. The Lambeth water contained rather less than a grain of common salt in each gallon, while the water of the Southwark and Vauxhall Company contained nearly forty grains. I ascertained afterwards from the information of Mr. Quick, the Engineer to the latter company, and from some examinations I made of the Thames water taken direct from the river, that the common salt was nearly all derived from a mixture of sea-water, owing to the extreme dryness of the season, which caused it to flow higher up the river than usual. When, Messrs. Graham, Miller, and Hofmann examined the water of the Southwark and Vauxhall Company, at the latter part of January, 1851, it contained rather less than two [33/34] grains of common salt. It has been objected (Brit. and Foreign Med. Rec., April, l855) that the water of the two companies might alter from day to day, and that I ought to have examined that in their reservoirs; but, besides that it would be impossible for the sea-salt to be elevated over Teddington Lock, and extremely improbable that the Thames in London should take on, in the middle of a dry autumn, the character it had in a wet winter, an examination of numerous specimens throughout the district is as good proof of the nature of the water supply as one made at the reservoirs. I am, however, able to say that the two kinds of water existed throughout the district during the whole time of my inquiries, and were characteristic of their respective sources, for I examined very numerous specimens where the other evidence was conclusive, independent of that derived from chemistry. The mere appearance of the water was generally enough to indicate its origin, but I never relied on that alone.)
It will be observed that, while the disproportion between the number of fatal attacks in the houses supplied respectively by the two kinds of water remained very striking to the last, yet that it somewhat diminished with the progress of the epidemic, being fourteen times as great in one class as in the other, during the first four weeks of the epidemic, eight times as great during the next three weeks, and more than five times as great during the last ten weeks. The reason of this is, that as the number of cases increased, the opportunities of taking the disease directly from the patient in the manner I first pointed out, increased also. The proportion of deaths in houses supplied by the Lambeth Water Company increased during the progress of the epidemic, just as it did in parts of London having a water supply which took no share in the propagation of cholera, as the central and north districts supplied by the New River Company.
The Registrar-General calculated from the Census returns the number of persons living in the houses supplied by the two water companies mentioned above; and by this means we are enabled to compare the mortality of these parts of the population with that of the rest of London, which is estimated according to the number of the people, and not of the houses. The mortality of London generally in the late epidemic was 44 to each 10,000 inhabitants; among the population supplied by the Southwark and Vauxhall Water Company it was 157 to each 10,000 inhabitants, while it was only 27 to each 10,000 persons having the supply of the Lambeth Water Company. The preponderance of deaths in the south districts over the other parts of London, was caused entirely by the mortality among the customers of the Southwark and Vauxhall Water Company; and it is extremely deserving of notice, that the customers of the Lambeth Water Company, although intimately mixed up with those of the former company, retained an immunity from cholera throughout the epidemic, not only greater than that of London at large, but greater than that of any of its divisions, except the central and north districts above alluded to, which are supplied by the New River Company with water receiving no town drainage whatever, and not even navigated by people living in boats. This circumstance confirms me in the conclusion which I expressed in a former paper to this Society, that the remarkable relation of an inverse nature, which Dr. Farr discovered to exist between the elevation of the soil, and the mortality of cholera in the metropolis, depended entirely on the relative purity or impurity of the water; taking into account not only the supply of the companies, but also that drawn from the Thames and tidal ditches, and that of the pump-wells, which are most liable, to pollution in the low-lying districts.
In the Report of the late General Board of Health on the Water Supply of the Metropolis, published in 1850, the following passage occurs, at page 130: "We could find no evidence to justify the supposition that the aggravated effects of cholera, in the lower districts, was to be attributed to persons drinking pipe-water, which, in fact, very few people do habitually drink." The latter part of this passage I found in my inquiries last year in the South Districts to be erroneous, for there were very few pumps in use, until one came to the more distant and suburban parts; in the more densely peopled parts of Lambeth, Southwark, and Bermondsey, the people seldom had any other water to drink than that of the cistern or water butt, and the mortality was greatest among children and others who drank it unboiled. As regards the influence of the pipe-water itself, I believe that, since the inquiries of last summer above alluded to, especially that part of them made and published by the Registrar-General, it has been generally admitted. In the recent Report of Dr. Sutherland, published by the present Board of Health, both the author himself, and every one of the Inspectors whom he quotes on the subject fully admit the influence of the impure water of the Southwark and Vauxhall Company on the prevalence and mortality of cholera, although they do not admit the explanation which I give of this influence. It only remains, therefore, for me to prove that this impure water can increase the prevalence and mortality of cholera in no other manner than that which I explained at the beginning of this paper, and I shall have established my point. I should first like to remark, however, that although a scarcity of water for such purposes as washing out dirty courts and alleys had often been complained of, I am not aware that the quality of the water supplied from any water-works had ever been suspected of actually promoting the prevalence of cholera, or any other epidemic disease, before I published my views on its pathology and mode of communication in August, 1849. So far was this from being suspected, that the most approved measure for preventing cholera in London was that of abolishing common privies and cesspools, in order to remove offensive odours, and by substituting water-closets, to send the evacuations of both the sick and healthy, as quickly as possible into the Thames, although it was well known that about half the metropolis were drinking the water of this river.
As far as I am aware, it is these views which have led to a knowledge of the injurious effect of water under certain conditions, and I would therefore suggest that they are worthy, on this account, of some amount of consideration from those who do not yet admit their entire truth. I would even suggest that this result of the views I entertain affords of itself a presumption that they are correct.
But to proceed to the proofs to which I alluded. There are very numerous facts to show that mere impurity in the water does not of itself increase the prevalence of cholera, even when that impurity consists of the contents of sewers and cesspools. The greater number of the shallow pump-wells of this metropolis contain a good deal of organic matter from the neighbouring sewers, house-drains, and cesspools, in fact, the ground being covered up with houses and pavement, they are chiefly fed from these sources, but they do not, as a general rule, take any share in the propagation of cholera during an epidemic; it is only here and there, when one of them happens to receive what comes from a cholera patient, that it communicates the malady to those drinking the water. Persons often allow the water in their cisterns and butts to become extremely foul and dirty, but this has no effect in promoting the disease, provided the water be originally of a kind, like that of the New River, which never contains anything proceeding from cholera patients.
It follows, therefore, that mere impurity in the water does not predispose to, or in any way increase the prevalence of, cholera; and that the disease, when influenced by the water, is really due to the specific cause of cholera contained in the water.
Those who dissent from the opinion, that the water promotes the prevalence and fatality of cholera, by containing the specific cause of the disease, generally believe that the ordinary impurities in the water act as what they call a predisposing cause. But a predisposing cause is one which is supposed to prepare the patient to be acted on by some more direct cause; and it must, therefore, require a certain time for its operation. But I met with many instances last summer of persons being fatally attacked with cholera in the south districts of London, very soon after arriving from a healthy part of the country, and drinking the water of the Southwark and Vauxhall Company. Some of them were attacked within forty-eight hours after their arrival. Many cases occurred also in the neighbourhood of Broad-street, Golden-square, last autumn, of persons who were not in the habit of drinking the water of the pump in that street, who yet were fatally attacked with cholera after taking the water contrary to their [34/35] usual position. I have notes of many such instances, but will mention only one, that of a family of three persons, at 51, Poland street, who were all attacked on the 1st of September, and died on the same day. They were not in the habit of drinking the water from this pump, but had a jugful on the evening of August 31. My informant was the brother of the deceased woman. He fetched the water on one of those evenings, and saw a sister who survives go for it on the other evening. There were several instances also of families and individuals who were in the constant habit of drinking it at the time of the great outbreak of cholera, escaped the malady. The above circumstances show that the water did not act as a predisposing cause, but must have contained the real and efficient cause of the cholera.
Anything which is supposed to act as a predisposing cause is generally believed to produce its effects by lowering the general health and reducing the strength; but observation shows that cholera attacks individuals of all kinds indiscriminately, when they are exposed to the influence of its specific morbid poison. We may ascertain, from a table constructed by Dr. Guy, that in 1849, some of the occupations which suffered more from cholera that any others were those in which the men are extremely strong and robust, and follow an out-door employment. The seamen and ballast-heavers suffered excessively; 1 in 24 of their whole calculated number died; whilst the coalporters and coalheavers suffered nearly as much, since 1 in 32 of their number died. In the last epidemic also, the men in these occupations suffered severely, but the numbers have not yet been calculated. The reason of those persons suffering so excessively from cholera is, that they draw the water they drink from alongside the ship, and, therefore, have a greater chance of getting the cholera poison in a fresh and unimpaired state, than when it has to pass through the reservoirs and pipes of a water company. It is quite evident to any one acquainted with these men, that the Thames water does not produce cachexia, or gradually undermine the strength.
[Part 2 appeared in the 28 July issue.]
Return to John Snow Publications
95."Further remarks on the mode of communication of cholera; including some comments on the recent reports on cholera by the General Board of Health"
Source: Snow, John. Medical Times and Gazette 11, 28 July 1855, pp. 84-88, Part 2.
Part 2
Another circumstance, which shows very forcibly that the impure water produced its deleterious effects in time of cholera in no other way than by conveying the real material cause of the disease, is, that in the outbreaks caused by the contamination of a pump well, or other local supply of water, nearly all the cases occur together. The water in nearly all these outbreaks had been habitually contaminated for a length of time, and, if it acted as a mere auxiliary cause of cholera, it would increase the prevalence of the malady during the whole time of its existence in the town or neighbourhood, instead of which, without any chemical or physical alteration in the water, a sudden outbreak of cholera takes place among those drinking it; and in most of the instances, as in that at Surrey-buildings, Horseleydown, in 1849, and in that last summer in the neighbourhood of Golden-square, it has been found that the evacuations of a cholera patient were among the impurities which entered the water just before the outbreak. When the cholera is communicated through the medium of a large river, and the pipes of a water company, this sudden kind of outbreak, or increase of the disease, does not of course take place, but the disease gradually increases, as the number of fresh cases add fresh germs or particles of cholera poison to the water, and thereby increase the chances of a person getting one. The time when the epidemic begins to decline is usually that when, on account of a diminution of temperature, persons begin to leave off drinking unboiled water.
Another evidence of the way in which impure water must act in promoting cholera, is the fact itself of cholera being a communicable disease, as is proved by numbers of instances of overwhelming weight. For in itch, syphilis, small-pox, measles, and other communicable diseases, we do not look about for necessary or predisposing causes, but acknowledge in the reproductive morbid material of the disease its sole and sufficient cause. Any circumstance, therefore, which determines the attack of cholera may be presumed to do so by conveying the specific cause of the disease, especially where there is other evidence in favour of this event.
If this point is shown to be established, namely, that impure water increases the prevalence and fatality of cholera, by conveying the morbid poison from one patient to another, then the circumstance of the disease being communicated by swallowing the morbid poison with the food that has been touched with unwashed hands, or otherwise contaminated by the cholera evacuations, is also fully established; for it cannot be supposed that any poison, whether a morbid one or not, could produce active effects when mixed with an almost indefinite quantity of water, and not produce its effects also without the water. If the views I am explaining be correct, we have, therefore, the power of avoiding cholera as easily as one may avoid the itch. Every man may be his own quarantine officer, and go about during an epidemic among the sick almost as safely as if no epidemic were present.
In the recent Report on Cholera to the General Board of Health, by Dr. Sutherland, after saying--"It is believed by some that the water which induces cholera contains the specific poison of cholera in it," and that others consider the impure water only a predisposing cause, continues as follows: "The matter in dispute is really of no practical value, for if it be a fact that the use of impure water is injurious to the public health, the manner of its action is of very secondary importance, at least for practical purposes." P. 40.
It seems very curious that Dr. Sutherland should not have perceived that this question, as to whether or not the water contains the specific cause of cholera, involves the entire question of the cause and prevention of the malady, and also the approval or condemnation of nearly all the so-called sanitary measures which have been adopted with respect to cholera, since it was first expected in 1830.
