d13: John Snow's Publications - Group 13 (# 103-113)
Return to John Snow Publications
103. "Chloroform"
Source: Snow, John. Medical Times and Gazette 12, 21 June 1856, pp. 680-81 [Letter to Ed.].
(To the Editor of the Medical Times and Gazette)
Sir,--I shall feel obliged if you will allow me to state, with respect to the case mentioned by Mr. Witten, and the question he asks in your Journal of to-day, that every patient may inhale the quantity of choloroform [sic] he mentions, vis., 8 or 9 drachms, without being rendered unconscious, provided the inhalation be extended over a sufficiently long time. It is the custom to give it so in certain cases of labour, especially during the first stage. On the other hand, I am satisfied, by long and careful observation, that every patient may be rendered insensible by the vapour of one fluid drachm of this agent, provided it be inhaled continuously and without intermission, and be diluted with not more than fifteen hundred cubic inches of air. I have had to give chloroform to a number of patients on whom large quantities of chloroform had previously been used without effect, and I have not found that any of them required to inhale more than other persons of similar bulk and strength.
Whenever I have met with unusual delay in rendering [a] patient insensible, I have been able to trace it to the circumstance, that the vapour did not enter the lungs in sufficient quantity with the inspired air. When the vapour enters the lungs, a large portion of it is necessarily absorbed into the blood; and being in the blood, it cannot help acting on the brain and nerves, according, as I feel assured, to a regular and definite law. But exhalation goes on in the lungs, as well as absorption; and if the inhalation of the vapour is interrupted only by a few seconds, the patient loses part of the chloroform which had previously been absorbed; moreover, if the vapour be too much diluted with air, there comes a point where the exhalation from the blood in the lungs balances the absorption, and no further effect can be produced though a person should inhale for hours. The true reason why Mr. Witten's patient did not become unconscious is, that the quantity of chloroform present in the circulating fluid never at any moment reached twelve minims, and was probably much below that amount.
I am, etc.,
John Snow, M.D.
Sackville-street, June 14.
Return to John Snow Publications
104. "Cholera and the water supply"
Source: Snow, John.Times 26 June 1856, p. 12, col. B, [Letter to Ed.].
(To the Editor of the Times)
Sir,--I shall be obliged if you will allow me to make a few remarks on the report of Mr. Simon to the Board of Health which forms the subject of a leading article [editorial] in the Times of to-day. This report, although valuable in some respects, contains, from the nature of it, only an approximation to the truth. The population supplied with the impure water of the Southwark and Vauxhall company suffered a mortality from cholera in the late epidemic not merely three and a half times as great as that supplied by the Lambeth Company, but six times as great; and even this fact expresses the influence of the impure water in an inadequate manner, unless the different periods of the epidemic are considered separately. The inquiry which supplies the matter for Mr. Simon’s report was not an original one undertaken during the epidemic, but an additional investigation made under very disadvantageous circumstances after the epidemic was over. Early in the epidemic of 1854 I commenced a personal inquiry respecting every death from cholera which occurred in the districts in which the water supply of the above companies is intermixed. For the first four weeks of the epidemic I was furnished with the list of deaths published in the weekly returns of the Registrar-General, and for the next three weeks I was permitted to copy the addresses at the General Register-office. During the succeeding ten weeks which [while?] the epidemic continued the Registrar-General obtained from the district registrars a return of the water supply in which fatal attacks of cholera took place. The results were as follows:--In the first four weeks of the epidemic the deaths from cholera were 14 times as numerous among the population supplied with the impure water of the Southwark and Vauxhall company as among that supplied with the better water of the Lambeth Company, taking into account the respective number of these populations. In the next three weeks the mortality was 7 ½ times as great, and in the last ten weeks of the epidemic nearly five times as great in one population as the other, or, taking the whole epidemic, the difference was as 6 to 1. The relative mortality increased during the progress of the epidemic among the customers of the Lambeth Company just as it increased in the north and central districts of London, which were supplied with water which did not contain any of those impurities which take part in the propagation of cholera. This circumstance can be explained when the other causes which assist in the propagation of the disease are taken into account as well as the water. The inquiry conducted by Dr. Farr, of the General Registrar-office, and myself referred to the houses in which the fatal attacks took place; that of Mr. Simon refers to the houses in which the deaths occurred: but, as many persons fatally attacked in houses supplied by the Southwark company were removed before death to Lambeth Workhouse and other buildings supplied with water by the Lambeth Company, the latter mode of inquiry does not accord a correct result of the influence of the water. The results of my inquiry were published briefly in the Medical Times of September the 2d and October the 7th, 1854, and those of the General Registrar-office in the weekly returns of October and November, 1854. Both of these sets of results can be shown to harmonize with the amount of mortality in the respective sub-districts, while those of Mr. Simon’s inquiry do not. The mortality from cholera in the autumn of 1853 is included in the tables of Mr. Simon’s report, but that ought not to affect the result, for the deaths at that time were few, and took place, like those in the commencement of 1849, almost exclusively among the population supplied with water by the Southwark and Vauxhall Company.
I should like to say, in conclusion, that many other diseases, beside cholera, can be shown to be aggravated by water containing sewage, and that since the Southwark Water Company has obtained a supply almost equal in purity to that of the Lambeth Company the mortality of the south districts of London has greatly diminished.
I am, Sir, your obedient servant,
John Snow, M.D.
18, Sackville-street, June 25
Return to John Snow Publications
105. "Administration of chloroform"
Source: Snow, John. Medical Times and Gazette 13, 5 July 1856, p. 21, [Letter to Ed.].
To the Editor of the Medical Times and Gazette.
Sir,--I consider that the time over which the inhalation extended in Mr. Witten's case of administration of chloroform explains the want of success, when we take into account the circumstance, that with the form of inhaler which he used only a part of the chloroform is taken into the lungs, and that a great portion is blown away by the warm breath during expiration. Mr. Witten would probably say that he has succeeded in other cases when using the same inhaler, apparently in the same manner. But the effect produced depends entirely on the proportion of chloroform vapour in the air breathed by the patient, and this varies, in using such an inhaler, with a number of circumstances which may easily pass unobserved; as, the accuracy with which the inhaler fits the face, the temperature of the sponge, and the amount of air which passes through it before being breathed. I have not found that the nervous temperament has rendered patients less susceptible to the influence of chloroform, and, as regards the deterioration of the blood, no amount of it which is consistent with life could affect the absorption of the vapour in the lungs, which is a strictly physical process.
With respect to my statement, that twelve minims of chloroform, when present in the blood, causes unconsciousness, I am able to adduce not only a calculation, but a direct experiment, in proof of it. The calculation is founded on some experiments which I published in the Medical Gazette for 1848, Vol. I. I found, that when animals were made to breathe air containing as much vapour of chloroform as would enable the blood to take up one fifty-sixth part, as much as it is capable of absorbing, it produced what I call the second degree of narcotism; a state in which the animals were incapable of perceiving what was occurring around them. Now, the serum of the blood, like other watery fluids, is only capable of dissolving about one part in 288 of its volume of chloroform; and if this number be multiplied by 56, and the quantity of serum in the body, (which, according to the experiment of Valentin, averages 410 fluid ounces,) be divided by the product, the result is 12 minims. The direct experiment is as follows:--If 12 minims of chloroform be put into a good-sized bladder, with 400 to 500 cubic inches of air, and an adult person breathes it backwards and forwards, as he would breathe laughing gas, he becomes quite unconscious in less than a minute; not sufficiently insensible for a surgical operation--for that would require about 18 minims--but he becomes altogether oblivious of everything about him. It is not necessary or desirable to exhaust the lungs before performing this experiment. The 12 minims of chloroform are undoubtedly diffused through the blood of the whole body. When animals are killed with chloroform I can detect it by chemical analysis as easily in the muscles as in the brain, and I found it readily in the leg of a hog, which was amputated while he was under the influence of the vapour. The quantity of chloroform in the brain at any one time is much less than a single minim, but this need not surprise us when we know in what small quantities the alkaloids produce their effects. Chloroform appears to produce its effects without undergoing any change itself; for, after a person has inhaled it, the vapour may be detected by chemical tests coming off unchanged in the breath; it can be detected in the bodies of animals killed by it, for a fortnight after death; and, lastly, by breathing it, mixed with oxygen, from a bladder, and making an arrangement to absorb the carbonic acid produced, the effect of a small quantity may be kept up for an indefinite period, and a few minims can be made to do the work of several drachms.
I am, etc.
John Snow, M.D.
18, Sackville-street, June.
Return to John Snow Publications
106. "On the supposed influence of offensive trades on mortality"
Source: Snow, John. Lancet 2, 26 July 1856, pp. 95-97.[Letter to Ed.].
By John Snow, M.D.
The science of public health, like other branches of knowledge, may be as much benefited by the removal of errors which stand in the way of its progress as by direct discovery; and it is with this conviction that I send for publication the result of an examination into a portion of the Registrar General's very valuable Weekly Returns of Deaths in London. Whilst a number of eminent authors have for a long period attributed the generality of epidemic or zymotic diseases to special poisons passing in some way from one patient to another, an active section of the profession has attributed the greater number of these disease to a variety of general causes, and in particular has asserted that they were occasioned, or greatly aggravated, by offensive gases proceeding from putrefying materials, even [95/96] though these materials did not proceed in any way from sick persons.
An opportunity is now afforded of examining this question on, as I believe, a larger scale than previously. For the last eighteen months the Weekly Returns of the Registrar General have contained the occupations of males aged 20 years and upwards whose deaths have been registered, and at the end of each quarter of a year the aggregate results have been given in a table. The causes of death are not contained in the table; but the diseases which offensive trades are presumed to promote are such as would increase the mortality, and in fact the mortality of persons in any occupation is the best criterion of its salubrity. The entire number of males aged 20 years and upwards in the metropolis at the last census was 632,545, and the number of deaths in this division of the population, in the year and a half just expired, was 22,889, being at the rate of 241 per annum in 10,000. The number of persons aged 20 years and upwards working and dealing in animal substances was 40,004 in 1851, and the number of deaths in the last eighteen months, 1210, being at the rate of 201 per annum in 10,000, or five-sixths as many as in the entire male population of 20 years and upwards. The greater number of persons working and dealing in animal substances are, however, occupied amongst silk, wool, and hair, which are in no way offensive; and I therefore thought it desirable to separate those trades which I believe to be really offensive, and I have included in the accompanying table all such occupations in which any death has occurred during the last six quarters. These occupations include 6943 persons, of whom 214 died, being at the rate of only 205 per annum in 10,000, which is greatly below the mortality of the whole male population of 20 years and upwards. There are some offensive trades in which no death occurred during the last eighteen months. If these trades had been included in the table, the mortality would have been shown to be lower than it appears. Butchers, poulterers, and fishmongers have sometimes been considered to follow offensive trades; but although these persons may occasionally, by a neglect of their duty and interest, be exposed to offensive gases, their proper occupations cannot be considered offensive, and I have therefore not included them in the table.
The Registrar General has very properly remarked that "As the persons engaged in various callings are distributed in different proportions through several periods of life, and as the rate of mortality depends on age, an analysis of the ages of the living and dying must be made before deductions regarding the comparative salubrity of professions can be drawn with safety." In comparing the mortality of a single occupation, or any group of occupations, with that of the whole population, however, one acts as if all the persons in these occupations had entered them before the age of 20; and therefore any fallacy from the above cause tells against the occupations examined, and not in their favour. For instance, according to the figures in the above table, the expectancy of life for the whole male population of London, at the age of 20 years, is 41.4 years, or, in other words, the average duration of life in those persons would be over 61 years; whilst in the persons engaged in the offensive trades enumerated in the above table, the expectancy of life at 20 would be over 48½ years, and the average duration of life over 68½ years; but if some persons enter these trades later in life than 20 years, then the expectancy of life at 20 is greater, and the average duration of life is greater in those who arrived at 20. The mortality amongst the licensed victuallers and beershop-keepers has been at the rate of 373 per annum in 10,000 during last eighteen months; but part of this high mortality is undoubtedly due to the circumstance that a great number of persons do not enter these trades till they are advanced much beyond twenty years of age. All these facts tend to show that if the above table does not express accurately the morality of persons engaged in offensive trades, it errs by making the mortality appear greater, and not less, than it really is. I am quite aware that, as time rolls on, the returns of the Registrar General will afford a greater body of facts regaling offensive occupations; but, during the six quarters that have already elapsed since these returns were commenced, the results have been pretty uniform, and are, in my opinion, sufficiently important to be commented on. The health of persons employed in any occupation is necessarily the best measure of the effects of any such occupation on the public health. As the gases given off from putrefying substances become diffused in the air, the quantity in a given space is inversely as the square of the distance from their source. Thus, a man working with his face one yard from offensive substances would breathe ten thousand times as much of the gases given off, as a person living a hundred yards from the spot. Currents of air would make a difference; but this would be the average proportion of the gases inhaled respectively by the two individuals. There are, moreover, so many causes which influence the health of a neighbourhood, that it would be almost impossible to judge from that alone of the effect of trades or occupations conducted in it. I of course attribute no benefit to offensive smells; and the reason why the persons employed in the callings I am treating of enjoy a greater longevity than the average, is probably because they are less exposed to privation and less addicted to intemperance than men following many other occupations, and because, as a general rule, they do not lead a sedentary in-door life. It is sometimes argued, that since the gases given off during putrefaction are capable of causing death when in a somewhat concentrated form, they must necessarily be injurious in the most minute quantity; but this by no means follows: for carbonic acid gas, which is a well-known poison when present in large quantity, is a natural consistent of the atmosphere; vapour of ammonia is sniffed without hesitation, and even sulphuretted hydrogen is absorbed, in considerable quantities, by the visitors at Harrogate and some other watering places.