There are some remarks in Dr. Sutherland's report respecting the south districts of London which require to be noticed, because they refer to the subject of which I am treating, and also because some of them are not quite correct. Quoting from an unpublished report by Dr. Greenhow, Dr. Sutherland says: "After the epidemic of 1849, Christchurch parish was exclusively supplied with the new and comparatively pure water of the Lambeth Company, while St. Saviour's continues to be mainly supplied with the impure water of the Southwark and Vauxhall Company," Now this is an error; Christchurch parish is not entirely supplied with the Lambeth water, as there are some houses in every part of the parish supplied with the water of the Southwark and Vauxhall Company. There is no district or sub-district nearer than Streatham, Norwood, Dulwich, and Sydenham which is supplied exclusively by the Lambeth Company. This is important as regards Christchurch, because there was a very high mortality among the minority having the impure water, and a very low one among the majority having the water from Thames Ditton. St. Saviour's is not mainly but exclusively supplied with water by the Southwark and Vauxhall Company; this error is, however, of less importance than the other. Dr. Sutherland, continuing to speak for Dr. Greenhow, says: "During the late epidemic the mortality in St. Saviour's had advanced from 73 to 97 in 10,000, while the mortality of Christchurch had fallen from 100 in 10,000 to 44 in 10,000, of population." Striking as this difference in the numbers appears, it is much greater when it is known that a great proportion of the deaths in Christchurch occurred in the comparatively few houses having the impure water supply of the Southwark and Vauxhall Company. In the first four weeks of the epidemic there were three deaths from cholera in Christchurch parish, two of which occurred in houses supplied by the Southwark and Vauxhall Company, and one in a house supplied with the water of the Lambeth Company. In the next three weeks twenty-two deaths occurred; nine of the attacks took place in houses supplied by the Southwark and Vauxhall Company, twelve in houses supplied by the Lambeth Company, and one in a house where the inmates begged water all round, as the supply was cut off. Mr. Greenwood, the Registrar of Christchurch, also made an inquiry respecting these eases, and, on comparing our notes, we found that our results coincided respecting the water supply in every instance.
Dr. Sutherland continues as follows:--"This great difference is sufficiently striking; but, while admitting the beneficial results of the purer water, Dr. Greenhow considers it not to be entirely due to the water alone, for Christchurch parish has been improved in other respects of late years, by the covering over of a pestiferous ditch which formerly occasioned a great deal of atmospheric impurity in the neighbourhood, and by other sanitary measures."
Now, leaving out the fact that there are no open ditches in St. Saviour's, with its recent high mortality, if Dr. Greenhow had been aware that the small number of persons in Christchurch who received the impure water of the Southwark and Vauxhall Company suffered as high a mortality as a similar number in 1849, and that the population having the improved water were enjoying only the same amount of immunity as the inhabitants who had the same water in Lambeth Church, first part, amongst the bone-crushers and skin-dressers; or, the ragged, bare-footed people in the streets near the Cornwall-road, in the sub-district of Waterloo-road first part, he would have had no reason to suppose that the ditch had any share in propagating cholera in 1849. I believe that open ditches, which receive the dejections of cholera patients, do sometimes assist in the communication of that disorder, not only when people drink out of them, but also when children can get down to the edge, to pick out their marbles and other toys, and afterwards clean their hands with their tongues before showing themselves at home; but the above circumstances would seem to show that the ditch in Christchurch was not of either of these characters.
Dr. Sutherland proceeds, still quoting from Dr. Greenhow; he says:--"In proof that impure water, though a predisposing cause of cholera, does not act as a specific poison in producing cholera, Dr. Greenhow adduces several instances in which houses supplied by the Lambeth water suffered from cholera, while those supplied by the Southwark and Vauxhall water escaped."
These instances may be correct, notwithstanding Dr. Greenhow's mistake respecting the water supply of Christchurch and St. Saviour's; but I have to submit that the suffering or exemption from cholera in particular houses, whilst it bears on the question of the influence of the water, has no relation to the manner in which the influence is exerted. That is a question which must be decided by other means. The water of the Thames never became as full of the cholera poison as to affect persons in all the 40,000 houses supplied by the Southwark and Vauxhall Company, therefore the exemption of some of these houses was a matter of course; and, as the persons living in houses supplied with the Lambeth water were exposed to at least the same opportunities of taking cholera, as those living in the districts supplied with the New River water, and other water which could have no effect in propagating cholera, it was equally a matter of course that some cases should occur in houses supplied with water by the Lambeth Company. It must also be recollected that the people having this last-mentioned water were not prisoners in their houses. Mixed up as these houses are with others having the impure water of the Southwark and Vauxhall Company, it is not unreasonable to suppose that they would be liable to take the other water. Out of the very few fatal cases occurring in houses supplied with the Lambeth water, in the early part of the epidemic, one was that of a carman who was constantly going about, and took none of his meals at home except his supper, and another was a journeymen baker, who drank no water at home except in his tea, (of course boiled,) but he drank a great deal of cold water when at his work.
I have previously stated that, in the first four weeks of the epidemic, the fatal cases of cholera were fourteen times as numerous in a given number of houses supplied with the Vauxhall water, as in the same number supplied with the Lambeth water from Thames Ditton; and it is by no means improbable that out of every fourteen drinks of water taken at that time, one drink might be of a kind different from that supplied at the house of attack, to say nothing of the use of water for making and adulterating beverages which are vended.
I find from some further quotations which Dr. Sutherland makes, that I have the happiness of agreeing with Dr. Greenhow as to the effect of the impure water, though not as to its mode of action. Dr. Greenhow states that the use of the Southwark and Vauxhall water very greatly aggravated the pestilence; and further he says, "although, doubtless, the unwholesome water has much aggravated the result, it is only one cause among several." I believe no one ever supposed that impure water was the sole cause of cholera, and, for my part, I do not consider it a cause at all, but only a frequent medium or vehicle of the one true cause of the disease, namely, the reproductive cholera poison.
In speaking of sanitary improvements, Dr. Sutherland makes the following remark:--"Mr. Walsh states that Jacob's Island, Bermondsey and its immediate neighbourhood, suffered much less during the late epidemic, notwithstanding its greater severity, than it did during either of the two former visitations, which he says is attributable, without doubt, to the filling up of the foul tidal ditch, since the epidemic of 1849."
Judging from what Mr. Walsh stated on a former occasion in this Society, it is most likely that he would mention in his report the fact of a number of the inhabitants of Jacob's Island and the neighbourhood drinking the water of these ditches in 1849, but if so, Dr. Sutherland has not quoted this in his report; and as the quotation now stands, it would be understood by nearly every reader to imply that the aggravation of cholera in this neighborhood, in 1849, was caused by effluvia from the ditches; and that the improvement in l854 was due to improvement of the air, by the ditches being filled up. I have, however, the results of a statistical inquiry to show that such was not the case. The Metropolitan Commissioners of Sewers caused an inquiry to be made, at the close of the epidemic of 1849, into the effects of using the water of these ditches; and Mr. John Grant, the Assistant Surveyor to the Commissioners for Kent and Surrey, was kind enough to favour me with the result. In Jacob's Island, and the streets immediately surrounding the ditches, there were 7286 inhabitants. Of these there were 865 individuals having no other supply of water than the ditches, and the remaining 6421 had the supply of the Southwark and Vauxhall Watar Company, or were supplied by private pumps. During the first nine months of 1849, 18 deaths took place from cholera, [85/86] and 8 deaths from other causes, amongst the 865 persons having no water supply but that of the ditches; and 95 deaths from cholera, and 46 from other causes, amongst the 6421 persons having another supply. The mortality from cholera was, consequently, at the rate of 208 in 10,000 amongst the persons using the ditch water, and 147 in 10,000 amongst the inhabitants who had the supply of the Southwark and Vauxhall Company, or that of private pumps. The mortality of the population living amongst and around the ditches, but not drinking the water, was, in fact, almost exactly the same as that of the other inhabitants further removed from the ditches; whilst that of the people who were obliged to drink the water was more than one-third higher; as the following figures from the Report of the Registrar-General show. St. James's, Bermondsey, in which Jacob's Island is situated, suffered a mortality from cholera of 142 in 10,000, St. Mary Magdalen, Bermondsey, a mortality of 159 in 10,000, and the Leather Market sub-district of Bermondsey a mortality of 160 in 10,000.
The ditches were of considerable extent, and as wide as an ordinary canal. The water had been formerly used for turning the wheel of a mill, as it flowed back into the river, but of late years the ditches were usually kept full, and only emptied at intervals. During the time of my visits in August and September, 1849, when the cholera was at the worst, they were not emptied at all, and no mud was exposed. The water of the Thames, admitted into these ditches, received the sewage of the surrounding population, either directly, by the privies overhanging the ditches, or through channels and drains. Thames water emits no smell, although the odour of exposed mud, and that from the mouths of sewers, sometimes leads persons to suppose it does.
The water of the ditches around Jacob's Island, although richer in manure than that of the Thames, did not seem offensive, so far as I could perceive; and if the ditches had been filled with black stinking mud, I believe they would not have increased the prevalence of cholera, as it could then have been impossible for the people to drink the water, and thus to imbibe the cholera poison coming from the cases in the neighbourhood. As it was, the water became moderately clear after standing in a vessel for a few hours, as the persons who were obliged to use it generally allowed it to do. Many of the persons having no other supply than that from the ditches, were able to beg water occasionally from their neighbours, otherwise the mortality amongst these people would probably have been still higher. In the recent epidemic, since the ditches were filled up, the mortality in the immediate neighbourhood has been only the same as that in the rest of the sub-district of St. James's, Bermondsey. The proportionate reduction of the mortality being entirely due, as the above facts prove, to the circumstance that none of the people drank worse water than those in the rest of the district. The whole of Bermondsey suffered a higher rate of mortality in 1854 than in 1849. This is the case with nearly all the other districts and sub-districts supplied exclusively by the Southwark and Vauxhall Water Company, and arises from the circumstance that, between 1849 and 1854, a great number of cesspools were suppressed, and water-closets substituted in their stead, throughout London, with the effect, when cholera was re-introduced, of sending the evacuations of the patients more generally and more quickly into the river.
Dr. Sutherland states that, "After the decline of the cholera, the President of the General Board of Health directed Dr. Fraser to make an inspection and inquiry into the condition of Lambeth-square, to ascertain to what extent the epidemic had prevailed among the population. This inquiry was directed in consequence of certain improvements in drainage having been carried out, subsequent to the epidemic of l849."--p. 67.
Dr. Fraser seems to have carried out his inquiry very ably and faithfully according to his instructions, which unfortunately contained no intimation that the supply of water had been altered in any part of Lambeth, and he appears not to have been himself aware of the circumstance, or he would have alluded to it. Lambeth-square contains 35 eight-roomed houses, inhabited by the better class of artisans. There were six deaths from cholera in 1849. In 1852 water-closets were substituted for open privies, and improvements were made in the drainage, and last year there was no death from cholera. The general mortality has also been lower the last two years than during the two years previous to the alterations. An improvement took place in 1852, however, of which Dr. Fraser was not aware. Lambeth-square is the property of one person, and is entirely supplied with water by the Lambeth Water Company, who in that year removed their source of supply from the middle of the sewers of London to Thames Ditton, as was before explained. To show that this was the real cause of the late immunity from cholera, I shall allude to another property, which has all the advantages described by Dr. Fraser as belonging to Lambeth-square, and the additional one of not being surrounded with the offensive smells external to the property, of which the inhabitants of that square still complain; but which has a water supply very similar to that which Lambeth-square had in 1849, namely, the supply of the Southwark and Vauxhall Company. In the Weekly Return of Deaths for September 9, 1854, the Registrar of the Clapham district writes as follows:--
"In consequence of there being a larger number of deaths from cholera this week in the vicinity of Park-road than in any other part of my district, I have inspected Park-crescent and Crescent-road, and found the drainage very good; the houses have recently been built, and there is great credit due to the landlords for the care they have taken to render them in every way comfortable and healthy; there is a water-closet and water laid on to each of them; but when I examined the water I found it in such a filthy state that I advised the inhabitants not to drink any more of it for the present. At most of the houses they had pieces of flannel, two or three thick, to act as filters."
There were only 472 deaths last year in all the 26,107 houses supplied by the Lambeth Water Company, or 1 death to each 56 houses, and therefore it is not surprising that a group of 35 should have escaped having a death.
Dr. Sutherland quotes some remarks respecting the water supplied to different parts of London, by Dr. Hassell, who very truly observes that the most impure is that of the Southwark and Vauxhall Company. He says: "Between it and the water of the Thames, as taken from the river at the spot at which the Southwark and Vauxhall Company obtains its supplies, there is frequently only that amount of difference which would arise from mere subsidence." Dr. Hassell describes the practice, which I have seen in hundreds of instances, of tying folds of flannel or other fabric over the taps through which the water of this company is distributed, and adds: "The quantity of dirt and organic matter obtained in this way in a short time is often perfectly surprising." Just after the above, on the same page (42), Dr. Sutherland quotes a passage from Dr. R. D. Thomson, who says that the water of the Chelsea Company is the most impure that is supplied in London, and that the water of the Southwark and Vauxhall Company comes next. The reader must not suppose, however, that the inhabitants of Belgrave-square and the great mansions round St. James's Park tie folds of flannel over the water taps, and collect a surprising quantity of dirt every time the water comes in, for this is certainly not the case. Dr. Thomson makes an unusual application of the word impurity, an application which would cause the water drunk at many of the fashionable watering places to rank as ten times more impure than that of an ordinary horse-pond. He includes every foreign ingredient in the water, in the term impurity, which may be allowable in a strictly chemical point of view, but practically pure water would, according to this view, be quite inadmissible in London, as it would dissolve the leaden cisterns and service-pipes, and poison the community.
The Chelsea Water Company obtain their supply from the same part of the river as the Southwark and Vauxhall Company, and their customers suffered a higher mortality from cholera in the late epidemic, than those of any other London water company, except the Southwark and Vauxhall. Between the mortality of the population supplied by these two companies, there was, however, a considerable difference. That of the population supplied by the Southwark and Vauxhall Company was 157 in each 10,000 inhabitants, that of the population an p plied by the Chelsea Company was 56, and that of the rest of London was 34 to each 10,000 inhabitants. The reason of the lower mortality in the districts supplied by the Chelsea Company than in those supplied by the Southwark and Vauxhall Company, can be very satisfactorily explained. While the latter company distribute the water nearly as they [86/87] take it from the Thames, the Chelsea Company have very large and expensive filtering beds, by which nearly all the visible dirt is separated from the water. The cholera poison may, much of it, be separated at the same time, but I have several reasons for concluding that the detention of the water reservoirs, which necessarily accompanies the filtration, is more effectual in diminishing the cholera poison than the mere filtration itself.
Whilst the Chelsea Water Company were detaining their water in large open reservoirs, during the hot dry weather of last summer, in order to separate from it as much as possible of what comes down the sewers, it was evaporating, and the relative quantity of sea salt, and of the salts belonging to the water of the river, were necessarily increased; in this way, Dr. Thomson, according to his method of investigating impurity, was able to pronounce this water more impure than that of the Southwark and Vauxhall Company.
Dr. Sutherland quotes a passage from Dr. Thomson, which seems to throw a very unmerited blame on the water of the New River Company. It is as follows:--"In the Soho district a very remarkable circumstance occurred in the houses supplied by the New River Company. In these it was found that the water, although taken on the same day, possessed a totally different composition from that contained in the reservoir at the New River Head; for, while the impurity of the reservoir water was 17.18 degrees, that of the Soho district, obtained from the New River Company, as ascertained by the water receipts, but from what source is unknown, was 30 degrees; the organic impurity being l.5l degrees in the first case, and 2 degrees in the second instance." P. 46.
Now, passing over the fact that the outbreak of cholera in this neighbourhood was confined, almost altogether, to persons who had water from a pump in Broad-street, Golden-square, and that those persons who confined themselves to the use of cistern water remained as free from cholera, throughout the outbreak, as persons in another part of London; there are two circumstances which ought at once to have shown Dr. Thomson that the water in these cisterns could have had nothing to do with the outbreak of cholera. The locality of this outbreak is extremely well defined. It is about a quarter of a mile in diameter, and includes a portion of the Golden-square sub-district, a portion of the Berwick-street sub-district, and a small part, only fifty yards wide, of the adjoining sub-district of St. Ann's, Soho. The outbreak commenced in all parts of the locality on the same day, and, as nearly as can be ascertained, at the same hour. But the New River water extends to only about one half of the locality attacked. It supplies the sub-districts of St. Ann's Soho and Berwick-street, but does not extend into the sub-district of Golden-square, which is entirely supplied with the water of the Grand Junction Company. The districts of these companies have been long fixed, as firmly as the parish boundaries, and there was small reason for the inspectors of the Board of Health to examine the receipts. But, even if the New River Company had supplied all the locality of the outbreak, there is another circumstance which might have shown Dr. Thomson that this water could have no connexion with it. It would be impossible that the company's pipe, after proceeding a certain distance down Wardour-street, should suddenly take up a certain quantity of additional foreign matter or impurity; and that, after proceeding some way, it should as suddenly leave off this foreign matter again, just where the cholera ceased, and that these two processes should take place in nearly all the streets of the locality. A little inquiry also would have shown Dr. Thomson that the kind of water he speaks of extended far beyond the limits of the outbreak. The reason of its differing from that at the New River Head admits of a very easy explanation, but I am treating of cholera, and not of water supply.
Mr. Glover, in his Report on the Common and Model Lodging Houses, recently published, in speaking of the Soho Chambers, 36, Old Compton Street, makes the following remark:--"In the district of Golden-square (in which these chambers are situated), up to October 7th, no less than 267 persons died from cholera alone, exclusive of the mortality from diarrhœa; and yet in these chambers there was not a single case of cholera, and only seven of diarrhœa, none of which proved fatal.* (*Page 27.) Mr. Glover moreover enumerates Compton-street among those in which "the inhabitants were a dying in large numbers daily. "Now, in the first place, Old Compton-street, in which the Soho Chambers are situated, is not in the district of Golden-square, but in the next district but one to it; namely, in the district of St Ann's Soho, the district of Berwick-street lying between the two. In the next place, and what is of still more importance, so far from Compton-street being one of the streets in which the inhabitants were dying in large numbers daily, there was not a single death from cholera in this street, either during the outbreak or for three weeks before or after it. The outbreak extended to a small part of the parish of St. Ann's, Soho, but not into Compton-street, than which there was not a street more free from cholera in London. It is a street containing 53 large houses, nearly all of them divided into tenements, and densely inhabited. The population of this street is probably not less than a thousand persons, and yet not a death from cholera was registered from it, from August 19th to September 30th, inclusive.
Mr. Glover makes it appear that the mortality of cholera in the common and model lodging-houses, during the late epidemic, was only at the rate of 7 to 10,000 inhabitants, whilst in the metropolis generally the mortality was 44 to 10,000. It is but justice to Mr. Glover to state that he makes the following remarks:--"This result is of so startling a character, that some doubts naturally arise as to whether the police return can be taken as actually correct, or merely as an approximation to the actual amount of mortality. It is very probable that many cases originated in the houses which ended fatally elsewhere."--P. 10.
The following circumstances, with which I became acquainted in making an inquiry for a different purpose, prove that Mr. Glover's surmise is correct. During the first seven weeks of the late epidemic there were only six deaths from cholera registered from the common lodging-houses in the parish of St. George, Southwark; but during this period there were seven deaths in the workhouse of persons who were admitted from the common lodging-houses, after being attacked with cholera. In fact, out of thirteen persons admitted into the workhouse, during these seven weeks, with fatal attacks of cholera, seven of them came from the common lodging-houses, as I have stated, and only six from all the other places, including two whose address was unknown, and who might also have been persons who generally lived in these lodging-houses. It is very probable, therefore, that if Mr. Glover had searched the books of all the workhouses and hospitals in London he would have been able to get a much nearer approximation to the real number of fatal attacks of cholera occurring in the common and model lodging-houses than he has done.
Except the distribution of the cholera poison in the water, there is no circumstance which favours its propagation so much as the crowding together of people of uncleanly habits; it is, therefore, very probable that the regulation of the common lodging-houses, and especially the establishment of model ones, has contributed greatly to the mitigation of the recent epidemics; but it is not likely that the inmates of the lodging-houses have enjoyed an immunity from cholera so much exceeding that of the inhabitants of May Fair as was indicated in Mr. Glover's report. As for the entire escape of model lodging-houses whilst the cholera was raging around, which has been so much commented on in the public prints, it did not exist at all. The idea arose out of the error respecting the Soho Chambers, which I have pointed out above.
The only other subject to which I shall allude in connexion with the recent Reports of the Board of Health, is the statement, several times repeated, and implied almost everywhere, that the cholera has been most severe where the air was most impure. That there is an occasional association between cholera and impure air, is what might be expected, according to any view of the pathology of cholera, but that this amounts to anything like a rule, a very few examples, drawn from the last epidemic in London, will serve to prove to every one acquainted with this metropolis. The sub-district of Saffron-hill, with the open Fleet Ditch steaming through it has experienced a lower mortality from cholera in the recent epidemic than any other sub-district in London, except the neighbouring one of St. George the Martyr, Holborn. Saffron-hill had a mortality of 5, and St. George of 4, in 10,000. No one acquainted with the south districts of London would assert that the air at Clapham and Kennington is as impure as in the low-lying districts of Lambeth, crowded with a poor [87/88] population, and containing the bone-boilers, and other offensive trades; yet the following figures, from the reports of the Registrar-General, show how these respective sub-districts were visited by cholera. I have added the London-road sub-district of Southwark, as it contains a very poor population in very dirty streets, and is on a level with Trinity high-water mark.
The reason of the lower mortality in the last four sub-districts, is that they receive a good deal of the new water supply of the Lambeth Company, while Clapham and Kennington 1st Part are chiefly supplied by the Southwark and Vauxhall Company, where the people have not pump-wells. In Kennington 2nd Part the water of the two companies is pretty equally distributed.
Cholera, as I stated before, spreads more readily from person to person in the crowded dwellings of the poor than under other circumstances. Even when the malady is propagated through the water supply, it causes a higher mortality among the poor than among the well-to-do, because, in addition to the cases caused directly by the water, others arise from the disease passing from one member of a family to another. But the poor very generally live in places where the air is impure, therefore, a certain amount of association between cholera and impurity of the air might be expected. A far greater association of this kind than actually exists, would, however, be no proof of any connexion in cause and effect. If an inquiry were set on foot with regard to the itch in London, and other towns, it would be rarely met with except in situations where the air is impure; a far greater association would be found between impure air and itch, than between impure air and cholera, and yet we know that impure air has no share in causing the itch.
Sackville-street.
Return to John Snow Publications
96."On the employment of chloroform in surgical operations"
Source: Snow, John. Lancet 2, 20 October 1855, pp. 361-63, Part 1.
Part 1
By John Snow, M.D.
I have now been very much occupied in the administration of chloroform for a period of nearly eight years; and I am quite confirmed in the opinion which I long ago expressed, that this agent may be exhibited with propriety in every case in which the patient requires, and is in a condition to undergo, a surgical operation. If it were simply a question of giving chloroform or not giving it, there are, indeed, some patients to whom one would prefer not to give it; but the question lies between exhibiting chloroform or inflicting the pain of an operation, and, according to my observation, the former is always the lesser evil of the two. The affection which is generally thought to be most opposed to the inhalation of chloroform is fatty degeneration of the heart; but from all that I have been able to observe, it is of great advantage, in such cases, to prevent the pain of an operation.
Patients with fatty degeneration of the heart are liable to die suddenly in two distinct ways: first, with the cavities of the heart empty; and, secondly, with the cavities of the heart full of blood. In the latter case, death is caused by the inability of the weakened heart to propel the blood; but, in the former case, where the patient dies by ordinary syncope, such as that occasioned by loss of blood, and where the cavities of the heart are empty, death must be caused by some undescribed condition which accompanies the disease of the heart, and not by that disease itself; for the most healthy heart would be unable to maintain the circulation when the blood no longer reached its cavities from the veins.
The pain of a surgical operation has a tendency to produce both those conditions of the cavities of the heart which are liable to prove fatal, when that organ is affected with fatty degeneration; whilst, on the other hand, chloroform has the effect of keeping the circulation in a more equable state. The ordinary kind of syncope, in which all the cavities of the heart are probably empty, was very common during surgical operations, before the introduction of ether and chloroform, even when the patients were apparently strong, and the operation of a trifling nature. Under the influence of chloroform, however, syncope is extremely rare, even in operations attended with considerable loss of blood. The pain of an operation has a tendency also, in many cases, to cause over-distention of the right cavities of the heart, owing to the patient straining violently, and holding his breath. The following instance, in which I had an opportunity of witnessing a similar operation, in the same patient, both with and without chloroform, shows this effect of pain, and the favourable effect of anæsthesia, in a remarkable manner.
On January the 6th, 1855, Mr. Fergusson performed lithotrity in King's College Hospital, on a man aged fifty-one. He generally directs chloroform to be administered in lithotrity, but in this instance he omitted to do so, as he thought that the bladder was not very irritable, and that the patient would not suffer much. I began to feel the pulse just when the patient saw the lithotrite about to be introduced. It was 120 in the minute. As soon as the instrument was introduced, the pulse increase to 144, and immediately afterwards it became uneven, irregular, and intermitting. I could not count more than three or four beats at a time, and, occasionally, when the pain seemed greatest, and the man was straining and holding his breath, the pulse at the wrist was altogether absent for four or five seconds at a time. In order to ascertain whether the absence of pulse might not depend on the pressure of the muscles of the arm, caused by grasping the table, I applied my ear to the chest, and found that there was no sound whatever to be heard during the intervals when the pulse was imperceptible. It was evident that the patient held his breath till the right cavities of the heart became so distended as to stop the action of that organ till the respiration returned. The man did not complain, or cry out, during the operation. A week afterwards the lithotrity was repeated, but on this occasion I administered chloroform. The pulse was about 120 in the minute, when the patient began to inhale; but it became slower as he was made unconscious, and it was regular and natural during the operation. It was only towards the end of the operation, when the effect of the chloroform was allowed to diminish, and the man began to strain a little, though not yet conscious, that the pulse intermitted slightly, passing over a single beat occasionally. There were none of the long intermissions of the pulse which were observed on the former occasion.