Cholera has not been present during the eighteen months for which the mortality in different occupations has been published; but there are certain facts which bear on the alleged influence of offensive trades on this disease. A great number of skin yards, bone boiling establishments, and other offensive factories are situated in that part of Lambeth which extends by the river side from Westminster-bridge to Vauxhall-bridge, and constitutes the sub-district called Lambeth Church, 1st part. This part of Lambeth contains also many of the other conditions which are supposed to, or which really, promote the prevalence of cholera. It is crowded with a poor population, wherever the ground is not occupied with the factories above mentioned, and it lies by the river-side, at an elevation of only two feet above Trinity high-water mark, yet the deaths from cholera in 1854 were only 29 to each 10,000 inhabitants, whilst in London at large they were 45 in 10,000; in the sub-district of Kennington, 1st part, less densely inhabited, they were 126, and in Clapham 103 in 10,000, the latter being a genteel, thinly inhabited sub-district, at the elevation of 21 feet. Again, the sub-district of Saffron-hill, with the slaughter-houses, knackers' yards, and catgut factories of Sharp-alley on its eastern boundary, and the Fleet-ditch, at that time uncovered, flowing through it, suffered in 1854 a mortality from cholera of only 5 in 10,000; being one-ninth of that of the metropolis generally, and one-twelfth of that of the Belgrave sub-district, where the mortality was 60 in 10,000. These circumstances might be thought to prove a little too much, were it not that the prevalence of cholera is influenced by a variety of circumstances, and in London very much by the nature of the water supply; for, in the short but severe epidemic of 1854, the chief medium of its propagation in the metropolis was water, containing what-[96/97] ever passed down the sewers from previous patients. The sub-district of Bermondsey, called the Leather-market, which contains a number of factories for skin-dressing, suffered, in 1854, exactly the same high mortality as the other five sub-districts in the South division of London, which, like it, were supplied exclusively with the impure water of the Southwark and Vauxhall Company. The conclusion to be drawn from all these facts is, that the vicinity of offensive factories leaves the cholera to pursue the same course that it would do in their absence.
Sackville-street, July, 1856.
Return to John Snow Publications
107. "Cholera and the water supply in the south districts of London in 1854"
Source: Snow, John. Journal of Public Health and Sanitary Review 2, October 1856, pp. 239-57.
In the summer of 1849, I published certain conclusions at which I have arrived with regard to Asiatic cholera, and the facts and reasonings which had led to them. The following is a very brief outline of these views. The cholera commences as an affection of the alimentary canal, and not with general illness; there is no evidence of poisoning of the blood in this disease, except in some cases where secondary fever occurs; there is conclusive evidence that cholera may be communicated from person to person, and it follows, therefore, that the morbid matter which produces the disease is applied to the interior of the alimentary canal, where it increases and multiplies during the period of so-called incubation, and passes off, during the attack, to cause fresh cases when suitable opportunities occur. Various circumstances connected with the propagation of cholera seemed in accordance with the above view of its pathology. Thus, it was observed to pass frequently from person to person in the crowded habitations of the poor, who eat, drink, cook, and sleep in the same apartment, and pay little or no regard to cleanliness, who live, in fact, under circumstances where the sudden and copious evacuations of cholera, soiling the bed and body linen, would not fail to contaminate the hands of the patient and his attendants, and be thence transferred to any food they might touch. The absence of colour and odour in the evacuations could not help to favour this result. The social visitor who came to see the poor patient, or attend his funeral, frequently suffered, whilst the medical man, and others who partook of no food in the apartment, and who washed their hands when requisite, escaped. The mining districts of this country have suffered excessively from cholera in each epidemic, an event which might be explained by the following circumstances when taken in connexion with the above view of the cause of the disease. The miners stay eight or nine hours at a time in the pits, and take food with them, which they eat invariably with unwashed hands, and without knife and fork, whilst the pits are without privies, and are generally extremely foul and dirty. The entire absence of daylight must also cause the workmen to take much more dirt with their food than they [are] aware of. It occurred to me, as soon as I began to entertain the above opinions, that if the cholera excreta could reproduce the [239/240] disease in the way just mentioned, they might also do so when diffused in water taken as drink, and that unless this were the case, the whole of the phenomena of cholera, as an epidemic, could not be explained. I, therefore, sought anxiously, and waited patiently, for some confirmation of this part of the subject before I should make my views known. Two outbreaks of cholera occurred, however, about the end of July 1849, one in Horsleydown, and the other in the Wandsworth Road, which I investigated, and which afforded what I considered conclusive evidence on the subject. The water drank by the persons attacked in each of outbreaks had received, amongst other impurities, what must have come from a patient previously ill of the disease. I was able also to point out that the cholera was prevailing most in those districts of the metropolis which received their supply of water from certain parts of the Thames which contained the sewage of the town, and, consequently, whatever proceeded from the cholera patients. Before the end of 1849 I was able to show that a very close connexion existed between the mortality from cholera and the nature of the water supply, not only in London, but throughout the country. This connexion was very evident in certain towns, as Exeter and Hull, where the supply of water had been changed between the epidemic of 1832 and that of 1849. Where a polluted supply was changed for an unpolluted one, the cholera was almost prevented; and where a scanty but unpolluted supply had been changed for one contaminated with the sewage of the town, the epidemic prevailed to a fearful extent. The attention of Dr. Wm. Budd and Dr. Farr was directed to this subject, with the result of confirming what I had stated.
Between the epidemics of 1849 and that of 1853, one of the water companies supplying the south districts of London changed its source of supply from the middle of the town, near the foot of the Hungerford Suspension Bridge, to Thames Ditton, at a part of the river which is beyond the influence of the tide, and, therefore, out of reach of the sewage of the metropolis. In the autumn of 1853 it was shown by Dr. Farr* that the districts partly supplied by this, the Lambeth Water Company, with improved water, suffered less than the districts supplied entirely by the Southwark and Vauxhall Company with the water from the river at Battersea Fields, although in 1849 they had suffered rather [240/241] more than the latter districts.
(* Weekly Returns of Deaths, November.)
By showing the water supply in subdistricts, and thus getting a more correct line of demarcation, I was able to point out that the advantage in favour of the population partly supplied with the purer water was even greater than Dr. Farr had indicated.†
(†On the Mode of Communication of Cholera, 2nd edit., p. 73.)
I had learnt from the evidence of Mr. Quick in the Health of Towns Reports, that the division of the houses, between the Lambeth Company on the one hand, and the Southwark and Vauxhall Company on the other, was not such as obtains in the north districts of London, where a parish is often divided between two water companies, but where one company always leaves off at the point at which the other begins. Throughout the greater part of Lambeth and Southwark, the whole of Newington, and a part of Camberwell, however, the supply of the two companies above mentioned is actually intermixed, the pipes of both companies going down the same streets, in consequence of the active competition which once existed between three water companies, two of which have since amalgamated and come to an agreement with the other--the Lambeth company. Observing, therefore, when the cholera returned in 1854, that there was the same advantage in favor of the districts partly supplied with water from Thames Ditton, I determined to make an inquiry, the idea of which I had previously entertained. It was obvious that, if the diminished mortality depended on the improved supply of water, the benefit of the whole diminution would be enjoyed by the inhabitants of houses having this supply, whilst the population receiving impure water would suffer as much as that of the districts which received the same water, and no other. This point could be determined by ascertaining the water supply of every house in which a fatal attack of cholera might occur. After commencing the inquiry I found that the circumstances were calculated for affording even more conclusive evidence than I had anticipated. The pipes of the two water companies not only passed down all the streets, but into nearly all the courts and alleys. A single house often had a different supply from that on either side. Each water company supplied alike both rich and poor, and thus there was a population of 300,000 persons, of various conditions and occupations, intimately mixed together, and divided into two groups by no other circumstance than the difference of water supply. One group supplied with water contaminated, to a large extent, with the sewage of London, and the other receiving a supply altogether free from such impurity.
I took great care to ascertain the nature of the water supply correctly in every instance. I did not rest content with the mere reply of the resident, or the appearance of the water, without other evidence, such as the production of the receipt for the water rate. I was also assisted very much by the application of a chemical test to the water, for throughout all the dry weather, which lasted whilst my inquiries were being made, a mixture of sea water extended further up the Thames than usual, and the water of the Southwark and Vauxhall Company contained nearly forty grains of common salt per gallon, whilst that of the Lambeth Company contained only .95 of a grain. These analyses were verified in numerous cases where the source of the water could be proved clearly by other evidence. For the first four weeks of the epidemic I employed the list of deaths from cholera published in the Weekly Returns of the Registrar-General, and for the next three weeks, during which my inquiry extended, I was kindly permitted to copy the addresses of persons dying of cholera at the General Register Office. My personal inquiry extended over every subdistrict to which the supply of the Lambeth Water Company extended, and it, therefore, included all the area in which the supply of the two companies was intermixed in the manner explained above.
At the time I was making my inquiry, the entire number of houses supplied by each water company was known, from a return made to Parliament, but the number of houses supplied in each district and subdistrict by each company respectively was not known. In order, therefore, to see the exact bearing of my results, I found it desirable to extend the inquiry over the districts supplied exclusively by the Southwark and Vauxhall Company; for this purpose I obtained the assistance of Mr. Whiting, a medical man, who took great pains with his part of the inquiry, which was merely to ascertain whether the houses in which fatal attacks had taken place were supplied by the Southwark Company, or from some other source, as a pump well or tidal ditch. His inquiry extended over the first four weeks of the epidemic.
I gave a copy of the first results of my inquiry to Dr. Farr, to whom I was indebted for facilities very kindly afforded: and Dr. Farr being much struck with these results, instituted a continuance of the inquiry through the district [242/243] registrars, who were requested to make a return of the supply of water to each house in which a fatal attack of cholera might occur in all the south districts of London. As the registrars could not be expected to make a chemical analysis of the water, or to seek out the landlord or agent in cases where the tenant was not acquainted with the water supply, the question remained unanswered in a considerable number of instances, but the return was obtained for more than three-fourths of the deaths, and shows, no doubt, the correct proportion. Dr. Farr's inquiry commenced from the 27th of August, and extended to the close of the epidemic; and as my inquiry extended to August 26th, the water supply was obtained for the whole epidemic of 1854. It was only necessary to make a computation of the small number of attacks occurring in houses supplied by pump wells or some other source, in the three weeks--the 5th to the 7th inclusive--of the epidemic, in Bermondsey and the other districts which do not receive the Lambeth water. This computation was made according to the result ascertained in the previous four weeks, and must approach very nearly the truth.
In treating of the general results of this inquiry, it is desirable to divide the epidemic into different periods, as the influence of the water supply was found to diminish in relative intensity as the epidemic progressed. In the first four weeks of the epidemic of 1854, that is, from July 9th to August 5th inclusive, there were 334 deaths from cholera in the districts to which the supply of the two water companies we are considering extends. The water supply in every one of these instances was made a matter of personal inquiry, and the result of each case was published by me in detail in the Appendix to a work on Cholera [that is, On the Mode of Communication of Cholera (1855)]. In 286 instances the supply of the house in which the attack took place was that of Southwark and Vauxhall Company; in 14 instances it was that of the Lambeth Company; in 4 cases the supply was from a pump well; in 26 cases the water was drawn direct from the river, or a canal, or a tidal ditch; and in 4 cases the supply could not be ascertained, owing to the address of the deceased persons, prior to the fatal attack, not being known. The number of houses supplied by the Southwark and Vauxhall Company was 40,046, having a population estimated by the Registrar-General* at 266,516, and the number of houses supplied by the Lambeth Company [243/244] was 26,107, with an estimated population of 173,748; the mortality from cholera was, therefore, at the rate of 107 to each 100,000 inhabitants supplied by the former company, and 8 to each 100,000 supplied by the latter; in other words, the disease was between thirteen and fourteen times as fatal to the population having the impure water as to that having the improved supply.
(*Weekly Returns for 1854, p. 433.)
It is particularly worthy of remark that, during the four weeks of the epidemic we are now considering, there were but 563 deaths from cholera in the whole metropolis, of which 286, or more than one-half, occurred amongst the customers of the Southwark and Vauxhall Company, who comprise a little more than one-tenth of London, and a considerable number of the remaining deaths took place amongst mariners, and others employed amongst the shipping, who almost invariably draw their drinking water directly from the river; it is, therefore, evident that at this early period of the epidemic the impure water of the Thames was almost the exclusive means of the propagation of the malady.
In the next three weeks of the epidemic there were 1,180 deaths from cholera in the districts supplied by the two water companies. Of these, the fatal attack took place in 977 cases in houses supplied by the Southwark and Vauxhall Company; in 84 cases in houses supplied by the Lambeth company; in 101 instances the supply was from some other source; and in 18 cases it could not be ascertained, for reasons previously stated. Taking into account the population supplied respectively by each company, the mortality was, at this period of the epidemic, nearly eight times as great in that supplied by the Southwark and Vauxhall Company as in that supplied by the Lambeth Company.
During the last ten weeks of the epidemic, from August 27th to November 4th inclusive, 3,564 deaths occurred in the districts to which the supply of the two water companies extends, and the returns of the district registrars showed that in 2,443 cases the water supply of the house in which the fatal attack took place was that of the Southwark and Vauxhall Company; in 313 cases it was that of the Lambeth Company; in 207 instances the supply was from pump wells and other sources independent of the two water companies, and in 601 instances the supply was not ascertained.† († Weekly Returns for 1854, pp. 514-18.) These numbers show a mortality of 916 to each 100,000 inhabitants supplied by the Southwark and Vauxhall Company, and 180 to each 100,000 supplied by the Lambeth Company; consequently at this period of the epidemic, the mortality was still more than five times as great amongst the population supplied by the former company as amongst that supplied by the latter.
The results of my inquiry into the supply of water were, of course, obtained separately for each district and subdistrict in which the inquiry was made, and were so published; but I was unable at the time to show the relation between the supply of houses in which fatal attacks took place, and the entire supply of each district and subdistrict, on account of the latter circumstance not being known. I expressed myself as follows in an article which I published soon after my inquiry was made: "I hope shortly to learn the number of houses in each subdistrict supplied by each of the water companies respectively, when the effect of the impure water in propagating cholera will be shown in a very striking manner, and with great detail."*
(*Medical Times and Gazette, Oct. 7, 1854, p. 365.)
This information did not, however, come within my reach till recently, and not even then with all the accuracy I could desire. In the Report on the Cholera Epidemics of London as affected by the Consumption of Impure Water, lately written by Mr. Simon, and published by the General Board of Health, there is a statement of the number of houses supplied by each of the water companies respectively in each district and subdistrict. The line has not been very accurately drawn where a street, as often happens, is partly in one district and partly in another; and thus, in the recent Report, the subdistricts of St. Saviour's, Southwark, Leather market, Bermondsey, Battersea, and Peckham, have been represented to contain a few houses supplied by the Lambeth Company although they do not contain any. With regard to Bermondsey, it is stated in a foot note that some ends of streets may have been included which have passed the registration boundary, and this has happened in other cases; but the errors arising from this cause are limited in amount, and cannot much affect the statistical calculations that I have made. There is also a further imperfection in the account of the water supply of the subdistricts. The numbers which are stated to represent the houses supplied by each water company in each subdistrict are found on adding up the tables not to do so, but to represent the number of houses, minus those situated in streets in which no death occurred; the latter being placed all together at the end of each group of subdistricts which constitutes a district. Streets vary in size from one or two houses to two or three hundred, and the small streets would obviously be the most likely to be exempt from mortality; it could, therefore, do little good to distinguish such streets; however, if thought desirable, this could as well have been done by simply stating the number of the houses, without deducting them from the gross number in each subdistrict. The number of houses in these exempted streets is about one-ninth of the whole. Instead of being able to compare, as I could wish, the mortality in the houses supplied by each company with the exact number of houses supplied, I have only been able to compare it with the number of houses in the streets in which deaths occurred. This will necessarily raise the proportion of deaths about one-ninth; but there is every reason to believe that the relative proportion of deaths in the population supplied by the two companies respectively, which is the real object of the inquiry, will remain almost unaltered.