It is very evident, that if this patient had been the subject of any affection of the heart which weakened or embarrassed its action, he would have run a much greater risk from the pain of the first operation than from the inhalation of chloroform in the second one.
I have given chloroform with a favourable result to a great number of patients having all the symptoms of fatty degeneration of the heart, as a weak, intermittent pulse, arcus senilis of the cornea, and liability to faintness. The only patient, indeed, whom I have had the misfortune to lose whilst inhaling chloroform had very extensive fatty degeneration of the heart, the symptoms of which were well marked during life; but I am by no means sure that this patient died from the effects of chloroform, although I thought it best at the time to designate the death as one from this agent. The patient, a gentleman aged seventy-three, died just as he probably would have done, at no distant day, if no surgical or medical interference had taken place. He was making a straining effort, as if he was beginning to feel the pain of the operation, and I was commencing to give him a little more chloroform, when he suddenly expired; and I am quite unable to tell whether it was the effort of straining, or the influence of the chloroform, which caused death to take place at the moment when it did. The quantity of chloroform he was taking at the time was very small indeed, and largely diluted with air, and he had inhaled it several times before. But if it be granted that this death was caused by the chloroform, when I take into account the number of other patients with similar symptoms, to whom I have given it with a favourable result, I do not consider that it furnishes any argument against the use of this agent in such cases. Patients with fatty degeneration of the heart in an advanced stage are, no doubt, very undesirable subjects for a surgical operation under any circumstances; but when it is absolutely necessary to perform one, I am of opinion, both from what I have seen of the effects of pain on the circulation, and from what I have seen of the effects of chloroform in patients of this kind, that it is desirable to let them have the advantage of its administration. Patients with symptoms of fatty disease of the heart sometimes become faint after the conclusion of an operation under chloroform if they are kept in a sitting posture, but I have always found the faintness to subside on placing them horizontally.
Out of the entire number of deaths from chloroform which are recorded, there are very few in which any considerable disease of the heart was found. In fact, the majority of those who are dead from chloroform were healthy persons in the best period of life--that is, from fifteen to thirty-five or forty, and it is most likely that they had, on the average, a sounder state of the heart than the multitude who have inhaled chloroform with impunity. It was not very uncommon occurrence for patients to die on the operating table before the introduction of anæsthesia, either just before the commencement of an operation or during its performance. Dr. Simpson, writing in 1852, says that two deaths had occurred on the operating-table in Edinburgh since the discovery of the effects of chloroform, in cases where the agent was not used. One died directly after the first incision through the skin, in a case of hernia, and the other instantly after the use of an abscess lancet. He also alludes to a case which occurred in Edinburgh just before the introduction of chloroform. Dr. Robertson had shaved the groin of a patient, and was proceeding to perform the operation for hernia, when the patient fainted, and died before any incision was made.
We have no information respecting the state of the heart in the patients who died suddenly on the operating table before the introduction of ether and chloroform, but it is extremely probably that many of them were affected with fatty degeneration of this organ; and I believe that by the careful administration of chloroform during operations on such patients, we not only prevent pain, but may in some cases save life.
The sudden deaths which occasionally took place on the operating table, before the introduction of anæsthesia, have sometimes been alluded to as affording an explanation of the deaths that have occurred during the use of chloroform; but, with a very few exceptions, this is not a correct view of the subject. In the instance at Mr. Robinson's, and in that at St. George's Hospital, the patients appeared to die suddenly from mental emotion, without being affected by the chloroform, which they were only just beginning to inhale; and in three cases on the Continent, where the patients died suddenly, just after great operations, loss of blood was probably the cause of death. With these, and perhaps one or two other exceptions, the deaths that have taken place under the influence of chloroform have nothing in common with those which happened on the operating-table before its introduction. In these latter cases, if the death did not arise from hæmorrhage, it was occasioned either by pain or mental emotion; but as the patient neither feels nor thinks when fully under the influence of chloroform, he cannot die from either of the two latter causes. In speaking of the benefits of chloroform, it is quite allowable to bring forward the sudden deaths which occasionally happened in operations, as a set-off against the deaths from this agent; but to suppose that the patients who have died during the employment of chloroform are the same that would have died without it is undoubtedly a mistake. The late Dr. Richard Mackenzie related a case of sudden death, which, he said, narrowly escaped being imputed to chloroform. He reduced a fracture of the radius, about an inch above the wrist, in a case where there was a good deal of swelling and displacement. He would have used chloroform, but he had none with him. Within five minutes after Dr. Mackenzie left the house, the patient died instantaneously, whilst he was talking freely to those about him. He was a corpulent man, from sixty-five to seventy years of age, who had lived freely, and Dr. Mackenzie thought it probable that he had fatty degeneration of the heart, but there was no examination of the body. The cause of death, in this case, was probably the pain to which the patient had been subjected, and it is not unlikely that the employment of chloroform might have saved his life for a time. At all events, there is no reason to conclude that the patient would have died in the manner he did if chloroform had been administered.
Surgical operations are, I believe, never performed during acute disease of the lungs, and chronic affections of these organs, as phthisis and chronic bronchitis, form no objection to its use. I have administered this agent in a number of operations where one or other of these diseases was present, and there have been no ill consequences in any case. The mucous membrane of the air-passages is always irritable, both in consumption and bronchitis, and the chloroform is apt to excite coughing at first. It is therefore necessary to begin by giving the vapour very gently in these cases, and in a little time the irritability of the mucous membrane is allayed, and insensibility can always be induced in a few minutes. The cough is afterwards relieved, in nearly all these cases, for a time--often for two or three days, in cases of chronic bronchitis.
Affections of the head offer no obstacle to the exhibition of chloroform in surgical operations. I have given it in many cases where more or less paralysis remained, from previous attacks of apoplexy, and no ill effects have followed. In a patient on whom Mr. Robert Wade lately operated--removing a scirrhous tumour of the labium pudenda--there was probably disease of the heart, as well as the remains of an apoplectic clot in the brain. The age of the patient is seventy-two; she is partially hemiplegic, from an apoplectic seizure two years ago; and her pulse, when I saw her, was irregular in the strength of its beats, and also intermitted. She went through the operation very well, and readily recovered her consciousness. I saw Mr. Wade eleven days after the operation, and learned that his patient was going on well. There is often some trouble in giving chloroform to insane patients, for when they cannot be persuaded to inhale it, it has to be given by force. When once they are under its influence, however, the surgeon is enabled to make examinations, and to perform operations that would otherwise be impossible.
I have given chloroform to a number of patients who were reduced to a state of extreme debility, from chronic disease of the large joints, and from various other causes. Chloroform agrees extremely well with such patients; they do not require to inhale so much as stronger persons, but that forms no difficulty, as the administration of this agent does not consist in giving a dose, but in executing a process, and the effects produced are observed as the process goes on.
An objection was raised in the Crimea last autumn to the use of chloroform in operations immediately succeeding to severe gun-shot wounds; but this objection seems to have given way before further experience. According to the letter of a medical officer, quoted in the medical journals, this agent was used with very good effect in such cases in particular where the soldier had the left thigh shattered to pieces, the right hand and wrist joint in the same condition, and a compound fracture of the other arm. Amputation of the thigh and forearm was performed, and, when sent to Sentari, two days afterwards, the patient promised to do well. The writer was of opinion that the soldier could hardly have borne the shock of his wounds and the operation without chloroform. I have not had occasion to give chloroform in operations immediately after gun-shot wounds, but after severe compound fractures from other causes, I have found its action very satisfactory, as well as in strangulated hernia, where there was excessive exhaustion.
I have often administered chloroform during pregnancy and no ill effects have followed in any case. Mr. Fergusson, Mr. Bowman, Mr. Henry Charles Johnson, and Mr. B. Travers, jun., are some of the surgeons for whom I have given chloroform to patients undergoing operation during pregnancy.
Chloroform may be given with propriety to patients of all ages. I have exhibited it to several infants aged from ten days to three weeks, and to one patient nearly ninety. I have notes of the cases of 145 infants under a year old, to whom I have administered this agent. A great number of them were operated on for hare-lip by Mr. Fergusson, who performs this operation at the earliest period of life, if the children are healthy. Chloroform acts very favourably on infants and children. There has, I believe, been no death from chloroform under the age of fifteen years. Chloroform was, indeed, blamed for the death of a child, in Germany, during the removal of a very large nævus on the side of the face, but there is no doubt that the cause of death in that case was hæmorrhage.
The only direction which it is usually requisite to give beforehand to the patient who is to inhale chloroform, is to avoid taking a meal previous to the inhalation; for chloroform is very apt to cause vomiting if inhaled when there is much food in the stomach. The sickness is not attended with any danger, but it constitutes an unpleasantness and inconvenience which it is desirable to avoid. The best time of all for an operation under chloroform is before breakfast; but the customs and arrangements of this country do not often admit of that time being chosen, and it is not advisable to make the patient fast beyond his usual hour. It answers very well to perform an operation about the time when the patient would be ready for another meal, or, if the time of the operation fall two or three hours after the usual time of eating, to request the patient to make only a slender repast at that time, so as just to prevent this feeling of hunger. It is impossible to prevent vomiting, in some cases, with best precautions, for the stomach occasionally will not digest when the patient is expecting a surgical operation, and the breakfast may be rejected in an unaltered state hours after it has been taken. In other cases the patient does not vomit, even when he inhales chloroform shortly after a full meal.
The most convenient position in which the patient can be placed whilst inhaling chloroform, is lying on the back or side, as he is then duly supported in the state of insensibility, and can be more easily restrained if he should struggle whilst becoming insensible. The semi-recumbent posture on a sofa, also, does very well; and there is no objection to the sitting posture, when that is most convenient to the operator. In that case, however, the patient could be placed in a large easy chair with a high back, so that the head as well as the trunk may be supported without any effort, otherwise he would have a tendency to slide and fall when insensible. It has been said, that it is unsafe to give chloroform in the sitting posture, on the supposition that it would, in some cases, so weaken the power of the heart as to render it unable to send the blood to the brain. Observation has proved, however, that chloroform usually increases the force of the circulation; and although the horizontal position is certainly the best for a patient under an operation in all circumstances, I consider that the sitting posture is by no means a source of danger when chloroform is given, if the ordinary precaution be used which would be used without chloroform, that of placing the patient horizontally if symptoms of faintness come on. I have preserved notes of 647 cases in which I have given chloroform to patients sitting in a chair, and no ill effects have arisen in any of these cases.
The person who is about to inhale chloroform is occasionally in a state of alarm, either about the agent itself or the operation which calls for its use. It is desirable to allay the patient's fears if possible before he begins to inhale, as he will then be able to breathe in a more regular and tranquil manner. In a few cases, however, the apprehensions of the patient cannot be removed, and they subside only as he becomes unconscious from the inhalation. It has been said that chloroform ought not to be administered if the patient is very much afraid, on the supposition that fear makes the chloroform dangerous. This is, however, a mistake; the danger, if any, lies in the fear itself. Two cases were alluded to above, in which the patients died suddenly from fear, whilst they were beginning to inhale chloroform, and before they were affected by it; but the probability is, that if they had lived till the chloroform took effect, they would have been as safe as other patients who have inhaled it. If chloroform were denied to the patients who are much afraid, the nervous and feeble, who most require it, would often be deprived of its benefits. Moreover, the patients would either be prevented altogether from having the advantage of surgery, or they would be subjected to the still greater fear of the pain, as well as the pain itself; for whatever undefined and unreasoning fears a patient may have when the moment comes for inhaling chloroform, he has only chosen to inhale it on account of a still greater fear of pain. The practice I have always followed has been to try to calm the patient by the assurance that there was nothing to apprehend from the chloroform, and that it would be sure to prevent all pain; but where it has been impossible to remove the fears of the patient in this way, I have always proceeded to remove them by causing a state of unconsciousness. As soon as this is induced, the pulse, which just before may have been extremely frequent and small, from the effects of fear, generally falls almost to its natural frequency, and resumes its full volume and force.
As a general rule, it is best to place the patient in the position in which the operation will be performed before he inhales the chloroform; but in cases of disease of the large joints, and other instances where motion causes pain, it is an advantage to give the chloroform to the patient in bed before he is removed to the operating-table. It is often desirable also to give it to children in another room, that they may not see any of the preparations for the operation.
[Part 2 appeared in the following issue.]
Return to John Snow Publications
97."On the employment of chloroform in surgical operations"
Source: Snow, John. Lancet 2, 27 October 1855, pp. 383-85, Part 2.
Part 2
By John Snow, M.D.