As the first four weeks of the epidemic did not furnish a sufficient number of cases in all the subdistricts to serve for a statistical inquiry in detail, I have commenced by taking the first seven weeks of the epidemic collectively; and the first of the tables which accompanies this paper exhibits the results of my personal inquiry, when placed in connexion with the number of persons and houses supplied in each subdistrict by each water company respectively.*
(*The numbers of deaths in the third division of this Table and the next, are copied from page 85 of the work On the Mode of the Communication of Cholera.)
The reader will observe from the last division of the table that the proportion of deaths was, in every subdistrict, very much greater amongst the population supplied by the Southwark and Vauxhall Company than amongst that supplied by the Lambeth Company, and that the relative mortality is nearly the same throughout, except in two or three instances, where there were but one or two deaths for the basis of calculation amongst the customers of the Lambeth Company. The second table shows the results of that part of the inquiry conducted by Mr. Whiting, treated in a similar manner.
In the subdistricts here enumerated, which were supplied, except just on the border of three of them, exclusively by the Vauxhall Company, the mortality will be observed to be nearly the same, only a little higher, than [246/247] amongst the population supplied by the same company, and mixed with that supplied by the Lambeth Company, as shown in the previous table. In the third table the figures contained in the two first are collected into a more compact form, to show the result of the inquiry during the first part of the epidemic, arranged in districts.
The fourth table contains the results of that part of the inquiry made by Dr. Farr, when compared with the population supplied by each water company respectively.
It is necessarily arranged in districts--for the results were so published in the Weekly Returns--and not in subdistricts. (Loc. cit.) The mortality during the last ten weeks of the epidemic was greater than during the first seven weeks, but the reader will observe that a very great disproportion continues in every district between the mortality of the population supplied by one company and that supplied by the other. There is no district to which the supply of both companies extends in which the mortality is not more than three times as great amongst the persons supplied by the Southwark Company as amongst those supplied by the Lambeth Company, and the general result shows a proportion of ninety-one to eighteen, or more than five to one, as was stated before.
In the fifth table the numbers in the previous ones are added together, and fresh calculations made, so as to show the result of the inquiry for the whole epidemic.
The instances in which the water supply was not specified, or not ascertained, in the returns made by the district registrars must evidently nearly all have been cases in which the house was supplied by one or other of the water companies, for, if the persons received no such supply, and obtained water from a pump well, canal, or ditch, there could be no difficulty in knowing the fact. Moreover, as the two water companies are guided by precisely the same regulations, the difficulty in ascertaining the supply is exactly the same with regard to one as the other; I, therefore, concluded that I could not be wrong in dividing the non-ascertained cases between the two companies in the same proportion as those which were ascertained, and I have done so at the foot of table V, in order to obtain a complete view of the influence of the water supply during the whole epidemic of 1854. These general results I have employed as the basis of some further calculations.
In table VI[,] I have copied from the Weekly Returns of the Registrar-General the mortality from cholera in every subdistrict to which the supply of both, or either, of the water companies extends.
I have also calculated the number of deaths which would have taken place in each subdistrict according to the number of persons supplied with water by each company respectively, and in accordance with the mortality ascertained for the whole of the population supplied; and it will be observed that the calculated mortality bears a very close relation to the real mortality in each subdistrict. This relation exists with regard both to the gross mortality and to the mortality to each 10,000 living, all through the table, and proves the overwhelming influence which the nature of the water supply exerted over the mortality, overbearing every other circumstance which could be expected to affect the progress of the epidemic. Thus, in the crowded, dirty, and very poor subdistricts of Lambeth Church, first part, and Waterloo, first part, lying by the river side, the mortality was low in consequence of the water supply being chiefly that of the Lambeth Company; whilst in the thinly peopled, and comparatively genteel subdistricts of Clapham and Battersea the mortality was very high, in consequence of the impure water of the Southwark and Vauxhall Company. Taking this inquiry altogether, and considering that the results which were published two years ago, and could only be estimated collectively, are now corroborated in detail through upwards of thirty subdistricts, it probably supplies a greater amount of statistical evidence than was ever brought to bear on a medical subject.
At the latter part of 1854, the General [B]oard of Health procured from the two water companies, by order of the Secretary of State, a list of all the houses which they supplied, which lists are very valuable, as affording the means of ascertaining the exact water supply of each district and subdistrict separately. By direction of the Scientific Committee of the Board of Health, the lists have been employed in making a supplemental inquiry into the effect of the water supply on cholora. For this purpose they were compared with the lists of deaths at the General Registrar Office, and the results have been embodied in the recent Report of Mr. Simon, previously referred to. There are, however, certain circumstances, which were probably unknown to the Scientific Committee, and which render it impossible that an inquiry, conducted in this manner, could do more than approximate to the truth; and show why it can bear no comparison in point of accuracy to a personal inquiry, made on the spot, at the time of the epidemic. In the first place, throughout the greater part of Lambeth, Newington, and the Borough, the houses are either without numbers, or numbered very irregularly, and the numbers are liable to frequent change, as new houses are built, or older ones repainted; there are also frequently repetitions of the same number in the same street, and although, in some instances, the companies have returned the names of the occupiers, that can be of no assistance in the case of the poor, who occupy but one or two rooms, and form the greater bulk of the population. In the next place, the poor often furnish, unintentionally, a wrong number to the registrar, even when the houses are regularly numbered. They know their own homes perfectly, but, having no occasion to refer to the number, they partially forget it; and, in the greater number of my personal inquiries, I had to call at two or three houses before I found the one in which the death occurred. For these reasons it follows that, in comparing the lists of the water supply with the lists of deaths, many errors must have occurred; and as the deaths were six times as numerous in the houses supplied by the Southwark and Vauxhall Company as in those supplied by the Lambeth Company, the evident result would be that out of every six mistakes five would transfer a death from the former company to the latter and only one would transfer a death from the latter company to the former. Another source of error, but operating to a less extent, is, that a number of persons who were attacked with cholera in houses supplied by the Southwark Company died in the workhouses of St. Saviour's, Lambeth, and Newington, which were supplied by the Lambeth Company. It need excite no surprise, therefore, that the supplemental inquiry, embodied in the recent Report, instead of showing a mortality of 160 and 27 for the population supplied by the two water companies, or a difference of 6 to 1, showed a mortality of 125 and 37 per 10,000, or a difference of only 3½ to 1. It must be obvious, however, independently of the above facts, that a difference of three and a-half to one would not explain the great difference in the mortality of the various districts and subdistricts. The epidemic of 1853 is included with that of 1854 in Mr. Simon's Report; but as there were but few deaths in 1853, and those chiefly amongst the population supplied by the Southwark Company, this circumstance would not much affect his results.
It is probable that, when the facts brought to light by this inquiry are sufficiently known, no one will deny the influence of impure water in promoting the mortality of cholera; but it must not be supposed that it is mere impurity of an ordinary kind that causes the disease, for there are innumerable facts to prove that ordinary impurities have no such effect, and that it is only when the specific morbid matter of the disease gains access to the water that cholera is propagated. Thousands of people drank water from their own neglected cisterns, during the late epidemic, as impure as that of the Southwark and Vauxhall Company without ill effect. An inquiry made by the vestry of St. James', Westminster, proved that the contents of a cesspool had been percolating for months through the three feet of earth which separated it from the pump well, in Broad Street; but although hundreds of people were daily drinking the water, and cholera was extending fearfully in many parts of London, only a few scattered cases occurred in the streets near the pump till the end of August, when, a case having happened amongst the persons using the privy connected with the cesspool above mentioned, more than five hundred persons were attacked within two or three days.
In the cases in which the cholera poison gains access to a limited supply of drinking water, such as a tank or pump-well, the outbreak it occasions is always sudden, violent, and limited; but when a river is the medium of the propagation of the disease, its progress is more gradual and extended, being diffused amongst the whole population using the water.
It is hardly necessary to remark, that every circumstance which proves the communication of cholera through the medium of water, corroborates the views, explained at the beginning of this paper, regarding its propagation in the crowded houses of the poor; for it cannot be supposed that morbid matter, which can produce its specific effects after being diffused and distributed through a quantity of water, could fail to act in an undiluted state.
It was my intention to make some remarks on the drainage and water supply of towns, but this communication has already exceeded the limits which I prescribed for it.
Sackville Street.
Return to John Snow Publications
108. "On the vapour of amylene, Part 1"
Source: Snow, John. Medical Times and Gazette 14, 17 January 1857, pp. 60-62. Part 1
By John Snow, M.D.
We are indebted for the agents which have hitherto been inhaled for the prevention of pain rather to a number of accidental circumstances, than to any systematic and well-regulated investigation. In the course of his experiments on nitrous oxide gas, Sir Humphrey Davy found that severe pain arising from inflammation of his gums was relieved by breathing it, and he published the following opinion in the first year of the present century:--"As nitrous oxide in its extensive operation seems capable of destroying physical pain, it may, probably, be used with advantage during surgical operations in which no great effusion of blood takes place."*
(*Researches concerning Nitrous Oxide, p. 556.)
This sentence was read by hundreds, and listened to at public lectures by thousands, for the period of forty-four years, without any result, when the late Mr. Horace Wells, a dentist of Hartford, Connecticut, being present at a lecture by a Mr. Colston, was induced to request the lecturer to accompany him to his office, and to exhibit the gas to him, while another dentist, named Dr. Riggs, extracted a tooth which was troublesome. The tooth was extracted without pain, and Mr. Wells, after the effect of the gas had subsided, exclaimed, "A new era in tooth-pulling!" Mr. Wells administered the nitrous oxide in thirteen or fourteen cases of tooth-drawing, in Hartford, with a success more or less complete; and before the end of the year he repaired to Boston, to introduce his discovery to the Professors at the Massachusetts General Hospital. For want of a more important operation, the gas was tried in a case of tooth-drawing. The patient felt some pain, and the application was considered to be a failure. Mr. Wells returned to Hartford in disappointment. He expressed his opinion to his friends that nitrous oxide gas was uncertain in its effects, and not to be relied on; and he altogether abandoned the use of it until some time after Dr. Morton's discovery of the effects of sulphuric ether in preventing pain.
Ever since 1818 the vapour of ether had been known to produce exhilarating effects, similar to those of the laughing gas. The circumstance was mentioned in nearly all the standard works on Chemistry; and it was the practice for the Medical Students in many of the Colleges, both in England and America, to inhale ether on the day of the lecture on that medicine. Dr. Morton, a dentist of Boston, had been formerly in partnership with Mr. Horace Wells, and had been [60/61] present at his unsuccessful attempt to apply the nitrous oxide in the Hospital. On September 30, 1846, Dr. Morton administered the vapour of sulphuric ether successfully in a case of tooth-drawing, and shortly afterwards he administered it with success in some Surgical operations in the Massachusetts General Hospital. He thus established the power of sulphuric ether to prevent pain in the very institution where Mr. Horace Wells had failed in his attempt to introduce the nitrous oxide. Dr. Morton had apparently received some information respecting ether from Dr. Charles Jackson, Professor of Chemistry, but to Morton the merit is entirely due of introducing the practice of preventing the pain of Surgical operations. This is certainly true of modern times, and, probably, of all times to which history extends; for I believe that the use of mandrake by the Greeks and Romans, and of Indian hemp by the Chinese, must have been attended only with slight success in Surgical operations. I need hardly remind the Society that the inhalation of ether was soon extended to the prevention of pain in obstetric cases and a number of diseases, as well as in Surgical operations.
A medicine called chloric ether has been in use since 1831. It was first applied by inhalation with success in preventing pain by Mr. Jacob Bell, of London, early in 1847; and it was exhibited afterwards with occasional success in St. Bartholomew's and the Middlesex Hospitals, and in the private practice of Mr. Lawrence. This miscalled chloric ether is a solution of chloroform in spirit, and the insensibility it occasions when inhaled is entirely due to the chloroform, of which it contains about twelve per cent. Mr. Waldic, of Liverpool, being in Edinburgh in the autumn of 1847, explained these circumstances to Dr. Simpson, who had been the first to apply inhalation in the practice of midwifery, and was at the time paying great attention to the subject of anæsthesia. Dr. Simpson procured the chloroform in its undiluted state, and was the first to exhibit it in this condition, and the public and the Profession are indebted to him for its introduction to general use. Chloroform was immediately adopted, to the almost entire exclusion of ether, and has continued to keep its place, with a few exceptions, to the present time. At the Massachusetts General Hospital the use of chloroform was prohibited by the governors three or four years ago, on account of two accidents; and sulphuric ether has since been used, to the entire exclusion of chloroform. Ether is the agent employed in private practice in the town of Boston; and I have been informed that this is the case at Philadelphia, and in Europe, at Naples and Lyons.
Ever since the introduction of chloroform I have been of opinion that other agents would be met with more eligible for causing anæsthesia by inhalation. It seemed improbable that this one, which happened to be standing on the shelf of the Pharmaceutical Chemist for another purpose, should be better than all the very numerous volatile compounds which organic chemistry is daily bringing to light; and the continued use of chloroform is probably due to the circumstance, that hardly any one has made anæsthesia by inhalation a subject of constant and protracted investigation. I have from time to time made experiments on animals with a variety of substances, and I find that the agents which might be inhaled for the prevention of pain, in the absence of others which are more eligible, are extremely numerous. They include, among other things, carbonic acid and carbonic oxide gas, olefiant gas, the vapour of hydrocyanic acid and cyanogen gas, which last is contained, as I found, in the fumes of the puff-ball, which Dr. Richardson brought before the notice of this Society. The agents which I have exhibited as anæsthetics to the human subject, in addition to ether and chloroform, have as yet been but few. They are nitric ether, Dutch liquid, benzin or benzole, a bichloride of carbon, made by decomposing chloroform with chlorine gas, the monochlorinetted chloride of ethyle, and amylene, the subject of this paper. Nitric ether was exhibited also by Dr. Simpson, and Dutch liquid by him and Mr. Nenneley. These substances possess no advantage over chloroform, unless it be their slower action, while in other respects they are scarcely so agreeable. With regard to benzin, I discontinued the use it on account of convulsive tremors which it occasioned in a case of amputation in St. George's Hospital. I found that these tremors are a constant result when its effects reach a certain stage. I administered the chlorinetted muriatic ether in twenty surgical operations, in the summer of 1851, chiefly in King's College Hospital. Its sensible and physical properties and its effects are nearly the same as those of chloroform, but I thought that it might possess some advantage in the circumstance that, being less volatile, while its other properties are the same, it would be less liable to cause accident, even if incautiously used. I was, however, prevented from using it further, owing to the great difficulty of procuring it in a state of purity.
Amylene was discovered and described in 1844 by M. Balard, Professor of Chemistry to the Faculty of Science of Paris.*
(*Annales de Chimie et de Physiqueem, 3me Serie, tom. xii. p. 320.)
It is made by distilling fusel oil with chloride of zinc. M. Auguste Cahours had given this name five years previously to a product which is isomeric with amylene, and is made in nearly the same manner, but is now termed paramylene. Amylene itself is a colourless and very mobile liquid, of extremely low specific gravity. M. Balard has not stated the specific gravity in his essay, but I found that of the amylene made for me by Mr. Bullock,† and which is extremely pure, to be 0.659 at 56°. It is very volatile, boiling at 102º Fahr., and the specific gravity of its vapour is 2.45. It is composed of ten atoms carbon, and ten atoms hydrogen, and it bears the same relation to fusel oil, or amylic alcohol, that olefiant gas, or ethylene, bears to common alcohol. It burns with a brilliant white flame. It is soluble in alcohol and ether in all proportions, but is very sparingly soluble in water, being in fact a hundred times less soluble than many substances which are usually said to be insoluble in water. I have not yet been able to determine its solubility so exactly as I could wish, but as nearly as I can ascertain, 100 volumes of water dissolve two volumes of the vapour, at which rate one part of liquid amylene would require 10,220 parts of water for its solution. It has an odour somewhat resembling that of naphtha; some persons think the odour rather agreeable, and others think it somewhat unpleasant; the odour is not so strong or permanent as that of sulphuric ether, and does not remain long in the patients' breath. The vapour of amylene is much less pungent than those of ether and chloroform. It is therefore easier to breathe, and does not cause the choking feeling which sensitive and nervous patients often complain of in breathing chloroform. It has not caused any coughing to signify, except in two patients who were suffering from cattarrh, and in these cases the cough subsided in a minute or two.
(†[of] 15, Hanover-street, Hanover-square)
I was not aware of the existence of amylene till a few months ago, or I should have tried it sooner; for I made inquiry in 1848 for a substance named eupion by Reichenbach, its discoverer, but was unable to obtain it. Eupion is a carbo-hydrogen, described as having all the physical characters which belong to amylene, though obtained in a different way; and I believe it is the same substance. Reichenbach obtained it from coal tar, but other chemists have not been able to make it.
Judging from experiments which I had made on analogous substances, there could be no doubt of amylene causing insensibility when inhaled; but I could not tell, without actual trial, whether it might not be too powerful, or otherwise unpleasant in its action. I made a number of experiments in 1848,‡ from which it appeared that each definite degree of narcotism was occasioned by an amount of the narcotic agent, bearing a certain relation to the whole amount which the blood is capable of dissolving, and that this relation was nearly the same in regard to ether, chloroform, and several allied substances. For instance, a very complete state of insensibility, which I named the fourth degree of narcotism, was caused by the presence in the blood of 1-28th part as much chloroform as it was capable of dissolving; and that the same state of insensibility was also occasioned by 1-28th part as much ether as the serum of the blood was capable of dissolving. The same relative amount of nitric ether produced the same degree of narcotism. In the case of bromoform and of bromide of ethyle, it was 1-27th part, with Dutch liquid it was 1-25th part, and with bisulphuret of carbon it required one part in 31 of what the blood was capable of dissolving, to induce the fourth degree of narcotism. Benzin was the only agent among those which I examined at that time which offered any great deviation from the others in the relative amount of its vapour which was required to be absorbed, in order to induce a definite degree of narcotism. To induce the fourth degree of narcotism by benzin it required 1-17th part as much as the blood is capable of dissolving. Now, benzin bears a great resemblance to amylene, being, like it, a carbo-hydrogen, the composition, however, being different.
(‡See Medical Gazette, Vol. II., 1848, "On Narcotism by the Inhalation of Vapours.")
The amount of amylene which requires to be absorbed is far greater in relation to the quantity which the blood would dissolve than in the case of benzin. I found, from some experiments which I made on guinea-pigs, mice, and linnets, that to cause the fourth degree of narcotism requires about 1-5th part as much amylene as the blood would absorb, to cause the second degree 1-10th part as much, and to cause the third degree, which is as far as I have carried its effect in the human subject, it requires an intermediate portion, or about 15 per cent. I found, for instance, that to induce the fourth degree of narcotism in a guinea-pig, it required that the air in the jar in which it was enclosed must contain 20 per cent, or a fifth part of its volume of the vapour of amylene. The temperature of the guinea-pig is, however, just that of the boiling point of amylene, when the tension of its vapour balances the weight of the atmosphere; and, consequently, the blood passing through the lungs could not take up, in the above experiment, more than 1-5th as much as the whole quantity which it could dissolve. This is a point capable of direct proof. The entire quantity of amylene which is absorbed during inhalation must, however, be extremely small, owing to its very sparing solubility. Taking the solubility of amylene in watery fluids to be what I have state above, viz., 1 part in 10,220, and taking the quantity of serum of the blood in the human adult to average 410 fluid ounces, as estimated by Valentin, then the amount of amylene circulating in the body in the third degree of narcotism would be not quite 3 minims. The above calculation of the small quantity absorbed into the blood is confirmed by some other experiments which I made. I introduced 14 minims of it into a bladder with 200 cubic inches of air, and after breathing it backward and forward a few times I became very nearly unconscious, and experienced, in fact, more effect from these 14 minims than from 45 minims breathed to and from a large bladder, holding 670 cubic inches.
Viewed in the light of the small quantity which requires to be absorbed into the system to cause insensibility, amylene is a very powerful agent; but when considered in relation to the quantity which is consumed during inhalation in the ordinary way, it is far from being powerful. This arises from the great tension and the small solubility of the vapour, in consequence of which it is, with the exception of a small fraction, expelled from the lungs again without being absorbed. In this respect it resembles, to a great extent, the nitrogen gas of the atmosphere, with which the lungs are always four-fifths filled, while the blood contains but a few cubic inches. It takes from three to four fluid drachms of amylene to cause insensibility in the adult, while less than a drachm of chloroform is usually sufficient. The quantity of sulphuric ether required to cause insensibility in the adult is eight to ten fluid drachms, one-half of which is absorbed into the blood. In a protracted operation of half-an-hour or upwards, the quantity of amylene used is greater even than that of sulphuric ether; the small quantity of the former which is absorbed is quickly exhaled again from the lungs, and has to be constantly replaced; while the large amount of sulphuric ether, when once absorbed, takes a much longer time to exhale in the breath. This constitutes some objection to the use of amylene in protracted operations, as it adds to the expense.
[Part 2 appeared in the issue of 24 January.]
Return to John Snow Publications
109. "On the vapour of amylene, Part 2"
Source: Snow, John. Medical Times and Gazette 14, 24 January 1857, pp. 82-84. Part 2
By John Snow, M.D.
Part 2
It follows from the experiments above alluded to that the patient must breathe air containing not less than fifteen per cent of vapour of amylene, in order to reach the third degree of narcotism, or that condition in which the pupils are usually contracted and inclined upwards, consciousness and voluntary motion being entirely suspended, but the muscular system not necessarily relaxed. As 100 minims of amylene produce 86.7 cubic inches of air a minute, and frequently more, the amylene is consumed at the rate of rather more than a fluid drachm in the minute, and in this way insensibility is caused in three minutes, or rather less. If the vapour is not inhaled in a sufficient volume the patient will not become insensible by continuing the inhalation for however long a time, consequently the quantity of vapour must be increased, or it will not succeed.
The amount of vapour of amylene that the air will take up at ordinary temperature is far more than enough to cause insensibility, even when but partially saturated. When fully saturated the quantity of vapour at different temperatures is nearly the same as in the case of sulphuric ether, a table of which I laid before the Society in 1847. At the following temperatures I find that air, when saturated with vapour of amylene, contains the subjoined quantities in each 100 cubic inches, when the barometric pressure is 30 inches:--
In the ordinary process of inhalation, however, it is not easy to get the air even half saturated with vapour, owing chiefly to the cold produced by the evaporation of the amylene. When a piece of blotting-paper is wetted with amylene it usually happens that the absorption of caloric by the evaporation causes, first, a deposition of the moisture of the atmosphere, and then the freezing of the water, so as to occasion the appearance of hoar frost on the paper. This extreme cold would, of course, limit the evaporation very much, but it is counteracted in a great measure by the bath of cold water which surrounds my ordinary chloroform inhaler, the water supplying the caloric which is abstracted by the vapour of amylene; and since using this latter agent I have had the apparatus somewhat enlarged, in order to afford a larger surface of bibulous paper, and a somewhat greater quantity of water; by this means I find that I have the power to exhibit a sufficient volume of vapour, even in this weather, when the temperature of the water, although kept in a dwelling-room, is often as low as 50?.*
(*The inhaler is made by Matthews, Portugal-street.)
After making several experiments on small animals with amylene, and inhaling small quantities of it myself, I first administered it in King's College Hospital, on the 10th of November last, to two boys about 14 years old, previous to Mr. Samuel Cartwright extracting some teeth. I had but a few drachms, and being very sparing of its use, it did not entirely remove consciousness in either case, and the pain was not altogether prevented; the effects, however, as far as they extended, were so favourable as to encourage a further trial, which was made in the same institution on December 4.
On this occasion I exhibited the amylene to four patients--two men, a young women, and a girl of 10 years old; it occasioned complete unconsciousness and absence of pain in each case. Each of the men inhaled for three minutes, and used half a fluid ounce of amylene; they each had a tooth extracted by Mr. Cartwright, and awoke and left feeling quite well, just six minutes after entering the room. The two females inhaled for four minutes; the elder one, who was not in good health, complained of dizziness afterwards, which, however, passed off in about ten minutes. On December 11, I exhibited the amylene again in five more cases of tooth-drawing in King's College Hospital, with very similar results to those obtained in the previous cases; and on December 13, I administered it in some more important operations.
In one case Mr. Fergusson performed an operation for fungus of the testicle; Mr. Bowman removed some diseased glands from the groin; and there were two cases of tenotomy, in one of which forcible extension of the knee was made.†
(†See Med. Times and Gazette, Dec. 20, p. 624.)
On December 27, I exhibited the amylene again to a girl three years and a half old, a patient of Mr. Fergusson, who had inhaled it on the 13th; the effects were the same; she inhaled for two minutes before the operation was commenced; there was no sign of pain, and she awoke almost the moment the operation, which consisted in the division of some additional tendons near the foot, was concluded. On January 3rd, I administered amylene again in three operations performed by Mr. Fergusson. One of these was an operation for the completion of a new nose. There was a little delay, owing to the difficulty of fitting the face-piece to the new organ; and the man inhaled for six minutes before the operation was commenced, but half this time he was making no progress towards anæsthesia. There was much less rigidity and struggling than when he inhaled chloroform a few weeks previously. After the operation was commenced the vapour was exhibited on a sponge as well as circumstances would permit, and, although the patient flinched a little once or twice, the anæsthesia was as complete as is usual in such cases; for there is generally some difficulty in keeping up the insensibility during operations on the face. At one part of the operation the man entered into a rambling conversation, which had no connexion with the use of the knife, of which he seemed entirely unconscious.
On the 7th inst., I gave the amylene whilst Mr. Henry Lee performed amputation above the knee in a girl who underwent excision of the knee-joint a few weeks ago. She had suffered from secondary abscess, was extremely week, and had a pulse of 150 in the minute. The vapour was exhibited to the patient in bed, before her removal to the operating table. There was an examination of the knee before the operation, and the anæsthesia was kept up till the dressings were applied, which was twenty-five minutes from its commencement, and nearly three fluid ounces of amylene were used. She went through the operation extremely well. There was no sign of pain, and the pulse remained the same throughout.
I have again given the amylene today in three operations performed by Mr. Fergusson in the Hospital. The first was an operation by ligatures on a large nævus of the lip in a young man; the next was lithotomy in a child about three years old; and the third was the removal of a large melanotic tumour from the groin of a middle-aged man. The patients were each brought under the influence of the vapour in from two to three minutes. The prevention of pain was complete in all, and the two men were partially conscious during a great part of the operation, the last patient repeating a number of verses with perfect accuracy while the vessels were being tied. These make twenty-one operations in which I have administered amylene.
In the use of amylene absence of pain has been obtained with less profound coma than usually accompanies the employment of chloroform and ether. There are some cases, indeed, in which the minor parts of an operation, under these latter agents, may be performed without pain while the patient is in a semi-conscious state, or even altogether conscious, but they form an exception; while in the use of amylene the patient has very often been half-conscious during the operation. In operations under chloroform the patients usually indicate the necessity of repeating the inhalation by a tendency to flinch or cry, without showing any signs of consciousness; but in the use of amylene they have more frequently begun to look about and to speak before showing any sign of pain. There are some patients who will not lie still under the Surgeon's knife while chloroform is being used, unless its effects are carried so far that the breathing is on the borders of being stertorous, but I have not yet met with any such case in using amylene.
I made the observation early in the practice of inhalation for the prevention of pain, that the anæsthesia, or loss of common sensibility, does not always keep pace with the amount of narcotism of the nervous centres, as evinced by coma, etc., even in the same case; and I offered an explanation of the circumstance to this Society* in the fact that narcotic vapours act on the nerves throughout the body, as well as on the brain; and there were certain circumstances connected with the circulation, why at one time, or in one case, the brain, and at another time, or in another case, the nerves should be most influenced. I have not at present, however, arrived at any conclusion as to the reason why amylene prevents pain with apparently a less amount of coma than ether and chloroform.
(*See Medical Gazette, 1848, Vol. II.)