It is unnecessary to say anything on the propriety and advantage of administering chloroform in lithotomy, in the larger amputations, and the removal of tumours of the breast, for I believe the whole of the profession agree on this point. There is still, however, some difference of opinion as to the propriety of giving it in lithotrity. It has been said that the surgeon requires the assistance of the patient's sensations, to prevent him from seizing the coats of the bladder in the lithotrite; but if this were the case, I believe that the operation could never have been performed at all. Some patients cry out when they are scarcely touched, whilst others will bear the greatest torture without a murmur. I believe there is very little danger, or even possibility of seizing the bladder with the lithotrite, and that, even if this should take place, the surgeon's sense of touch would be the proper guide to prevent mischief. The greatest sensibility of the bladder appears to be at the neck and it may fairly be doubted whether seizing the mucous membrane of the cavity would cause much pain. It has always appeared to me that the operation of lithotrity is one in which chloroform prevents very great suffering, and is of the utmost advantage. I will, however, quote the opinion of one who has had much practice in lithotrity both before the introduction of anæsthetic surgery and since, and is therefore better able to judge. Mr. Fergusson says, in his Practical Surgery,* "I am of opinion that there is not any department in practical surgery in which anæsthesia has been of more service than in this. Since the earliest period of its introduction I have almost invariably used it on such occasions, and with the best possible effects; and now I no more think of performing the operation of lithotrity without this agent than I would that of lithotomy." (*Third edition, p. 800.) Many other surgeons are of the same opinion as Mr. Fergusson, and some of those who are disinclined to use it as a general rule, practically admit its benefits by resorting to its employment in cases where the urinary passages are very irritable, or the patient very intolerant of pain. The operation of lithotrity requires a pretty full dose of chloroform, as, without this, the patient is apt to strain very much and move his legs about.
Some surgeons, and more especially those of Edinburgh, had an objection, at one time, to employ chloroform in large operations about the mouth and nose, and especially in the removal of tumours of the jaw, for fear the blood should flow into the windpipe during the state of insensibility and cause suffocation. However, I have given chloroform in a great number of such cases without any ill effects. Unless the effects of the chloroform are too deep or long-continued, the sensibility of the glottis is not impaired; if a little blood enters the windpipe, it is coughed out again; the patient can hold a little blood in his throat, and breathe through it with a gurgling noise, just as he would in the waking state; and if the quantity of blood begins to embarrass the breathing, the head must be leaned forward to get rid of it, and the same attention paid to the patient which would be paid if chloroform were not used. After the commencement of an operation of this kind, a little chloroform may be given from time to time, on a sponge, as opportunity permits, so as to keep up the insensibility to some extent. I prefer, under these circumstances, to have the chloroform diluted with spirit, in the manner and for the reason that I shall mention further on, in treating of its use on a handkerchief.
A case has been related by Mr. Prescott Hewett, in the Medico-Chirurgical Transactions, (vol. xxxiv., p. 43.) in which a patient died about half an hour after the removal of the greater portion of a tumour of the upper jaw. He was previously much reduced by hæmorrhage from the tumour, and he fainted before the operation was concluded. He remained much exhausted till the period of his death, though quite conscious. The breathing was not embarrassed until he was moribund, at which time a little blood, which was still oozing from the remains of the tumour was drawn into the trachea, as I was informed by a surgeon who was standing by at the time. This circumstance gave rise to some small spots of ecchymosis, which were found in the lungs after death. It was suggested that in this case blood might have got into the lungs during the insensibility from chloroform, and so have been the cause of death. But, in the first place, the symptoms which were observed during the operation, and for some time afterwards, were simply those of syncope, and not of embarrassed breathing; and, again, the amount of blood met with in the lungs was not enough to cause death, or even acute symptoms of any kind.
Extraction of cataract is an operation in which surgeons hesitated for a long time before employing chloroform. They were afraid lest the vomiting which sometimes attends or follows the use of this agent might be injurious to the eye. Mr. George Pollock and Mr. White Cooper were, I believe, the first surgeons who adopted the use of chloroform in the extraction of cataract; and I have since administered this agent also in many operations of this kind for Mr. Lawrence, Mr. Bowman, Mr. Haynes Walton, and others. Several of the patients were considerably over eighty years of age. By taking care not to give the chloroform too soon after a meal, there has very seldom been vomiting; and although a little vomiting has taken place in a very few of the cases, it was not attended by straining, and, as I understand, did not do harm in any case. I have, indeed, been informed of a case, at which I was not present, where chloroform was given, and where the patient vomited and expelled the humours of the eye; but she was a person of bad constitution, and such accidents did occasionally happen before the use of chloroform. In some cases, where the patient is very nervous, and the eye very irritable, I believe that chloroform is essential to the success of the operation, but it is not necessary to use it in all cases. I understand from Mr. Bowman that his practice is to operate without chloroform in cases where the patient does not wish for it, and has resolution to lie still, and keep the eye steady. The operation is said to be not very painful, but it is one which has a great tendency to rouse the patient, if he is not very insensible; it is necessary therefore to induce complete insensibility, and to keep it up till the lens is extracted, as the least movement of the patient might be prejudicial.
Operations about the anus generally require a full dose of chloroform, as the part is very sensitive when in a state of disease, and the patient, if not quite insensible, has a tendency to move his legs, which is very embarrassing to the surgeon, especially if there is no one to hold them. It was feared at one time that there would be a difficulty in operating for hæmorrhoids under chloroform, as the patient is often required to press them down; but it is found that if he do so beforehand, and whilst he is beginning to inhale, the bowel remains down; in fact, there is a great tendency to make a straining effort under the influence of chloroform, when the rectum is the seat of operation. Mr. Salmon thinks that the vessels of the rectum bleed rather more during operations under chloroform than without it, owing to the relaxation or diminished contraction of the sphincter; but I have not heard other surgeons make the same remark.
With respect to the deaths which unfortunately take place, now and then, from chloroform, many medical men have supposed that they are to be avoided by carefully selecting the cases for its administration; and declining to give it in certain affections, especially of the heart; whilst others, remarking that the deaths have often occurred in persons apparently the most healthy, acknowledge that they are not to be avoided by selecting the patients, but consider that they nevertheless depend on some peculiarity in the constitution which is not to be discovered beforehand. This is a more melancholy conclusion than the former, as it invests the chloroform with some amount of danger in all cases. It meets with apparent support at first sight, however, in the circumstance that some patients have died from a very small quantity of chloroform, whilst in numerous instances a large quantity has been used without ill effects. A little further inquiry shows, however, that several of the patients who died from chloroform had inhaled it previously in as great quantity without ill effects; and in the case of Samuel Bennett, which occurred in Westminster, in February, 1849, half an ounce of chloroform was used without causing insensibility, and when a fresh supply was obtained and administered, two hours afterwards, he suddenly expired. But it cannot be supposed that a person would have a peculiarity of constitution at one time which he did not possess at another, especially within the space of two hours.
In two papers which I had the honour to read to the Medical Society of London* a few years ago, it was shown that the deaths which had taken place from chloroform were occasioned by the sudden arrest of the action of the heart by this agent, and this is equally true of the deaths which have since occurred.
(*See Edin. Med. and Surg. Journal, No. 180, and London Journal of Medicine, 1852.)
To stop the action of the heart by the direct action of chloroform, there requires to be a larger proportion of it present in the blood than suffices to arrest the action of the muscles of respiration, and, therefore, if the vapour were always inhaled in a very regular and gradual manner, it would be impossible for it to paralyse the heart by its direct influence; for the breathing would first cease, and the action of the heart would only be brought to a close by the absence of the respiration, as in asphyxia. But as the heart is the first organ which the chloroform reaches after it is taken into the lungs, the coronary arteries being the first branches given off from the aorta, it is possible, if the vapour inhaled be too strong, that the heart may receive an overdose. When animals are made to breathe air containing four or five per cent of vapour of chloroform till death ensues, the breathing ceases first, and the heart continues to beat for a minute or two longer. During this interval life can easily be restored by means of artificial respiration, and the animals sometimes give one or two gasps at the moment when the heart is ceasing to beat, which may restore the action of that organ, and bring about recovery, if the animal have been removed from the chloroform. On the other hand, when animals are made to breathe air, containing eight or ten per cent of the vapour, death takes place suddenly, the motion of the heart ceasing at the same time as the breathing, or even before it. It requires a little contrivance to make the air on all occasions take up as much as eight or ten per cent of vapour of chloroform, and this explains not only how accidents may happen, but also why they happened so rarely, even when no regard is had to the amount of vapour in the air breathed by the patient. According to experiments, which I related on a former occasion, the amount of chloroform required to stop the action of the heart is one-eighteenth part as much as the blood will dissolve, or one part of chloroform to about 5,184 parts of serum of blood. The actual quantity of chloroform, therefore, which, by acting locally on the heart, arrests its motion, and causes a sudden accident, is very little more than a quarter of a minim. Consequently it need excite no surprise that the amount of chloroform which has been used in cases where accidents have occurred has been extremely variable. The danger from chloroform bears very little relation to the quantity used. In fact, to make an adult patient insensible with half a drachm is not so safe as to use a drachm in the process, if it be used judiciously; for in the former case the air must be more highly charged with vapour than in the latter. Exhalation of chloroform is always going on at the same time as inhalation, and to cause insensibility with vapour largely diluted, a larger quantity of it must be used than when it is less diluted.
I have already expressed the opinion that chloroform may be given to every patient requiring an operation without increasing the danger, whatever his condition may be; and have now to add, that the danger from chloroform, when it does exist, is as great to the strong and healthy as to the feeble and diseased. In fact, it is precisely in the most strong and robust persons that, according to my belief, the greatest care is required in giving chloroform. Robust lean persons, accustomed to hard work or athletic sports, require the narcotism of the nervous centres to be carried further than in the feeble, fat, or sedentary, before they will lie still under the use of the knife; and they are also very apt to struggle and become rigid after they are made unconscious, but before being insensible. During this state of struggling and rigidity they often hold the breath for a considerable time, and then suddenly draw a deep inspiration; and, if the vapour of chloroform is not presented in a very diluted form, a large quantity of it may be drawn into the lungs all at ounce, at a time when the pulmonary circulation is probably much retarded from the temporary suspension of respiration. In this way the portion of blood passing through the lungs at the moment may be so overcharged with chloroform as suddenly to paralyse the heart. In a considerable number of the fatal cases of inhalation of chloroform, the patient has expired suddenly whilst he was struggling in an involuntary manner.
The danger which exists in giving chloroform is simply that the patient should be allowed to breathe air too highly charged with vapour; for when the vapour is sufficiently diluted its effects takes place so gradually that no medical man can mistake them, and proceed to give an overdose. A very prevalent error respecting chloroform is to suppose that the patient is safe as long as he gets sufficient air for the purposes of respiration, whilst the truth is that the more air a person breathes the greater is his danger, if the air happens to be over highly charged with vapour. I have not space, in this paper, to enter on mode of operation of narcotic vapours, but, in order to show that narcotics, in a gaseous form, do not produce their effects by mechanically excluding the air, it is only necessary to allude to two or three well known agents of this class. Thus, whilst air containing eight per cent of vapour of chloroform cannot be inhaled without danger, air containing four or five times as much vapour of ether may be breathed with the utmost impunity. Nitrous oxide gas may be breathed when diluted only with the air which is present in the lungs at the beginning of the experiment; whilst the vapour of hydrocyanic acid requires to be diluted with several hundred times its volume of air before it can be inhaled without danger.
The means which I use to prevent the air breathed by the patient being too highly charged with vapour, is an inhaler which I have described on a former occasion. I cannot with a handkerchief regulate the amount of vapour and of air in the manner that is desirable; but I consider that those who prefer to give chloroform on a handkerchief may do so without danger though with no great accuracy, if they dilute the chloroform with rectified spirit. Either two parts by measure of spirit to one of chloroform, as recommended by Dr. Warren, of Boston in America, or equal parts of each, answer very well. Very little of the spirit is inhaled; it remains behind on the handkerchief, but it has the effect of lowering the elastic force of the vapour of chloroform, and thereby diminishing the amount of the vapour that the air will take up under the same physical circumstances.
In whatever way chloroform is given, it is necessary to begin gently at first, in order to accustom the mucous membrane of the air-passages to the pungency of the vapour, and to increase the strength of the vapour by degrees. I usually take two or three minutes in children and about four minutes in the adult to produce insensibility; but in robust, muscular subjects, who struggle much, it is sometimes desirable to proceed so cautiously as to take seven or eight minutes. In giving chloroform, it is best to observe every symptom exhibited by the patient; but the sensibility of the edge of the eyelid is the best test of the general sensibility. When the ciliary border may be touched without causing winking, or with very slight winking, the knife may in nearly all cases be used without causing a flinch or a cry. The state of the breathing is the best guide against carrying the effects of the chloroform too far. If it beings to [384/385] be stertorous, it is advisable to suspend the inhalation. The pulse is of less consequence than many of the other signs; for if the chloroform be properly diluted with air, it cannot seriously affect the pulse, and if it be not the pulse might cease suddenly. Its last beat in some of the accidents which have happened has been equal in strength to any which went before.
It is impossible in a brief space to allude to more than a few of the points connected with the use of chloroform in operations. I have therefore passed over most of those points on which I believe the profession are entirely agreed, and have treated chiefly on those respecting which I considered that my views might differ from those of, at all events, some of my professional brethren, in order that there might be the more room for the expression of opinion and experience.
Sackville-street, October, 1855.
Return to John Snow Publications
98."On the mode of communication of cholera"
Source: Snow, John. Edinburgh Medical Journal 1, January 1856, pp. 668-70, [Letter to Ed.].
To the Editor of the Edinburgh Medical Journal
Sir,--Dr. Alison has called attention in the last number of the Journal to the opinions and facts of Dr Budd of Bristol, respecting the communication of cholera by dejections, and I shall be obliged if you will allow me to make a few additional remarks on the subject, partly on my own account, but chiefly to lay the matter before the reader in what I conceive to be its true aspect. I arrived at the conclusion in the latter part of 1848, that cholera is communicated by the evacuations from the alimentary canal, and in August, 1849, I endeavoured to establish this point by a number of facts, which I published in a pamphlet, On the Mode of Communication of Cholera. In the following month, Dr William Budd published a pamphlet On Malignant Cholera in which he expressed views similar to my own, and made a full and handsome acknowledgment of my priority in more than one place in his essay. I feel sure that Dr Alison was not aware of these circumstances, or he would have mentioned my name in connection with his subject.
In his recent papers in the Association Journal, Dr William Budd attributes a much greater range to the action of the cholera poison through the air, than I am willing to admit, and if he can establish this point, the credit of it will be due to him. In my opinion, the cholera poison only produces its effects through the air when carried by insects, or when the evacuations become dry, and are wafted as a fine dust. I have on several occasions, since the autumn of 1849, alluded to the great mortality from cholera amongst the mining population of this country, as an instance in which the morbid matter of the disease is swallowed with the food. As the miners stay in the pits eight or ten hours at a time, they always take food down with them, which they invariably eat with unwashed hands, and without knife and fork. There are no privies in the pits, and Dr Budd himself alludes to the foul state of the latter. When a case of cholera or choleraic diarrhœa occurs in a pit, it must therefore almost of necessity happen that the hands of many of the workmen would be soiled by the evacuations, minute quantities of which would be swallowed with the food. Dr Budd has alluded to the food of the pitmen being supplied from very different sources, and prepared by different hands; but the hand by which the food is contaminated is as often that from which it is eaten, as that by which it is prepared. This mode of taking minute quantities of poison was pointed out by Dr. Christison long ago as being the way in which house painters of uncleanly habits, sometimes acquire lead colic.
In the very interesting cases which Dr Budd has related of propagation of cholera in the ill kept privies of a large workhouse, the same mode of communication of the disease could not fail to exist. The seats would be soiled by the cholera discharges, and the paupers who came afterwards would have neither the desire nor the opportunity to wash their hands after each visit to the place.
. . . . . . . . . . . . . . . . . . . . . . .
The mode of communication of the disease which I am advocating also, explains many circumstances in the history of cholera, which could not be explained by effluvia from the evacuations. I allude to the spreading of cholera in the crowded habitations of the poor, who cook, eat, and nurse the sick in the same room, and pay little attention to cleanliness, and to its not spreading in the houses of the well-to-do; also to the escape of the medical and clerical visitors, who do not eat or drink in the room of a poor cholera patient, and who carefully wash the hands when required, whilst the social visitor who comes to see the patient, or to attend his funeral, often suffers.
. . . . . . . . . . . . . . . . . . . . . .
Dr Budd entirely agrees with me that the cholera poison is produced only in the alimentary canal, and acts only on that canal, which it reaches by being swallowed. He enforces this point by the same arguments that I had used, adding indeed some additional illustrations; so that in fact there is no difference between us respecting the essential mode of communication of the disease, but only as to the extent to which it is communicated through the air.
. . . . . . . . . . . . . . . . . . . . . .
I would gladly say much more on the pathology of cholera as bearing on the mode of its communication, but I am afraid of making this letter too long. I will only say in conclusion that, should the views I first promulgated be exactly correct, the extension of cholera may be more easily prevented than it would be if the slight modification of these views introduced by Dr Budd were true. In [669/670] the former case all that would be required to prevent the disease would be such a close attention to cleanliness in cooking and eating, and to drainage and water supply, as is desirable at all times.--I am, Sir, your obedient servant.
John Snow, M.D.
18 Sackville Street, London, 14th Dec. 1855.
([Editorial comment:] We regret that from want of space, we have been compelled to abbreviate Dr. Snow's letter. The important points, however, have been retained. His theory that it is chiefly or almost exclusively by swallowing that the poison of cholera is taken in, can scarcely be supposed, notwithstanding his arguments, to be the usual mode of admission of the poison in the numerous cases which he, as well as Dr Budd, seems to suppose to have extended by the people using the same privies. Dr Alison, in former papers, in which he maintained the contagious property of cholera, has, however, expressly said that he gave no opinion as to the mode or modes in which the poison, thrown off by the human body, may be taken into another--only as to the question whether, in one way or another, it may be so thrown off and may be so taken in, and the epidemic extension be thus affected; and, therefore, if as Dr Alison believes, there are different modes of extension, multiplication and absorption of the poison, demanding a certain multiplicity and variety of practical precautions--this will be all in favour of the only practical opinion Dr Alison has given on the subject.)
Return to John Snow Publications
99. "Further remarks on the cause and prevention of death from chloroform"
Source: Snow, John. Lancet 1, 9 February 1856, pp. 148-50.
By John Snow, M.D.
I read two papers before the members of the Medical Society of London a few years ago,* on the Cause and Prevention of Death from Chloroform, in which I pointed out that when animals, such as cats, rabbits, and guineapigs, are made to breathe air containing four or five per cent of vapour of chloroform till they die, the breathing ceases a minute or two before the circulation of the blood; and that during this interval, in which the heart can be heard and felt to be still beating, the animal could be easily restored by artificial respiration; and, moreover, that at the moment when the heart's action was ceasing, the creature often gave one or more gasping inspirations, which, in many cases, had the effect of causing its recovery, if it had been removed from the chloroform. I showed that this mode of dying did not depend on a want of power in chloroform to arrest the functions of the heart by its direct effects, but on the circumstance that it requires rather more of this agent to stop the action of the heart than to arrest the respiratory movements. I had ascertained the power of chloroform to act directly on the heart by blowing the vapour on that organ when exposed, and by injecting a solution of it in water into the coronary arteries, as well as by giving it by inhalation. In some experiments on frogs, which go on absorbing vapour by the skin, after the respiratory movements have ceased, I was able also to ascertain the amount of chloroform which suffices to paralyse the heart, and I found it to be one-eighteenth part as much as the serum of the blood is capable of dissolving; whilst about one part in twenty-two of what the blood will dissolve has the effect of arresting the action of the muscles of respiration.
(*See Edinburgh Medical and Surgical Journal, 1849, No 180, and London Journal of Medicine, 1852.)
I pointed out also what I considered to be of the utmost importance in relation to the accidents from chloroform--viz., that this agent has the effect of arresting the action of the heart, by its direct influence, in animals of warm blood, when they breathe air containing not less than eight or ten per cent of the vapour. I had ascertained the circumstance in numerous experiments in which the stethoscope was applied to the chest of the animals whilst they were inhaling the chloroform, and also in two experiments, in which I was assisted by Mr. Peter Marshall, where, the animals being kept alive by artificial respiration after the heart was exposed, the chloroform was administered by a tube inserted in the trachea, and its instant effect on the heart could be seen.
The reason why the chloroform is thus able to act directly on the heart, under certain circumstances, is as follows:--When the vapour is breathed till such an effect is produced on the brain and nerves of respiration, that the action of the respiratory muscles is suspended, there is still vapour in the lungs, which has been inhaled during the last inspirations, and this continues to be absorbed into the blood which is passing through the lungs at the moment, increasing the quantity of chloroform which the blood already contains. Whether this additional quantity of chloroform, which is absorbed into the blood during the first few seconds after the breathing has ceased, shall be sufficient to remove the remaining sensibility of the cardiac nerves, and so paralyse the heart, depends on the quantity of vapour in the air last taken into the lungs. I find that when this quantity has not much exceeded five per cent, the action of the heart is not arrested by its direct influence, but when it reaches to about ten per cent, the action of the heart is at once arrested. I might explain the reason of this by arithmetical calculation, but shall content myself at present by stating the simple fact. In a few experiments, the action of the heart ceased a little before the breathing and I shall allude to them afterwards.
In the paper which I read in 1852, I expressed my conviction that no accident, of which the particulars had been related, had arisen from the medical man mistaking the symptoms, and continuing to exhibit too long the vapour of chloroform sufficiently diluted with air; but that in all the recorded cases the action of the heart, as well as the respiration, had been suddenly arrested by vapour not sufficiently diluted with air. An examination of the accidents from chloroform which have since been recorded, has satisfied me that they have also been occasioned in a similar manner.
Dr. Black, of St. Bartholmew's Hospital, who has had great experience in the administration of chloroform, has lately advanced the opinion, that in the accidents from chloroform the patients did not die from the pathological effects of this agent, but died simply of asphyxia before they were brought under the influence of the chloroform, owing to the respiratory movements having been arrested, or impeded, by the pungency of the vapour, which has been administered in too concentrated a form, at the beginning of the inhalation.
This view is, in my opinion, altogether untenable, as an explanation of the accidents from chloroform for various reasons. I find that when the access of air to the lungs is entirely cut off, death does not take place in less than three minutes and a half in guinea pigs, and four minutes in cats. In dogs, the process of asphyxia is still slower. Mr. Erichsen states, that on taking the average of nearly twenty experiments, the contractions of the ventricles continued for nine minutes and a quarter after the trachea had been closed, and that the pulsations of the femoral artery also were perceptible for an average period of seven minutes and a half after all access of air to the lungs had been prevented. The duration of life under privation of air, in the human subject, resembles its duration in dogs more nearly than in still smaller animals; and even if the pungency of the vapour of chloroform should entirely prevent the patient from breathing, and the medical man could overlook the fact that respiration was not going on, it cannot be supposed that he would use the force, and have the perseverance, to cause his patient to die slowly by asphyxia. With the breathing merely impeded, the process of dying would be still slower; but there has been no accident, during the exhibition of chloroform, in which death took place so slowly as to resemble that caused either by the complete or incomplete exclusion of air. If, therefore, any patient has died from the mere impediment to breathing, caused by the pungency of the vapour, it must have been in a case where there was a great tendency to sudden death.
An examination of the recorded cases of death from chloroform shows, indeed, that the patients did not die by impeded or interrupted respiration. To take, for example, the fatal case which occurred in the Royal Infirmary of Edinburgh. The patient breathed the chloroform from a handkerchief, which was held a little distance from the face, to allow the air to enter freely. An ounce of chloroform was expended in the process of inhalation. The man struggled considerably, from the effects of chloroform, as a certain class of patients do. The exhibition of the vapour was left off when the man began to snore, although he was still violent. He soon became quiet, however, and Dr. Dunsmure says, "I then shaved the perinæum, and was just going to make my first incision, when one of the assistants said that his pulse was becoming weak. The posterior tibial, Mr. Spence remarked, was good, but in a second or two after, both gentlemen exclaimed the pulse was gone." Dr. Dunsmure adds, "Those present who had an opportunity of observing the respiration positively assert that the breathing did not cease before the pulse." This patient certainly inhaled the chloroform, and became insensible from it, after which he died suddenly by cardiac syncope.
I may allude to another case which happened in St. Bartholomew's Hospital, whilst Dr. Black was present.
"A drachm of chloroform, by measure, was first poured on the sponge, but as the administration did not immediately commence, a considerable part of this was no doubt wasted. After a short inhalation, a second drachm was supplied, and subsequently the further quantity of half a drachm. The [148/149] patient had gone through the usual stages of excitement, etc., and the last dose was scarcely used as she sank off, almost immediately, after its application, into a state of complete insensibility, unattended with alarming symptoms. Almost five minutes had been occupied in the inhalation, and probably not more than a drachm and a half of the fluid really inhaled. The apparatus was now removed from the face, and the patient having been drawn into the proper position, Mr. Paget was about to commence the operation, when Dr. Black, who throughout had kept his finger on the pulse, noticed it to have become extremely feeble and fluttering. Almost immediately afterwards, the patient's countenance was observed to be dusky, turgid and congested, and the respiratory movements began to be performed at long intervals, and by slight catching efforts. . . . All efforts at respiration ceased about two minutes after the first indications of failure; the pulse [continued], however, as a very feeble flutter was felt occasionally, for at least two minutes later."
In this case, also, the patient breathed the chloroform, and became quite insensible from it, when the heart became suddenly paralysed, so far as to be unable to keep up the circulation.