The pulse is generally increased in frequency and force during the inhalation of amylene to a greater extent than happens with chloroform. There has generally been an increased redness of the face during the first part of the inhalation, and in one case there was profuse sweating, a phenomenon also met with, now and then, under the influence of chloroform.
The respiration is very often accelerated during the inhalation of amylene, about as often, I think, as with ether, and more frequently than with chloroform. Dr. Sibson and I found that the breathing was greatly accelerated by these latter agents in a dog, after he had divided both the pneumogastric nerves, so that the phenomenon is not occasioned by the local effect of the vapour in the lungs.
There has not been much increase of saliva from the use of amylene, and I have not yet met with the profuse salivation which is often troublesome in the employment of chloroform and ether. What is of most importance of all, however, if it should continue, is, that there has been no sickness in any case, nor any of the depression which so often precedes and accompanies the sickness from chloroform and ether.
There has been hardly any struggling or rigidity in any of the patients, although several of them being robust men, a good deal of both might have been expected before complete insensibility, if chloroform had been the agent employed.
A point of great interest connected with amylene is its probable safety or danger. While I cannot venture to predict for it the absolute safety which seems to attend sulphuric ether under all circumstances, I confidently trust that it will be perfectly safe with careful management. Although the use of ether was commenced when there was no experience in the production of insensibility by inhalation, yet there seems to have been no fatal accident from its effects during its very extensive employment. It has, indeed, been alleged that it has proved fatal in two instances; but in one of these cases, which occurred at the Hôtel Dieu of Auxerre in July, 1847, the patient probably died from want of air, owing to a defective apparatus; the inhalation was persevered in for ten minutes, although there were alarming symptoms the greater part of the time. The other case happened at the Hôtel Dieu of Lyons, on August 26th, 1852. M. Barrier was removing the superior maxilla, affected with osteo-sarcoma, in a woman in a bad state of health, who was seated in an easy chair. She died of sudden syncope in the middle of the operation, a result which occurred in a similar operation by an eminent Surgeon in this metropolis before ether was introduced. From the history of the inhalation and of the symptoms, I feel sure that the loss of blood was the cause of death, and not the ether. There have, however, been several sudden and fatal accidents in the use of chloroform; and although they are extremely few in comparison with the multitude of cases in which this agent has been used, they are, nevertheless, much to be regretted.
I have on former occasions explained the reasons why accidents have happened in the use of chloroform, and not in the use of sulphuric ether, and I will now very briefly recapitulate these reasons. The quantity of ether which a patient requires to inhale in order to be made insensible occupies about 400 cubic inches in the form of vapour, and necessarily mixes in the process of inhalation with not less than 800 cubic inches of air, and makes a volume of at least 1200 cubic inches, which can only be inhaled by a number of inspirations; and no great proportion of the whole quantity can ever be in the lungs at one time. The quantity of chloroform, on the other hand, which when inhaled will cause insensibility in the adult is only about 36 minims, which occupies only a little more than a pint in the form of vapour, and this, if precautions be not taken to prevent it, may be mixed in the process of inhalation with less than a gallon of air, which may all be inhaled in a few inspirations, and a great proportion of it might be in the lungs at one time. For the above reasons ether cannot produce its effects except gradually, whilst chloroform is capable of acting almost instantaneously, when the point of safety may easily be overstepped. Chloroform, ether, and similar agents have the power, when pushed to excess, not only of arresting the respiratory movements, but of stopping the action of the heart by their direct physiological effects. It takes, however, a larger quantity to paralyse the heart than to suspend the action of the respiratory muscles; and as ether can only enter the circulation by degrees in the process of inhalation, it is necessary to open the pericardium and blow the vapour on the surface of the heart, or to perform some other manaeuvre in order to show the direct action on the heart. When animals are made to breathe ether till they die, the action of the heart continues after the ordinary breathing has ceased; and, at the moment when the action of the heart is stopping from over distension, there are generally two or three deep gasping inspirations, which set about the recovery of the creatures, unless they are made to breathe more ether during these gasps. These are also the phenomena which occur in killing animals with chloroform, if care be taken to have the vapour so diluted that the air they breathe does not contain more than five per cent of it. But when the air breathed contains eight or ten per cent of vapour of chloroform it acts so quickly, and is absorbed in such quantity into the blood as it passes through the lungs, that not only are the brain and nerves of respiration narcotised, but also the nerves of the heart, and the animal is beyond recovery. The above facts explain, in my opinion, both the great safety of ether, under all ordinary circumstances, and the great care required with chloroform to ensure its safety.
The quantity of amylene which the patient requires to inhale to cause insensibility is intermediate, as stated above, between that of chloroform and that of ether, and so also is the amount of air which must be mixed with it; and it is my opinion that the cold produced during its evaporation would, in all the ordinary methods of inhalation, prevent the air from taking up a quantity of the vapour which would be dangerous.
The relative advantages and disadvantages of amylene may, as nearly as I can judge, be summed up as follow:--In regard to its odour, it is more objectionable than chloroform, but much less so than sulphuric ether. The odour of any volatile substance is, however, no longer perceived after a patient begins to inhale. In respect to its pungency, it has a great advantage over both ether and chloroform, being much less pungent than either of them. Thus, whilst the patient, especially if a female, often complains of a choking feeling and want of breath in commencing to inhale chloroform, and two or thee minutes are lost before the vapour can be inhaled in any useful quantity, she can begin to inhale the amylene of full strength within half a minute from commencing, and the operation may generally be begun within three minutes. In the amount which suffices to induce insensibility it is intermediate between chloroform and ether, chloroform having the advantage. Amylene has the advantage in preventing pain with a less profound stupor than that occasioned by the other agents, and in the ready waking and recovery of the patient it has an advantage over chloroform, and a still greater advantage over ether. Its probable safety I have spoken of; and the greatest advantage of all, if it should continue to be met with in all cases, is the absence of sickness from its use. The almost entire absence of struggling and rigidity may also be mentioned as an advantage of amylene over ether and chloroform.
I do not venture to predict that amylene will supersede the use of other agents, but I trust that the subject in its present stage is sufficiently interesting to warrant me in bringing it before the notice of the Profession, and I consider that the results obtained with the amylene have been so satisfactory as to encourage the further use of it. It would probably become cheap if there should be a demand for it.
Sackville-street.
Return to John Snow Publications
110. "On the recent accident from chloroform"
Source: Snow, John. Medical Times and Gazette 14, 21 March 1857, pp. 282-83.
By John Snow, M.D.
In the case recorded by Mr. Paget, in the Medical Times and Gazette of the 7th inst., the symptoms were observed with unusual care, and described with great clearness; hence the case is one of more than ordinary value, as illustrating the manner in which accidents from chloroform occur. The symptoms in this case were so clear and well marked that they would almost enable us to come to a correct conclusion as to the death if we had no set of exact and systematic experiments on the subject. The chloroform at the moment of the accident was given so as not to interfere with free respiration; the boy had as much air as he could breathe, and did in fact take a long inspiration just when the accident occurred. There was, however, every facility for the air which the patient breathed to be highly charged with vapour of chloroform, as it passed over the lint and cotton wool held half an inch from the face. The effect of the chloroform taken into the lungs by the long inspiration just mentioned was most marked on the action of the heart. According to Mr. Paget's account the pulse, which "had to this time been normal, suddenly began to beat very quickly; then it ceased for two or three seconds; then beat rapidly several times with a kind of flickering movement, and then ceased to be perceptible." Whilst the heart was thus paralysed by the chloroform the brain was not seriously affected by it, for after a few stertorous breathings he breathed naturally for at least a minute, when the respiration began to fail from the want of circulation of blood through the brain.
So much is suggested by a mere reflection on this case, but when it is compared with experiments and observations that I have made on animals there can no longer be any doubt as to the exact cause of death; and I should like to observe that as chloroform produces precisely the same effect on the smaller domestic animals as we daily witness in man, up to a state of complete insensibility, it is very evident that when they are killed by it in such a way that their death resembles exactly the sudden accidents which have happened occasionally to the human species, the cause of death and the conditions under which it occurs must be the same. The strength of the vapour of chloroform which I find most suitable for causing insensibility in patients is about four volumes in one hundred volumes of air; and I ascertained by experiments which I performed some years ago that when animals are made to breathe the vapour of this strength till they are killed, death takes place very slowly, the insensibility becomes very profound, with complete relaxation of the voluntary muscles, the breathing becomes embarrassed or very feeble before it ceases, and after it has ceased the heart continues to beat distinctly for a minute or longer, during which interval the creature can easily be restored by artificial respiration. I found, moreover, that at the moment when the heart ceases to beat from over-distention of its right cavities, there is often a deep gasping inspiration, which frequently has the effect of setting about the recovery of the animal if the vapour have been withdrawn.
On the other hand, I ascertained that when animals are made to breathe vapour of chloroform of twice the usual strength or more, that is, of eight or ten parts to one hundred of air, the death is very sudden, taking place in some cases even before insensibility has been induced, and the heart ceases to act, either at the same time as the respiration or before it. These are two distinct modes in which death takes place from chloroform, although with vapour of intermediate strength one mode of dying may more or less encroach on the other.
There is no recorded case of accident from chloroform in the hands of a medical man where the death took place in the first of the above-mentioned modes, as it would do if vapour of the proper strength were continued too long, in the disregard or misconception of gradually approaching dangerous symptoms; in all the recorded cases the death, or at least the fatal symptoms, set in suddenly, generally almost instantaneously, and, in the cases where the pulse was not observed, the sudden pallor or stoppage of bleeding sufficiently indicated that the circulation was arrested. Omitting two cases of fatal syncope, apparently from fear, which have sometimes been attributed to chloroform, there seems to have been ample opportunity in every instance for the vapour to be inhaled in too strong a form, and the result shows that this must have been the case.
In some of the recorded cases of deaths from chloroform the last beat of the pulse was a good as those which preceded it, but more frequently it has been noticed to become very weak just before it ceased. In Mr. Paget's case it beat very rapidly several times, and intermitted for two or three seconds before it finally ceased. In the numerous instances in which I have killed animals quickly with air strongly charged with chloroform, I have generally found the action of the heart to become weak just before it ceased, and in two or three cases, of which I have notes, it beat with extreme rapidity when its action was just on the point of ceasing.
The case under consideration supplies a clear refutation of two of the most serious and prevalent errors respecting chloroform. The first of these is that the patient is safe so long as he has sufficient air for the purposes of respiration; and the second, that close attention to the pulse and the general condition of the patient may of themselves avert danger. Both these rules are right enough, but the present case proves that they will not of themselves avert danger. Indeed the more air the patient breathes the greater is his danger, if the air be too highly charged with the vapour of chloroform; and I have often had occasion to point out the risk arising from a deep inspiration, such as occurred in this case, if the air should contain too much of the vapour. No case could apparently have been more carefully watched than the one under consideration; but the truth is that the first rule to be observed in giving chloroform, is to have the vapour so diluted that it cannot occasion sudden death, and the second rule is, to closely watch every symptom in the patient, so that one may leave off at the right moment, and not produce an unnecessary amount of oppression of the brain, with stertorous or embarrassed breathing.
Mr. Paget says that the quantity of chloroform poured on the cotton wool just before the accident was about forty drops. He probably means a quantity equal to about forty minims, as forty drops of chloroform from a small phial are not quite equal to nine minims; and although that portion of the inhaled chloroform which, by circulating through the coronary arteries, paralyses the heart and causes a sudden accident, must be extremely small, it is not likely that sudden death would occur unless the vapour of several minims of chloroform were to gain access to the lungs in a short time, so as to impregnate the blood passing through these organs very strongly with the agent. The power of chloroform to paralyse the heart by its direct action having been established by experiment,* it can be easily understood how this may occur during the inhalation of strong vapour without the functions of the brain and medulla oblongata being entirely abolished, although their functions cease first when the vapour is slowly introduced; for the coronary arteries being the first given off, the heart must receive its supply of the blood newly arrived from the lungs a little in advance of the brain, and becoming more or less completely paralysed the brain suffers rather from the want of circulation, than from the direct effect of the chloroform. (*"On Narcotism by Inhalation [of vapours]," Med. Times and Gazette, 1848, vol. ii.) In many cases of accident, however, the heart and brain are both overwhelmed by the narcotic vapour at the same moment, as might be expected.
It must be quite obvious that a handkerchief, or cotton wool, or lint can afford no adequate means of properly regulating the amount of vapour in the inspired air, when a patient is to be rendered quite insensible by chloroform; and when Medical men do not take the trouble to use an inhaler, which they have studied with the view to regulating these proportions, they should, as I have several times recommended, dilute the chloroform before using it with an equal measure of spirits of wine. The alcohol is hardly any of it inhaled, but it acts by lowering the tension of the vapour, and diminishing the quantity which is inhaled. For instance, 100 cubic inches of air when saturated at 60º Fahr. with vapour from pure chloroform, takes up 14 cubic inches, and it would be dangerous to inhale it of half this strength; but when the chloroform is diluted with an equal measure of spirit, it will only yield 8 per cent of vapour to the air at 60º, even when fully saturated; practically, it easily yields enough to cause insensibility, but not to cause sudden accident.
There is one opinion, which has many advocates among intelligent Medical men, although it seems to me to be supported neither by facts nor reason. It is, that fear on the part of the patient is a cause of death from chloroform. If this were so, accident might be extremely common; for many patients inhale it, unfortunately, with great fear, only because they have a still greater fear of pain; children, also, are usually afraid of anything so strange, yet accidents have seldom happened to them. Mr. Paget's patient was rendered insensible with safety, notwithstanding his fear, and also a second time after his waking. At the time of the accident he indicated by movements some degree of sensibility, but was not conscious, and therefore could not be under the influence of fear.
If chloroform were forbidden, as some recommend, in cases where the patient is frightened, its employment would be extremely limited, and those who most require it would be entirely deprived of its use. It is, indeed, desirable to try to calm any needless fears the patient may have, for fear is injurious while it lasts; and there are two cases--the one at Mr. Robinson's, and the other at St. George's Hosptial--where the patients died suddenly, before enough chloroform had been inhaled to produce any appreciable effect; but these were not deaths from chloroform; and had the patients lived to come under its influence, their fears would have subsided, and they would probably have been as safe as the thousands who yearly commence to inhale it with great fear. Excessive fear and an overdose of chloroform may either of them cause sudden death, just as infancy and old age both predispose to bronchitis; but they cannot combine to cause an accident in the same case. In fact, as soon as a patient becomes unconscious from chloroform, the effects of fear on the pulse quickly subside.
I have on this occasion, as on all others, thought it my duty to express my views as clearly as I could on the subject of chloroform; but it is not my wish to imply any censure on those, either at home or abroad, who do not agree to my views, or follow the same practice. A commission, which lately sat in Paris, reported that in death from chloroform the breathing always ceases before the action of the heart. It doubtless was so in the experiment they performed; and if, in giving chloroform in what may be called the ordinary way, it always cut off the animal suddenly, in the middle of the experiment, we should be at a loss to understand how it could be exhibited to patients in that way at all. Fatal accidents from chloroform are, however, rare under any circumstances, and a careful consideration of those which are well recorded, like the one under our consideration, as well as experiments on animals, contrived and arranged systematically for the purpose, clearly point out the way in which the accidents occur, and how they may be avoided.
Sackville-street, March, 1857.
Return to John Snow Publications
111. "Further remarks on amylene, Part 1"
Source: Snow, John. Medical Times and Gazette 14, 4 April 1857, pp. 332-34. Part 1.
Part 1.
By John Snow, M.D.
In my former paper, which appeared on the 17th and 24th of January, I merely stated, with regard to the preparation of amylene, that it was made by distilling fusel oil with chloride of zinc; and I referred to the original paper of M. Balard, its discoverer, for further particulars.*
(*Annales de Chimie et de Physique, t. lxxxvii. 1844.)
As amylene is beginning to be somewhat extensively used, I think it is desirable that I should quote the process of its preparation more in detail. The crude fusel oil must be submitted to a careful distillation with a thermometer in the retort. It begins to boil at a comparatively low temperature, but that portion only is to be retained which comes over from 130º to 140º Centigrade. Caustic potash is added to decompose the œnanthic ether which the distilled liquid contains, and it is then redistilled, and that portion which boils steadily at 132º Cent. is collected as pure amylic alcohol. Amylene can be obtained from amylic alcohol in the same manner that olefiant gas, or ethylene, can be made from common alcohol, namely, by heating it with dishydrating agents, as sulphuric, phosphoric, fluoboric and fluosilic acids, and chloride of zinc; but most conveniently with the last substance, which is the one that M. Balard employed. The product which is obtained when amylic alcohol and chloride of zinc are distilled together contains at least three distinct hydro-carbons, amylene, paramylene, and metamylene; and the amylene which is the most volatile is separated from the others by successive distillations.
It is probable that the amylene hitherto produced is not entirely free from other hydro-carbons of a similar composition, for its boiling-point is not quite steady. M. Balard gives 39º Cent. (102º Fahr.) as its boiing-point; and I have found this to be the average boiling-point of the amylene I have obtained from Mr. Bullock, but it usually begins to boil freely at about 35º Cent.; and as it evaporates the boiling-point gradually rises to about 43º Cent. There are some specimens which begin to boil at a still lower temperature than 35º Cent., and are put in a state of ebullition by the warmth of the hand, owing to gaseous hydro-carbons, which they hold in a state of solution. The greatest part of the odour of amylene is contained in that portion which distils over below 39º Cent. It is probable that the amylene, as hitherto prepared, contains a little butylene, for butylic alcohol is one of the constituents of crude fusel oil, and it is not likely that amylic alcohol can be obtained entirely free from it by fractional distillation, the only process at present known for its separation.
The fact of amylene not being an absolutely pure body in a chemical sense is no objection to its use, since it can be obtained uniform in all its properties and in its physiological effects. The numerous specimens of amylene with which Mr. Bullock has supplied me, have been uniform in their physical properties, and in their effects. Soon after my former paper was published some amylene was made by M. Berthé, of Paris, which was shown to M. Balard, the discoverer of the substance, and met with his approval. A portion of this was administered by Dr. Debout, to some patients operated on by M. Aran, in the Hospital Saint Antoine, and produced exactly the effects which I had described.*
(*See Bulletin Général de Thérapeutique, 15 Février, p.127. Since the above passage was written Dr. Debout has kindly sent me, through Mr. De Metic, a specimen of the amylene prepared by M. Berthé. I found it to be just like that prepared in London, and I used it in an operation by Mr. Fergusson, in King's College Hospital, with the usual result.)
Dr. Debout also examined some amylene made by Mr. Bullock, in London, and performed some experiments on animals with it, and he found it to possess the same properties as that prepared in Paris.†
(†Ibid. 15 Mars, p. 215 and 223.)
Mr. Bullock has succeeded in preparing amylene during the last few weeks with much less odour than before, and thus the strongest objection to this agent is already in a great measure removed. It is probable that the nearer the amylene approaches to a state of absolute purity, the less will be its odour. A substance was supplied as amylene to one of the large hospitals in London, which produced no effect when inhaled, and I found that it was brownish liquid, having no resemblance to amylene. At another placed the amylene failed to produce an effect, and I was informed that it was adulterated with twice its volume of spirit of wine. This kind of adulteration can easily be detected by shaking a portion of the amylene with water in a graduated tube or minim measure, when the spirit mixes with the water and the amylene rises to the surface. When the amylene is pure it is not diminished in volume by shaking with water; it is perfectly clear and colourless, and it evaporates quickly and entirely when dropped on the hand. Although it has a very distinct odour, somewhat resembling naphtha, it is almost without taste, and it is entirely without pungency, furnishing in this last respect a marked contrast to both chloroform and ether. It produces no irritation or effect of any kind on the sound skin, even when confined, and prevented from evaporating.
Amylene is inflammable, and in pouring it out by candlelight the same care is required as in dealing with sulphuric ether. A slight explosion may be obtained by applying a light to a mixture of a small quantity of its vapour with a large amount of air.
The paramylene, which is produced at the same time as amylene, does not possess sufficient volatility to be inhaled with a view to induce insensibility. It has been tried in Paris, and failed. It boils at 160º Cent. Metamylene, which does not boil till raised to 300º Cent., is still further out of the question. There are, however, other carbo-hydrogens produced in the process of making amylene, which boil at a temperature between the boiling point of amylene and that of paramylene, and, so far as their physical properties are concerned, I thought they might be eligible and convenient for inhalation; but, on making some experiments on guinea-pigs and mice, with a specimen boiling from 85º to 100º Cent., with which Mr. Bullock was good enough to furnish me, I found that the physiological effects were altogether undesirable. It produced illness, debility, and difficulty of breathing, but neither unconsciousness nor anæsthesia.
I have administered amylene in 110 additional cases since January 10, when my former paper was written; and this extended experience has confirmed the observations which I made on the earlier cases. The great ease with which it can be breathed owing to its entire want of pungency, is a decided advantage which it possesses over both ether and chloroform. It rarely causes the least cough, unless the vapour be inhaled too strong at the very beginning; and insensibility can always be induced in as short a time as is desirable, namely, in from three to four minutes in the adult, and about two minutes in young children. It is not desirable to cause insensibility in a shorter time than this with any agent. If narcotism is induced too quickly, the symptoms are not uniform or in regular order, owing, no doubt, to the circumstance that the narcotic vapour is not equally distributed through the blood, which must convey it to the nervous centres. Insensibility can, indeed, be generally induced with chloroform in the time above-mentioned, but there are many cases in which there is considerable delay at the commencement of inhalation, owing to the pungency of the vapour, especially in nervous and in sensitive patients, and in persons with irritability of the air-passages from chronic bronchitis, phthisis, or any other cause.
Further experience has entirely confirmed me in the conclusion that anæsthesia, or the absence of common sensibility, is obtained by the use of amylene with much less coma or stupor than occurs in the use of chloroform or ether. Indeed the greater number of operations under amylene have been performed whilst the patient was apparently awake, although not really conscious of surrounding objects. I am quite satisfied, from experiments which I have performed on animals, that amylene is capable of causing a state of deep coma, and that very quickly, by increasing the quantity of vapour in the inspired air; and I have in two or three instances observed this condition for half a minute or so in a patient; but since pain can be prevented by amylene without deep coma, one abstains from inducing it. The usual absence of come in the employment of amylene cannot be looked on otherwise than as an advantage. It must conduce to the safety of the agent. The reason why no accident is known to have happened from chloroform in the practice of midwifery when superintended by a Medical man, is, no doubt, due to the circumstance that it is only requisite to induce a slight effect, in comparison with the effect required in surgical operations. The best indication that the patient will quietly bear an operation under chloroform, is the more or less complete absence of sensibility of the ciliary edge of the eyelid; but during the inhalation of amylene the patient is often entirely regardless of the surgeon's knife, whilst the edges of the eyelids retain their full sensibility, and the slightest touch causes strong winking. In operations on the eye, however, and in all other cases where great steadiness on the part of the patient is required, I have though it best to continue the amylene till the sensibility of the margin of the eyelid was almost abolished; and to effect this it has usually been requisite to carry the influence of the vapour as far as the beginning of the third degree of narcotism, or that condition in which there is no longer voluntary motion of the eyes, or any other part, and in which the eyelids are usually closed, and the pupils inclined upwards. But even in these cases the patient has usually reverted to the second degree of narcotism before the end of the operation, and has shown signs of ideas by the voluntary motion of the eyes and eyelids, or in some cases by speaking. In several cases, however, the sensibility of the eyelid has been removed in the second degree of narcotism, and important operations have been commenced before the patient was "off," to use an expression familiar on these occasions. One instance of this kind was the operation of lithotomy by Mr. Fergusson on the 14th instant, in a young man, aged 17, in King's College Hospital. The sound was first introduced, and the stone being detected, the assistants were requested to tie the patient up; and finding his limbs somewhat rigid, they requested me to give him some more vapour; if I had been using chloroform, I should have done so without any request, in order to cause relaxation, but I allowed the effect of the amylene to partially subside, and in less than a minute the bandages could be easily applied. I then proceeded to give a little more amylene, but soon found that the margin of the eyelids was insensible, so the operation was performed whilst he was calmly looking about, as if awake, but he showed no signs of pain, and knew nothing of the operation. I never saw a capital operation performed on [333/334] the adult under the influence of chloroform or ether, whilst the patient was in this condition; but I once administered chloroform in St. George's Hospital to a child of three or four years old, which was cut for stone whilst lying calmly with its eyes open, and holding a toy in its hands, all the time of the operation, without letting it fall. In tenotomy, and many other minor operations, I have merely continued the amylene till an altered expression of countenance indicated that the patient was no longer conscious of his situation, or of surrounding objects, and the operations have always been completed without the patient's knowledge, although awaking often within a minute afterwards.
There is a tendency to laugh during the inhalation of amylene much more frequently than during the inhalation of chloroform. It occurs just after the patient has lost his consciousness, but it is soon subdued by the increasing effect of the vapour. The colour of the countenance is generally heightened more or less during the whole period of the inhalation. The expression generally remains calm and cheerful, but in a few instances there is a singular, and even unpleasant aspect of the countenance for a short time, arising apparently from a brief spasmodic action of the muscles. I have only met with strong mental excitement in three patients, all females; it subsided in half a minute in one case on leaving off the vapour, and was as quickly subdued in the others by continuing it. The excitement did not return in the first case, when the inhalation was resumed.
The pulse is almost always accelerated during the early part of the inhalation, and the breathing at the same time quickened. In many of the early cases in which I administered amylene the pupil was dilated for a short time, and I consider that this arose from giving the vapour rather stronger than is desirable. I have lately given the vapour more gently, and for several weeks I have not observed the pupils to be dilated; they have remained, as nearly as I could tell, of the natural size, and also sensible to light, in the cases where I have made an observation on that point.
There has been some amount of rigidity and spasm in a considerable number of cases in which I have employed amylene, but not to the extent which occurs sometimes in the employment of chloroform. The rigidity, moreover, is of a somewhat different kind, and occurs in patients in whom we should not expect it from chloroform. In the spasm and rigidity from the latter agent the head is more commonly bent forwards, or turned to one side, although occasionally it is thrown back; but under amylene the latter is the usual position it assumes when rigidity occurs, constituting a brief opisthotonus. The rigidity under the influence of chloroform is usually accompanied with struggling, while in that caused by amylene the patient is generally quieter. The person in whom rigidity and struggling are most violent from the effects of chloroform are lean, muscular men, who work at hard labour, or follow athletic sports, such as hunting, and especially boating; while those who lead a sedentary life, or are reduced by illness, seldom exhibit these phenomena. Women and children seldom exhibit any rigidity under chloroform, and fat persons least of all. Old people do sometimes, especially if thin. Under the use of amylene, on the other hand, I have most frequently met with some amount of rigidity in children and young persons, while many robust men, in whom it would be almost certain to occur under chloroform, have not shown any signs of it. The cause of this probably is, that the operation has generally been performed without carrying the narcotism beyond the second degree, while rigidity does not take place till the third degree is attained. In every case where rigidity and struggling have occurred in the employment of chloroform, however violent these symptoms might be, I have continued the vapour gently and steadily till they were subdued, either by removing the tendency to these symptoms, or by carrying the narcotism to the fourth degree, which is accompanied by relaxation of the voluntary muscular system, and usually with some tendency to stertor. When the struggling from chloroform is once subdued it rarely recurs during the operation, although there are a few patients, especially among hard drinkers, who have a tendency to struggle whenever the effect of the chloroform diminishes. In the use of amylene, on the contrary, I have not attempted to subdue the spasm by continuing the inhalation, but have, with the exception of a case of dislocation, to be mentioned further on, withdrawn the vapour when the rigidity appeared, and the operation has either been performed at once, or else, if it was of a nature that the spasm would interfere with, I have waited a short time, and exhibited a little more vapour very gently. I have every reason to conclude from experiments which I have made on animals, that the spasm caused by amylene could always be subdued by increasing the strength of the vapour; but I have not followed this plan, as it appears to be unnecessary. In fact, I have reason to believe that in some of the earlier cases in which I administered amylene, a certain amount of spasm, which might have been avoided, was induced by carrying the effects of the vapour a little further than was necessary, or by giving it a little more quickly than was desirable.