Out of forty-four deaths from chloroform which are recorded, seven took place after the patient was quite insensible, and when the surgeon was just about to begin the operation; twelve occurred during the performance of the operation, which was already commenced; in eight cases the operation, being of short duration, was completed before it was discovered that the patient had expired. In two or three of these latter cases, it was thought that the patient was probably dead when the operation was begun. In the remaining seventeen cases, the inhalation was discontinued at some period of its progress, owing to the sudden occurrence of alarming symptoms. In some of these cases, death took place quite early in the inhalation, before the patient had evinced any of the usual signs of the influence of chloroform, and it is extremely worthy or remark that, in every accident, the particulars of which are related, the symptoms of real danger set in suddenly, whether they appeared during the inhalation or after it was discontinued.
A commission appointed by the Academy of Medicine of Paris, in 1849, to report on the fatal case which occurred at Boulogne, denied that the death in question was caused by chloroform, on the ground that this agent always produces intoxication and insensibility before death. M. L. Lallemand also expressed a similar opinion last year, as the reporter of an experimental enquiry undertaken by the Society of Emulation of Paris. He stated that the phenomena produced by chloroform are "always manifested in the same order, and with the same characteristics," and that the respiratory movements always cease before the action of the heart."*
(*See L'Union Médicale, 1855, No. 13.)
These commissions are, however, in error as to a simple matter of fact; what they say is only true of chloroform when the vapour is diluted with air to a considerable extent; with a less amount of dilution, chloroform may cause sudden death by paralysing the heart, without its usual effects being apparent; and I can kill animals suddenly with it, as with vapour of prussic acid, without inducing previous intoxication or insensibility.
In all cases of death from chloroform, in which the state of the pulse at the time of the accident is described, it was found to cease suddenly and abruptly, and in only two of the cases was there the slightest indication of returning pulsation, for a brief interval. In several cases, indeed, it was observed that the very last pulsation was equal in strength to the ordinary ones. This is entirely different from what takes place in asphyxia. Under a total privation of air, the pulse retains its usual strength for a minute or two, and then gradually diminishes in frequency and force during two or three minutes, till it finally ceases.
In twelve of the recorded cases of accident, the face was observed to become suddenly pale at the moment when symptoms of danger set in. This symptom probably occurred in many of the other cases, but was either not observed, or if so, not recorded. I need hardly say that sudden pallor of the countenance is indicative of death beginning at the heart, and is irreconcilable with asphyxia.
In four of the instances in which death occurred during the performance of an operation, the attention of the surgeon and his assistants was first called to the patient's danger by the sudden cessation of the bleeding—-a phenomenon which proves the occurrence of sudden syncope even more strongly, if possible, than the circumstances previously mentioned.
A fact which also shows clearly, that in the accidents from chloroform, death has not taken place by asphyxia, is, that when animals are killed by it very suddenly, so that death occurs in the same manner as in the accidents to the human subject, the blood is found to be of a florid colour in the lungs, if the body is opened immediately after death.
Except in the case of children and lunatics, who cannot always be persuaded to inhale chloroform, the patient breathes it voluntarily, but it would be manifestly impossible that a patient should willingly go on suffering from a want of breath, owing to the pungency of the vapour, without making any complaint, until he should die from this cause, or even become unconscious. As regards children and lunatics, no accident from chloroform is known to have happened to them. Persons do indeed complain sometimes of a choking feeling, and want of air, but the practice is to humour them at first, and restraint is never applied, except in the excitement and struggling that sometimes occur from the genuine effects of chloroform, after unconsciousness has been induced.
The vapour of sulphuric ether is as pungent and irritating as that of chloroform, if not more so, and, therefore, if the accidents were occasioned by the pungency of the vapour preventing the access of air to the lungs, they would be quite as liable to occur under the exhibition of ether as that of chloroform. But accidents during the inhalation of ether were extremely rare; only two are known to have occurred, and these, I believe, not from the effects of the vapour. In one of these cases, which occurred at the Hôtel Dieu d'Auxerre, the patient seemed to die by asphyxia, not occasioned, however, by the pungency of the vapour, but, more probably, the narrowness of the tubes of the inhaler. Symptoms of distress commenced when the man had been inhaling three minutes, and continued till the time of his death, at the end of ten minutes, the apparatus being kept applied the whole time. I need hardly say that no case resembling this has occurred during the exhibition of chloroform. In the other case which happened at the Hôtel Dieu de Lyons, the patient died of sudden syncope, caused, in my opinion, by loss of blood during the removal of the superior maxillary bone--an operation which the surgeon had been reluctant to undertake, on account of the weakness and general bad state of the patient.
In a few cases of death from chloroform the countenance has been observed to become turgid and dusky just after the circulation ceased. This circumstance has been thought to indicate death by asphyxia, which is an error. Although not of itself proving the kind of death, the turgid and dusky state of the face is what must take place from sudden arrest of the action of the heart in patients who are not deficient of blood. The moment the heart ceases to beat, its right cavities become distended, and no more blood can enter them from the veins; but the arteries are emptied by their contractility through the molecular forces connected with the circulation through the capillaries, and consequently the veins become distended, even to their radicles.
In several of the fatal cases of exhibition of chloroform there was considerable struggling, either before the real symptoms of danger set in, or just as the circulation ceased, and Dr. Black considered that these efforts indicate asphyxia. In many of the cases the struggling arose, no doubt, from the ordinary effect of the vapour on a certain class of patients, whilst in a few patients who died suddenly, without first being rendered insensible, there was a spasm at the time the heart ceased to beat, analogous to what one often sees when animals are bled to death. In asphyxia, the convulsions cease before the action of the muscles of respiration, and the heart continues to beat distinctly for two or three minutes longer, but it has not done so in any fatal case of the exhibition of chloroform.
If it were possible for a medical man to overlook or misunderstand the symptoms induced by vapour of chloroform when sufficiently diluted with air, and to go on administering it till the patient should die, the death would very much resemble one by asphyxia; for the respiratory muscles would first cease to act, and the circulation would be gradually brought to a stand by the failure of the respiration; of this I am satisfied from very numerous experiments upon animals. There has been no cases recorded, however, of death occurring in this manner during the exhibition of chloroform. In the few cases where persons have lost their lives by imprudently inhaling the vapour when no one was present, death has most likely taken place in this way, but this cannot be known for a certainty. In this mode of dying from chloroform, as well as in asphyxia, there are often two or three gasping efforts at inspiration directly after the heart has ceased to beat; and if fresh air is allowed to enter the lungs during these efforts, the circulation is in many cases restored, both in asphyxia and narcotism from chloroform.
Dr. Sibson made the remark, in 1848, that during the inhalation of chloroform the blood which circulates in the coronary arteries must be more highly charged with vapour than that in any other part of the body except the lungs. When the chloroform is exhibited in a gradual and uniform manner, this circumstance is of no consequence, as the heart is capable of bearing a greater proportion of chloroform than the brain; but when the vapour is not sufficiently diluted the case is different, and the suggestion of Dr. Sibson affords the best explanation of those fatal cases, and of some experiments I have performed on animals, in which the action of the heart has ceased before the breathing. In a few of the fatal cases the period of inhalation was so short that it is impossible that the chloroform could have been equally diffused throughout the system, and the quantity of chloroform used was so small that no harm could have resulted if it had been thus diffused. In a case which occurred at Ulm, a lady, in good health and spirits, took but five inspirations of chloroform, when she expired; but it is impossible that, in a quarter of a minute, even a tenth part of the blood in the body could pass through the lungs and become charged with chloroform. A portion only of the blood was thus charged, and the mode of dying showed that it acted fatally on the heart.
There is a very common mistake with regard to the action of carbonic-acid gas, which has led to an erroneous opinion of the effects of chloroform in more than one quarter. Undiluted carbonic-acid gas is known to cause death very quickly, and it is generally believed to do so by causing spasm of the glottis; but spasm of the glottis would not cause death more quickly than tying the windpipe, or immersing the head in the water, and the mode of dying would be the comparatively slow one of asphyxia. When an animal is placed in a jar of this gas, over water, the gas is seen to diminish considerably in volume, as it is absorbed into the blood with each inspiration. Moreover, I have never myself had any difficulty in inhaling pure carbonic-acid gas, by small quantities--fifteen or twenty cubic inches--at a time, since I first tried nearly twenty years ago.*
(*See Cyclopedia of Practical Surgery, article Asphyxia, by T.B. Lucas, p. 440.)
The gas causes no particular sensation till it reaches the lungs, when there is a tendency to cough and a feeling of tickling in the throat. It is advisable not to attempt to fill the lungs with this gas, for it has an unpleasant way of upsetting the dogma that narcotism is necessarily gradual and progressive.
As we have seen that all the accidents during the exhibition of chloroform have been caused by the air breathed by the patient being, at some moment, too highly charged with the vapour, it follows, that to prevent such accidents it is only necessary to insure that the vapour shall at all times be sufficiently diluted with air. The most fatal error with regard to chloroform has been to suppose that the patient was safe so long as he was supplied with sufficient air for the purposes of respiration; for the truth is, that the more air the patient breathes the greater is his danger, if the air be over highly charged with the vapour. Sudden death from this cause may happen at any period of the exhibition of chloroform, and a few accidents have occurred almost at the beginning of the inhalation. It is, however, a mistake to suppose that the danger from vapour not sufficiently diluted is greatest at the beginning of its administration. The danger from this cause increases as the patient comes under the influence of the chloroform, and as the blood absorbs more and more of it, the greater number of deaths having occurred after the patients were first rendered quite insensible. In the beginning of the inhalation, it is, indeed, necessary to give the vapour in a state of greater dilution than afterwards, in order that it may not be needlessly disagreeable to the patient; but there would be no danger in commencing at once with vapour diluted only with 95 per cent of air, as I know by very numerous experiments on animals.
The means which I employ to regulate the amount of vapour in the air breathed by the patient is an inhaler, which has been described on a previous occasion, and which enables me to effect that object near enough for practical purposes. In using a handkerchief or sponge, the danger of the vapour being breathed in a too concentrated state may be prevented by diluting with an equal measure of rectified spirit. Air at 60º Fah. is capable of taking up 14 per cent of vapour from pure chloroform, and although it never gets fully saturated in the ordinary process of inhalation, the result shows that it has on many occasions taken up, at some moment, a great deal too much. When diluted with an equal measure of spirit, chloroform will only yield 8 per cent of vapour at 60º Fah., even if the air were quite saturated with the mixed vapours. In practice, it yields enough to induce insensibility, without any risk of causing a sudden accident.
Artificial respiration, very promptly and efficiently performed, is almost the only measure which promises a prospect of relief in cases of accident from chloroform. It is the only thing which I have ever found to restore animals, when it was clear that they would not recover spontaneously from the chloroform. Electricity seems to be injurious, by exhausting the remaining sensibility; but opening the jugular vein is advisable, in cases where the veins are turgid, in order to relieve the distention of the right cavities of the heart.
Sackville-street, January, 1856.
Return to John Snow Publications
100. "The mode of propagation of cholera"
Source: Snow, John. Association Medical Journal 4, 16 February 1856, [Letter to Ed.].
[In the letter below, Snow refers to the following passage from Shuttleworth's address: "Animal and vegetable physiology already rest upon results of chemical inquiry, and it will yield further secrets to the microscope, to analysis, and to experiment. In like manner, the phenomena of disease must be investigated. The discoveries of Dr. Semelweiss as to the mode of the propagation of puerperal fever by the cadaverous poison, and Dr. Budd's discovery of one mode of the dissemination of cholera by a poison evolved in the early stage of decomposition of the specific secretions, are facts which indicate, though they may not prove, the influence of virus (meaning the morbid matter specific to a particular disease) on the constitution of the blood, and the action of that fluid in a state of a disease on the solid parts. But perhaps the experimentum crucis of this department of observation consists in the discovery of Jenner." (abstracted in the Association Medical Journal 4 (9 February 1856): 118].
Letter from John Snow, M.D.
Sir,--It appears from the interesting report in the Journal of to-day of the address of Sir James Kay Shuttleworth at Manchester, that he alludes in complimentary terms to my conclusions regarding the propagation of cholera, as modified by a suggestion of Drs. Thiersch and Pettenkofer, but he erroneously attributes these views, so modified, to Dr. W. Budd. Dr. Alison fell into a similar mistake, which was afterwards rectified in the journal in which it had appeared--the Edinburgh Medical Journal--and I suspect that it is Dr. Alison's mistake which has misled Sir J. K. Shuttleworth. A few weeks after the first edition of my essay on cholera appeared, in 1849, Dr. W. Budd published a pamphlet on the subject, in which he adopted my views, and made a full and handsome acknowledgement of my priority. In the latter part of 1854 he also published a series of papers in the Association Medical Journal, containing some interesting facts in support of these views. These papers were published at first with the signature of "Common Sense"; but Dr. W. Budd avowed the authorship before their conclusion. In the number of the Journal for December 22nd, he gave a qualified adhesion to the opinion of Drs. Thiersch and Pettenkofer, that some kind of change or fermentation is necessary in the peculiar excretions of cholera to enable them to propagate the disease. This is a modification of my original views, which I, however, see no reason to adopt. In one or two places in his papers in the Association Journal, Dr. W. Budd advocates the propagation of cholera through the air, by means of the excretions, to a greater extent than I am inclined to admit; but with this and the before mentioned exceptions, his opinions respecting every point connected with the pathology and mode of communication of cholera are exactly those which I first published in 1849, and have since maintained.