I stated in my former paper, that I had not met with sickness in any of the twenty-one cases in which I had exhibited amylene. I afterwards learnt, however, that vomiting had occurred in one of these cases two or three hours after the operation. In the subsequent 110 cases I have only been able to hear of sickness in seven instances, although I have been able to make inquiry respecting all but a few of the patients. What is remarkable is, that I have not seen vomiting take place in any instance in which I have administered amylene, although in the last hundred cases in which I have given chloroform twenty-two of the patients, or more than one-fifth, vomited before I left the room. This occurred, notwithstanding that directions had been given in the greater number of instances not to take a meal before the operation. Certainly, these directions were given in a greater proportion of the chloroform cases than in those where amylene had to be inhaled. I administered amylene on January 30 to a lady about 25, while Mr. Bowman operated for strabismus, and there was no vomiting or sickness, either at the time of the operation or afterwards; but the same patient had undergone a similar operation a week previously, when chloroform was administered, and on that occasion vomiting commenced before the operation was finished, and recurred every quarter of an hour, with violent retching, for twelve hours. The sickness caused by chloroform usually begins at the time of the operation, or within a quarter of an hour afterwards; the most usual time for it being, as consciousness is returning; and if there is no sickness after chloroform till some hours have elapsed, there has generally been a dose of opium in the mean time, or some other cause, which would account for it. The few instances of sickness which have happened after amylene, however, have chiefly occurred at the end of a few hours, although there was no intervening cause for it. The sickness has not been severe in any case; it was generally a single attack of vomiting, after which no feeling of sickness remained.
[Part 2 appeared in the 11 April issue.]
Return to John Snow Publications
112. "Further remarks on amylene, Part 2"
Source: Snow, John. Medical Times and Gazette 14, 11 April 1857, pp. 357-59. Part 2
Part 2.
By John Snow, M.D.
Amylene differs widely from chloroform, and still more from sulphuric ether, in the promptitude with which patients generally recover from its effects. This is a character of amylene which might have been predicted from its physical properties. I have many times observed how quickly, and, indeed, almost instantaneously small animals recover from the stupor occasioned by certain permanent gases which are sparingly soluble in watery fluids, as olefiant gas, carbonic oxide and carbonic acid gases, nitrous oxide and the gaseous oxide of methyle. Now amylene is so volatile as to approach to a permanent gas; at a temperature a little above that of the human body it would be a gas, and the vapour is very sparingly soluble in water fluids, and consequently in the blood. Suphuric ether is, indeed, as volatile as amylene. I cannot remember any other two bodies whose volatility is so nearly alike; but sulphuric ether is very soluble in watery fluids, in comparison with amylene. Water dissolves a tenth of its volume of liquid ether, or 23 volumes of the vapour. Consequently a large quantity of ether is absorbed during inhalation, and the blood has to pass many times through the lungs before it is freed from it. The quantity of amylene which is absorbed is, on the contrary, extremely small, as I explained in my paper in January, and this, together with its volatility, is no doubt the reason why the patient recovers so promptly from its influence. In about a minute after the operation is concluded, and the inhalation left off, the patient usually awakes from the influence of amylene, and completely recovers his consciousness. The same quick recovery may take place after chloroform, but more frequently it is a few minutes before the patient is quite conscious. I have seen two or three instances in which a child has slept for twenty minutes or half an hour after amylene, but it must be remembered that children sometimes sleep for hours after chloroform in cases where the operation has not produced a painful wound. The quick recovery of the patient is a decided advantage in all minor operations. In great operations, where the patient is obliged to keep his bed afterwards, it is of less consequence whether he wakes promptly or not, although, even under these circumstances, his friends are generally anxious to see him recover his consciousness. The smarting of the wound after an operations is often prevented longer when chloroform has been employed than after the use of amylene, and this may be considered as a slight advantage which chloroform possess in certain cases. In some instances, however, in which chloroform has been used, the patient begins to show symptoms of suffering pain in the wound before he has entirely recovered his consciousness, while after amylene I have not seen symptoms of pain in the wound till consciousness has completely returned. In any case where the pain after an operation, either from a wound or ligature or caustic, is very great, the inhalation of the agent which has been employed may be gently repeated at times until the pain has a tendency to subside, or till an opiate shall take effect.
The patient generally seems surprised or confused on first recovering from the effects of the amylene, but in a few seconds he becomes, in most cases, completely conscious of his position, and feels that his mind has been wandering. He often says he does not know where he has been in his dreams, or that he has been a long way. Sometimes he does not remember exactly what he has dreamed about; at other times he does. All this is common enough after chloroform, except that the process of recovery is generally much slower; but there is one condition of mind which is very common after chloroform, which I do not remember yet to have met with after amylene. If the patient, when he awakes from even a deep and prolonged insensibility, is in the same position as when he became unconscious, he often asserts that the vapour has not taken effect, he requests that the operation may not be commenced, and will not believe it is over till convinced by his own senses. It seems as if, in such cases, a piece has been snipped, as it were, out of the mental existence of the patient, and that not even dreams had occurred.
The patient has nearly always a very cheerful expression of countenance when he recovers from the amylene, and the state of his mind, as indicated by his conversation, corresponds to his look. Dr. Debout has noticed the same circumstances. Speaking of the patients operated on under amylene in Paris, he says, "A leur réveil et le premier moment de stupeur passé, leur physionomie est épanouie." The same state of countenance and mind is met with after chloroform only now and then, and is by no means the rule. I have met with hysterical laughing and crying in three females after operations under amylene, which I think is not oftener than the same symptoms might be met with after chloroform. In one case where Mr. Fergusson amputated the leg of a young woman, the hysteria lasted about an hour; in the other two cases it subsided in a much shorter time, although the patients were very subject to this affection.
Amylene appears to support the pulse under loss of blood at least as well as chloroform. I have not as yet found the pulse to fail, although there was rather free hæmorrhage in one or two operations.
There has been a little headache in a few cases as the effects of this agent were subsiding, but it has passed off in a few minutes.
I have already administered amylene in many of the chief operations of surgery. There have been five cases of lithotomy in the male, three of them by Mr. Fergusson, in King's College Hospital; the young man and the child already alluded to in my former papers, and another child; and two cases in St. George's Hospital, one by Mr. H. C. Johnson, and the other by Mr. Pollock, both children. All the five cases have done well. In addition to the amputation of the thigh by Mr. Henry Lee, mentioned in the paper in January, I administered amylene in a similar operation by Mr. Tatum, in St. George's Hospital, and also in an amputation of the forearm by the same gentleman, and an amputation below the knee by Mr. Fergusson, in King's College Hospital. I have administered amylene in the removal of the head of the femur by Mr. Bowman; in the removal of three large tumours near the groin, two of them by Mr. Bowman, and one by Mr. Fergusson; in the removal by Mr. H. C. Johnson of a tumour deeply seated behind the angle of the jaw, and in the removal of six tumours of the breast by different Surgeons. There have also been three operations for stricture by perineal section, two by Mr. Fergusson, and one by Mr. Curling. The amylene has answered perfectly well in all these cases, so there can be no doubt of its general applicability in the great operations of surgery.
Amylene has succeeded perfectly well in operations of the eye. In the extraction of cataract it will probably have an additional advantage, in the almost entire absence of sickness after its use. I have exhibited it in two cases of extraction of cataract, performed by Mr. Bowman, and one operation for cataract by drilling. Also in six cases of excision of the eyeball for various diseases, by Mr. Bowman; one of these cases occurred in King's College Hospital, one in the Ophthalmic Hospital at Moorfields, and the others in private practice. There have been also twelve operations for strabismus, and a number of other operations on the eye and the eyelids, in which I have administered amylene chiefly for Mr. Bowman. I have given it in three cases of the forcible rupture of the adhesions in anchylosed joints, and it has answered perfectly in preventing the pain. Two of the cases were in King's College Hospital, and one in the Orthopædic Hospital, under Mr. Lonsdale.
I have employed amylene in two cases of dislocation of the humerus, both patients of Mr. French in the St. James's Parochial Infirmary. The first case was a dislocation downwards in a woman aged 68. She inhaled for three minutes, when extension being made, the bone slipped into its place with the utmost ease, although Mr. French had found a good deal of resistance in an attempt he made just before sending to me--not any serious resistance or pain, but so much of both as led him to think it would be a good opportunity for trying the amylene. In two minutes after the reduction of the dislocation, and five minutes after beginning to inhale, the patient was awake again, and said that she had felt nothing. The other case was a dislocation forwards in a man aged 72. No attempt to reduce it was made till the amylene was administered. The case was under the care of Mr. Buzzard. After inhaling two or three minutes, the old man got into a state of muscular rigidity, and did not get beyond this state, although I continued the inhalation nearly ten minutes until about two ounces of amylene were used. He was quite insensible, but the rigidity prevented the reduction of the dislocation. So I discontinued it, and sent for some chloroform, which I administered a few minutes afterwards. It produced muscular rigidity rather stronger than that which the amylene had caused, but by continuing the inhalation steadily for about two minutes, the limbs became relaxed, and the humerus slipped easily into place. This is the only case in which the amylene has not effected the purpose for which I have exhibited it; and I have no doubt, for reason which I stated before, that I could have produced relaxation of the voluntary muscles by increasing the strength of the vapour the patient was breathing; but there were one or two circumstances which at the moment stood in the way of this. The patient's face was so hollow from his loss of teeth that the face piece fitted badly, and as it was early in a frosty morning the water bath of the inhaler was colder than usual. These defects could have been remedied if necessary, but I thought it as well to use chloroform; and I am inclined to think that chloroform is the better agent to employ in those rare instances where relaxation of the voluntary muscular system is required. I remain also of the opinion, which I expressed years ago, and which I occasionally act on, that sulphuric ether is preferable to chloroform in the reduction of old dislocations, as it seems to produce complete relaxation of the muscles more readily and constantly than chloroform.
Amongst the minor operations in which I have administered amylene, have been eighteen operations of tenotomy, chiefly by Mr. Williams Adams and Mr. Lonsdale, in the Royal Orthopædic Hospital, and mostly in children and young people. An inhalation of about two minutes generally sufficed to prevent the pain entirely. I find that some surgeons have entertained an objection to use chloroform in tenotomy, lest it should cause a relaxation of the muscles, which would interfere with the operation. I have, however, been in the habit of exhibiting it for eight or nine years, both in King's College Hospital and in the private practice of Mr. Fergusson and some other surgeons. I never carried the effect of the chloroform so far as to cause relaxation of the muscles, and I have generally heard the tendons give way with a snap. With a small dose of amylene the tensions of the muscles not only remain, but is usually somewhat increased.
Amongst the more important and painful operations in which I have given amylene, and where it has answered perfectly, I ought to have mentioned several cases of necrosis affecting various bones,--as the femur, lower jaw, tibia, etc. I administered it to an infant about six months old, in King's College Hospital on January 17th, previous to Mr. Fergusson operating for hare-lip. The child was insensible to the knife at the beginning of the operation, but began to cry before the incisions were finished, and cried very lustily as the hare-lip pins were introduced. The property, previously alluded to, which amylene possesses, of allowing the patient to awake so quickly, although an advantage in most operations, is not desirable in operations about the mouth, where the inhalation cannot very well be continued or resumed. This is more especially the case in young children, who awake, even from chloroform, more quickly than we wish in such operations. There have been four or five operations on infants for hare-lip since the one above mentioned, but I have given either chloroform or sulphuric ether. In all the other operations in this Hospital, when I have been present to administer any narcotic vapour, since the 13th of December last, I have exhibited amylene, in order to give it a fair trial. There have been several plastic operations on the face in patients of adult age, or nearly so. The amylene has always prevented the pain at the beginning of the operation, and has been continued on a hollow sponge afterwards for some little time. On two or three occasions it was so continued with success to the end of the operation; but two or three times the sponge became so cold by the continued evaporations of the amylene, as to make my fingers ache, and to limit the evaporation so much that the patient seemed about to awake. I therefore put a little chloroform on the sponge, and it answered the purpose desired. Chloroform absorbs much less caloric than amylene during its evaporation, as the patient inhales, on account both of the quantity which evaporate being less, and of the specific gravity of the vapour being greater.
In tooth-drawing, amylene has both its advantages and disadvantages as compared with chloroform. The prompt recovery from its effects, and the almost constant absence of sickness, are decided advantages, as also is the greater ease with which it is inhaled; but in cases where eight or ten teeth require to be extracted at once, as often happens, where my assistance is required, or where several stumps are in the alveolus, the effect of amylene does not last long enough to complete the operation, without one or more repetitions of the inhalation. A difficulty in getting the mouth open occurs about as often, I think, with one agent as the other.
I have only as yet had leisure to administer amylene in two cases of labour. One was under the care of Mr. Buzzard in the St. James's Infirmary, on January 20th. It was the patient's second labour, and was a lingering one, having lasted 35 hours. I administered the amylene only during the last 20 minutes preceding the birth of the child, the head being advanced so as to rest on the perinæum. The vapour was given well diluted at the beginning of each pain. The patient breathed very deeply, and got relief very quickly from each pain; the mind was quite clear between the pains, and I could not tell whether or not the consciousness was removed for half a minute or so, during each pain. Half a fluid ounce of amylene was used. The other case occurred in an out-patient of King's College Hospital under the care of Mr. Meadows, Dr. Farre's assistant. It was the patient's third confinement. I arrived three hours after the commencement of labour, and two hours before the birth of the child. The os uteri was almost dilated on my arrival, and the pains were very strong, recurring every three minutes or so. They continued to increase in strength to the last. The patient was probably unconscious for a brief period during the uterine contractions, while the amylene was administered, but between the pains she was quite conscious. Under the use of chloroform, in a labour with brisk and frequently recurring pains, as in this case, the patient usually sleeps on from one pain to another, but I offer no opinion at present as to which state of circumstance is preferable. The amount of amylene inhaled in this case was three fluid ounces. The quantity used in each of these cases must have been about half a fluid drachm in each pain, and this is the quantity I had previously recommended Dr. Tylor Smith to employ, when he did me the honour to ask me some questions about amylene before he employed it in a case of labour. The results arrived at by Dr. Tylor Smith, in the case in which he employed amylene, were similar to my own, viz.[,] relief of suffering during the uterine contraction, consciousness between pains, and no interference with the progress of labour. I look forward with some interest to a more extended experience of amylene in midwifery. Chloroform answers so extremely well that there does not seem much room for improvement; there are cases, however, in which chloroform has a tendency to retard the progress of labour, by diminishing the force, duration, and frequency of the uterine contractions, even when administered very moderately; and it remains to be ascertained, by observing a number of cases, whether amylene may not be free from this disadvantage.
In the concluding part of this paper I shall make some remarks on the mechanical means of administering amylene in the most efficient way, and on its relative safety as compared with chloroform and ether.
[Part 3 appeared in the 18 April issue.]
Return to John Snow Publications
113. "Further remarks on amylene, Part 3"
Source: Snow, John. Medical Times and Gazette 14, 18 April 1857, pp. 379-82. Part 3.
Part 3.
By John Snow, M.D.