I have not made the above remarks by way of complaint; but as my researches respecting cholera were conducted with great labour, and very much to the detriment of my more immediate interests, I feel it a duty not to allow the credit of them to pass from me by a mere mistake.
I am, etc.,
John Snow.
Sackville Stree, 8th February, 1856.
Return to John Snow Publications
101. "The mode of propagation of cholera"
Source: Snow, John. Lancet 1, 16 February 1856, p. 184 [Letter to Ed.].
To the Editor of the Lancet
Sir,--I did not, until to-day, read the important and interesting Address of Sir J. K. Shuttleworth, Bart., in the Lancet of the 2nd instant. I find that he alludes in complimentary terms to my conclusions regarding the propagation of cholera, as modified by a suggestion of Drs. Thiersch and Pettenkofer, but he erroneously attributes these views, so modified, to Dr. W. Budd. Dr. Alison fell into this mistake, which was afterwards rectified in the journal in which it appeared—-the Edinburgh Medical Journal; and I suspect that it is Dr. Alison's mistake which has misled Sir J. K. Shuttleworth. A few weeks after the first edition of my essay on Cholera appeared, in 1849, Dr. W. Budd published a pamphlet on the subject, in which adopted my views, and made a full and handsome acknowledgement of my priority. In the latter part of 1854 he also published some interesting facts in support of these views, and afterwards gave a qualified adhesion to the opinion of Drs. Thiersch and Pettenkofer, that some kind of change or fermentation is necessary in the peculiar excretions of cholera, to enable them to propagate the disease. This is a modification of my original views which I, however, see no reason to adopt. In one or two of his papers Dr. W. Budd advocated the propagation of cholera through the air, by means of the excretions, to a greater extent than I am inclined to admit, but with this and the before mentioned exception, his opinions respecting the pathology and mode of communication of cholera, as expressed in those papers, are exactly those which I first published in 1849, and have since maintained in several papers before the Medical Societies, and in a second edition.
I have not made the above remarks in the way of complaint; but as my researches respecting cholera were conducted with great labour, and very much to the detriment of my more immediate interests, I feel it a duty not to allow the credit of them to pass from me by a mere mistake.
I am, Sir, your obedient servant,
John Snow, M.D.
Sackville-street, Feb. 1856.
Return to John Snow Publications
102. "Case of purpura hemorrhagica"
Source: Snow, John. Association Medical Journal 4, 3 May 1856, pp. 364-65 [Letter to Ed.].
By John Snow, M.D., London.
The following case presented an appearance which is not clearly described in the works with which I am acquainted.
CASE. I was called on Aug. 13th, 1855, to see a patient, aged about 45 years. He is a mechanic, in business on his own account. He had formerly a good constitution, and enjoyed good health; but within the last few years he had acquired a habit of hard drinking, and has suffered from attacks of dyspepsia and a morbid sensibility of the nervous system. On the present occasion, he had been drinking to excess for two or three weeks, and eating scarcely any food. I was sent for on account of a copious bleeding from his nose, which he had, however, stopped before my arrival, by the application of turpentine on cotton wool. There were large ecchymoses on his arm, hands, thighs, and legs, and some smaller ones on his head. They had appeared at various times within the three previous days, and some of the earlier ones were already fading. In the centre of each patch of ecchymosis there was small hard tumour, over which the skin was quite white. These tumours or nodules felt almost as hard as cartilage, and were proportionate in size to the ecchymosis: where these were as large as the hand, the tumours were as big as a horse-bean; where the purple patches were smaller, so were the tumours. The pulse was bounding but compressible; there was great debility, and the limbs were rather tremulous. He was treated with lemon-juice and decoction of cinchona with dilute sulphuric acid, and was directed to take such nourishing food as his appetite would permit. He improved during the next two days. On the 15th, the patches of ecchymosis had faded considerably, and the nodules were diminished in size.
I was sent for again on the 18th, and found the patient labouring under a rather severe attack of erysipelas of the face and head. He took quinine and nourishing diet; nitrate of silver was applied externally; and on the 26th, he was convalescent.
REMARKS. I consider that the small hard tumour situated in the centre of each patch of ecchymosis consisted undoubtedly of the fibrin of the blood, which had coagulated quickly at the point where it escaped from the ruptured vessel, whilst the serum and globules spread all round in the cellular tissue. The above case of purpura did not differ in any essential particular from that important variety of the disease we call scurvy; and although in some cases of scurvy the blood seems to have lost its power of coagulating, there are other cases in which this fluid coagulates more quickly and strongly than usual. This was remarked by Dr. Milman, who wrote on scurvy in 1782, and attributed the disease to impaired nutrition of blood-vessels. Dr. Budd has since observed that the blood in many cases of scurvy retains its power of coagulating undiminished.
Although I have not observed the above mentioned little tumours in any other case of purpura, I cannot consider this to be a solitary instance of their presence. I think it probable that they may have been passed over, as belonging to what is called purpura urticaria. The tumours, however, have no relation to the wheals of urticaria, and do not in the least resemble them.
Sackville Street, April 1856.
Go to Group 13 (# 103-113)
Click to return to Stream 1 - d: John Snow's Publications
Click to continue to Stream 1 - e: Memoir of his friend Benjamin Ward Richardson
 (# 88-102 )
(# 88-102 ) Return to John Snow Publications
Return to John Snow Publications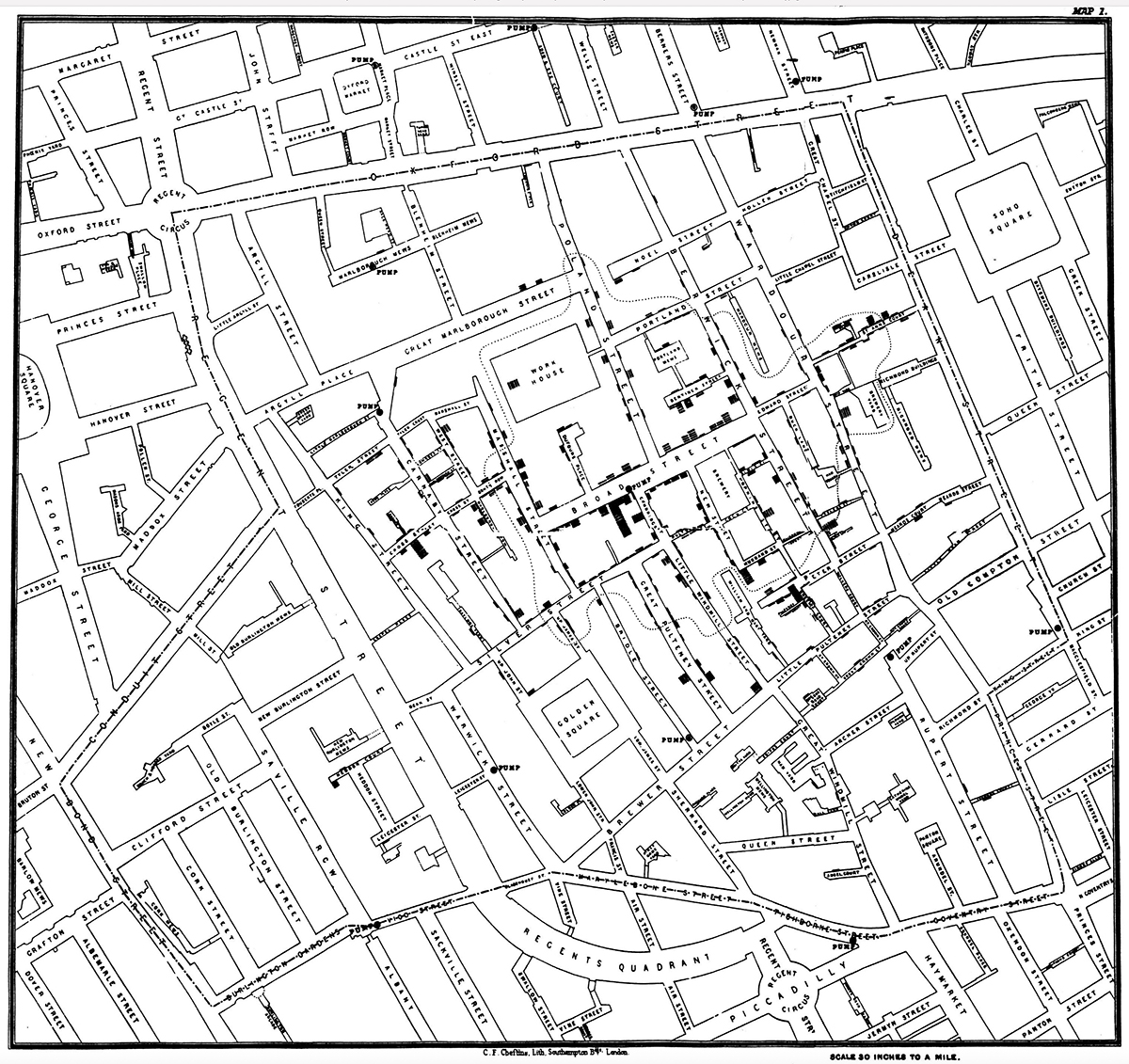
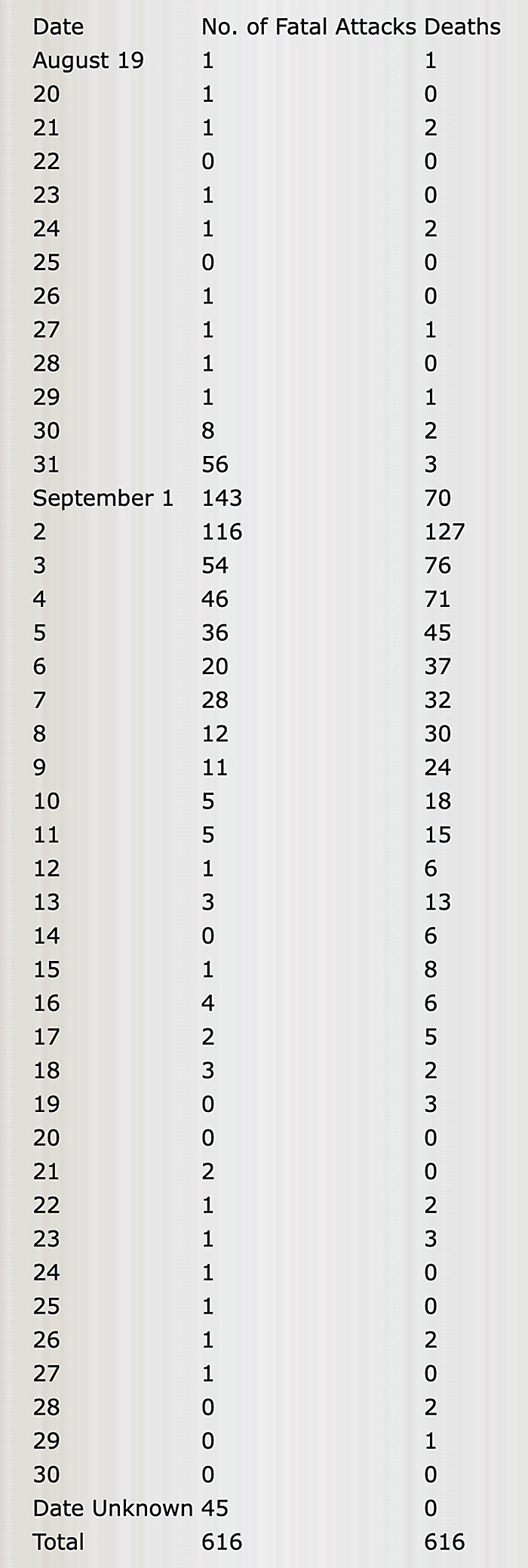
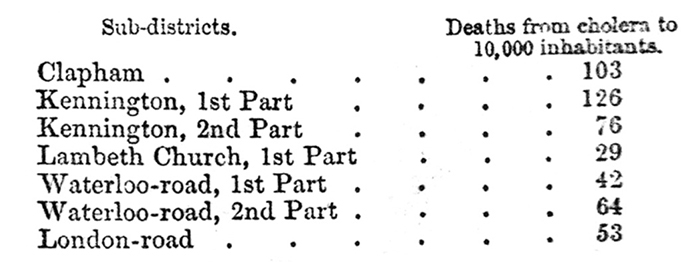
 (# 103-113)
(# 103-113)