The most exact way of administering any narcotic vapour is that which I have been in the habit of pursuing in experiments on animals, namely, to place them in an air-tight vessel so large, relatively to their size, as to represent a considerable apartment, and to introduce a known quantity of the narcotic agent in such a manner that the vapour should become uniformly diffused through the air. This method is evidently inapplicable to the human subject, but I tried a plan in a few cases in 1849, which very nearly approaches to it in point of accuracy; this was, to put a measured quantity of a volatile liquid into a balloon of known size, to fill it up with air by means of the bellows, and let the patient breathe from it. With so much chloroform as produced four per cent of vapour, in proportion to the air, the effects were extremely uniform, the patients becoming insensible in three or four minutes, according to the greater or less freedom of respiration, and the vapour being easily breathed, owing to its being so equally mixed with the air. I did not try, however, to introduce this plan into general use, as the balloon would sometimes have been in the way of the Surgeon, and filling it with the bellows would have occasioned a little trouble. It seemed necessary to sacrifice a little of absolute perfection to convenience, and I therefore continued the plan which I had already followed.
The great point to be observed in causing insensibility by any narcotic vapour, is to present to the patient such a mixture of vapour and air as will produce its effects gradually, and enable one to stop at the right moment. Insensibility is not caused so much by giving a dose as by performing a process. Nature supplies but one mixture of diluted oxygen, from which each creature draws as much as it requires, and so, in causing insensibility by inhalation, if a proper mixture of air and vapour is supplied, each patient will gradually inhale the requisite quantity of the latter to cause insensibility, according to his size and strength. It is indeed desirable to vary the proportions of vapour and air, but rather according to the purpose one has in view, whether medicinal, obstetric, or surgical, than on account of the age or strength of the patient; for the respiratory process bears such a relation to the latter circumstances, as to cause each patient to draw his own proper dose from a similar atmosphere in a suitable time.
When sulphuric ether was first introduced, it was often very slow in producing the desired effect, and not infrequently failed altogether, owing to the great cold produced by its own evaporation. The sponge, or whatever contained the ether, was often reduced much below the freezing point, and the patient went on breathing air of an arctic temperature with very little vapour in it. By using a metal inhaler, and placing it in a good quantity of cold water, which replaced the caloric carried off by the vapour, I was enabled to cause insensibility in four or five minutes, in every patient who was able and willing to breathe the vapour of the strength which was supplied. When the use of chloroform was introduced by Dr. Simpson, I retained a small water-bath with the inhaler I employed, as a regulating power, and quite as much to prevent the vapour from being in excess as to ensure its sufficient quantity.
In the use of amylene some kind of inhaler is required to prevent a great loss of the article, and to insure its producing its effects. I have supplied amylene on a hollow sponge several times, to keep up the effect, after insensibility had been produced by means of an inhaler, and in short operations, such as most of those on the eye, it has answered perfectly, but in the longer operations, not always so well. In applying amylene in this way the moisture of the breath is condensed on the sponge, and congealed, so as to produce the appearance of hoar-frost, and at the temperature of freezing water, the air does not take up enough of the vapour of amylene to cause insensibility. M. Tourdes, of Strasbourg, has, indeed, succeeded perfectly in making children insensible with amylene by means of a sponge placed in a hollow cone of waxed cloth, with a small aperture at the extremity. The waxed cloth, no doubt, causes the warm breath to counteract, in some measure, the cooling effect of the evaporation. In an operation on the adult, however, in which M. Rigaud, of Strasbourg, applied amylene in this manner, he used 100 grammes (between four and five fluid ounces) in causing insensibility.
In administering amylene, I have employed the same kind of inhaler which I have used for many years in the exhibition of chloroform. I have lately had one made a little deeper, to adapt it better to the larger quantity of the agent used, and to make the water-bath a little more capacious. It is figured in the adjoining wood-cut. The inhaler itself is on a scale of half the dimensions, but the artist has drawn the face-piece on a smaller scale. The temperature of the water-bath varies according to that of one's dwelling-rooms, at different times of the year, but I am in the habit of diminishing the depth of the coils of bibulous paper in the inhaler in warm weather. The quantity of vapour can also be diminished to any extent by turning the expiratory valve of the face-piece more or less to one side.
[text at bottom of figure]
a. Outer case for water bath.
b. Cylindrical vessels into which the amylene is put; it is lined with a coil of bibulous paper up to the point c.
d. Cylindrical frame which screws into b; it has apertures at the top for the admission of air, and its lower two-thirds are covered with two coils of bibulous paper, which touch the bottom of the vessel b. except where the notches are cut in them.
f. Elastic tube.
g. Face-piece.
h. Inspiratory valve.
i. Expiratory valve: the dotted lines indicate the position of the valve when turned aside for the administration of air not charged with vapor.
From experiments I have made with the inhaler, by passing a measured quantity of air through it, in the way in which it passes through during inhalation, and weighing it before and afterwards, I find that when the water-bath is at 56º Fahr. the air takes up 16 per cent of the vapour of amylene, and at 62º nearly 19 per cent. For instance, 625 cubic inches of air carried off 76 grains of amylene at the former temperature, and 90 grains at the latter.
In speaking of the bisulphuret of carbon in 1848,* I said, "On account of the great volatility and very sparing solubility of this substance, the point of relative saturation of the blood by it is soon reached;" and further I said, "Indeed, I feel convinced that if a person were to draw a single deep inspiration of air, saturated with it at a summer temperature, instant death would be the result."
(*London Medical Gazette, vol. i. 1848, p.1077.)
Last autumn, when I commence[d] my experiments on amylene, and ascertained its extremely sparing solubility, only one part to upwards of ten thousand of water, I was apprehensive that the above remark would apply to this agent; but on finding afterwards that the blood required to absorb about one-fifth as much of amylene as would saturate it, before a deep state of insensibility was induced, instead of only one part in thirty-one, as in the case of sulphuret of carbon, the question was very much altered, and I came to the conclusion that it might be inhaled with at least comparative safety. I soon became aware, however, that it was capable of acting directly on the heart, if given too strong, or not well regulated. In one of the early experiments which I made to ascertain the effects of this substance, I placed a guinea pig in a jar holding 428 cubic inches with 25 grains of it. In two minutes and a half the animal was quite insensible. Soon afterwards the breathing became slower, and it ceased at the end of three minutes and a half from the beginning of the experiment. I immediately took the animal out, and in ten or fifteen seconds it gave a gasp, and in a few seconds more the breathing became quick and natural. There was, however, no action of the heart to be heard with the stethoscope, and, although the breathing continued for three minutes, the action of the heart did not return. The chest was opened immediately after the breathing ceased. The auricles were acting briskly, but the ventricles were not contracting. The right one was much distended with blood.
I concluded that the vapour was not properly mixed with the air in the above experiment, and that there had been an undue proportion of it at the bottom of the jar. I soon found that this must have been the case, for on introducing the amylene through an aperture contrived in the cover of the jar, and allowing it to evaporate gradually from a sheet of blotting paper suspended within, I found that twenty-five grains only produced a state of inebriation with staggering, however long the animal might breathe it, and that it was necessary to increase the quantity to forty-eight grains in order to induce a moderate state of insensibility. With the above quantity the air in the jar contains fifteen per cent of vapour. I found in several other experiments that the amount of vapour may be increased to twenty-five per cent, and that guinea pigs may breathe it for four minutes without danger. It was only by increasing the amount of vapour up to nearly forty per cent that I was able to arrest the action of the heart of a guinea pig by the direct effect of the amylene in such a way that the gasping respirations which followed did not restore its action. With a kitten six weeks old I did not succeed, even with vapour of this strength, for when the action of the heart seemed to have ceased, or to be on the point of ceasing, the respirations of the animal, when it was withdrawn from the vapour, always restored it.
Three cats, indeed, died with a less amount of vapour, but they died slowly. One of them was placed in a jar holding 3,000 cubic inches, and a fluid drachm of amylene was introduced on blotting paper every two minutes. The cat became gradually insensible after the sixth drachm had evaporated, and the breathing ceased as the eleventh drachm was evaporated, upwards of twenty minutes after the commencement of the experiment, and when the amount of vapour had reached between seventeen and eighteen per cent. The animal was immediately taken out and the stethoscope applied to the chest. The heart continued to beat for three minutes, quickly at first, more slowly afterwards, and it gradually ceased without any further respiration. I caused a cat to breathe air from a large bladder containing 20 per cent of the vapour of amylene, while the stethoscope was applied. The breathing became embarrassed, and the action of the heart rapid, but I did not succeed in stopping the latter. When mice are exposed for half a minute to air containing eight or ten per cent of vapour of chloroform, and taken out as the breathing gets embarrassed, I have always found them get worse and die; but if they are placed for half a minute in air containing 25 per cent of vapour of amylene, and taken out under the same circumstances, they recover.
Under all these circumstances I concluded that amylene might be employed with a greater prospect of safety, if care and caution were used; for it is only by the sudden action of a narcotic vapour on the heart that a patient would be allowed to die in the presence of a medical man.
In speaking of amylene in my paper published in January,* I said, "Whilst I cannot venture to predict for it the absolute safety which seems to attend sulphuric ether under all circumstances, I confidently trust that it will be perfectly safe with careful management;" and, further, "It is my opinion that the cold produced during its evaporation would, in all the ordinary methods of inhalation, prevent the air taking up a quantity of vapour which would be dangerous."
(*Medical Times and Gazette, p. 84.)
Mr. Clarke, of Bristol, in a paper published in the British Medical Journal (March 28), says of amylene, "It seemed impossible to get too much into the system, and with this I have been greatly impressed; it is this fact that appears to me to promise an immunity from danger. . . . It requires to be given almost unintermittingly, and requires the same amount of attention to keep up its effects as chloroform does to keep the patient safe. The direction of the attention, however, is one less calculated to give anxiety." Dr. Debout stated, as the result of some experiments on animals, in which he was assisted by M. Duroy, that if it sufficed to double the quantity of chloroform in order to transform the anæsthetic dose of that agent into a poisonous dose, it was necessary to quadruple that of ether, and to quintuple that of amylene, in order to arrive at the same result, and that, therefore, the innocuousness of the new agent was still greater than that of sulphuric ether.†
(†Bulletin Général de Thérapeutique, 15 Mars, p. 223.)
In a paper which Professor Tourdes, of Strasbourg, read before the Academy of Medicine of Paris, he came to the conclusion, from a series of experiments and observations, that "amylene was evidently much less dangerous than chloroform, perhaps even than ether." In a subsequent paper, M. Tourdes says that the innocuousness of amylene is indicated theoretically by the insolubility and volatility of that substance; but this is a mistake; the insolubility and volatility which are a cause of the prompt recovery of the patient, as I have explained, are also a cause of its quicker action, and demand greater care in its administration; so that whatever safety amylene possesses is not a consequence of these properties, but rather exists notwithstanding they are present.
These sanguine expectations of the French investigators, and my own more moderate hopes, have been greatly disappointed by an accident which has happened in my own hands, since the last part of my paper was in print. Mr. Fergusson requested me to assist him on the 7th instant, in the case of a gentleman on whom he was about to operate for fistula in ano. The patient was 33 years of age and was in good health, with the exception of the local complaint, although he had lived somewhat freely. Mr. Fergusson examined the patient's chest the day before the operation, and found the sounds of the heart to be normal. I felt his pulse just before he began to inhale. It was natural, but somewhat accelerated, as usually happens just before an operation. He was lying on his side in bed. About six fluid drachms of amylene were put into the inhaler, (I never intentionally use all I put in, but add more before the paper become dry,) and he breathed steadily and gently. The valve was gradually advanced over the opening in the face-piece till it about three-quarters covered it, and the patient appeared to become quietly unconscious in about two minutes. He breathed quickly for a few inspirations just as he appeared to become unconscious. Just after this Mr. Fergusson came and felt the patient's pulse, and he says it was very good. I felt it also. I looked at my watch at this time, and it was two minutes and a-half or two and three-quarters from the beginning of the inhalation. Mr. Fergusson commenced to use the probe, and, finding the patient did not flinch, he began to use the bistoury. Mr. P. C. Price assisted at the operation. I held the patient's thigh with one hand, as I often do in such an operation, lest he should flinch. He did not flinch, however, but kept his limbs tense, without moving them. Just at this moment I observed that the valve of the face-piece, which I had left three-quarters covering the opening, had moved so as to cover it entirely, but I cannot say whether or not the patient had taken an inspiration a little stronger than I intended, and thought nothing of the matter, as I have frequently had to close the valve completely in giving amylene. It could not, however, have been many seconds in that position, for I paid no attention to the operation, except so much as was requisite to guide me in what I was doing. The inhalation was discontinued at the moment I have mentioned, and on looking round directly after I found that the operation, which had apparently been but one incision, was finished. I now began to feel for the pulse, more out of constant habit, and from a scientific curiosity, than from any supposed necessity of doing so. Although it had been good only half a minute before, I could not find it in the left wrist, and only a slight flutter in the right one. His breathing was, however, good, indeed quite natural, and he did not seem even to be very insensible, for there was some motion both of his features and limbs as if he were about to awake. I watched the patient with great anxiety, thinking that surely his good and natural breathing would restore the pulse, and feeling that at all events this superseded any other measure at the moment. In two or three minutes, however, he seemed to be getting more insensible; he did not wink on the edge of the eyelids being touched, and the breathing was getting slower and deeper. I called Mr. Fergusson's attention to the patient, and both he, who was preparing to go away, and Mr. Price, who had all the time been standing by the patient, were surprised to find that anything could be wrong, as they has seen the patient going on apparently so well, not only during the inhalation, but after it was discontinued. They dashed cold water in his face, which did not seem to have any effect. His countenance was now livid, and his breathing of a gasping character. It soon began to leave off, with the exception of deep, distant, gasping inspirations, and we therefore began to perform artificial respiration, by Dr. Marshall Hall's method, placing him in the prone position, and bringing him partly round, while Mr. Price kept the mouth open. The air could be distinctly heard passing through the larynx during this motion. We also tried pressing on the chest with the head on one side and the mouth open, which answered very well as regarded the ingress and egress of air. Inflation from mouth to mouth was tried, but did not seem to answer so well. Although deep gasping inspirations were made by the patient till fully ten minutes had elapsed from the failure of the pulse, the measures used had no effect; I believe that I heard a feeble motion of the heart even after this period; and, as Mr. Fergusson perceived a slight pulsation at the same time in the right wrist, I was probably not mistaken. There were no further signs of life after this, although the artificial respiration was continued for a long time. I am quite sure as to the length of time respiration continued after the failure of the heart's action. The pulse ceased to be distinctly perceptible at ten minutes before five, and the patient was still breathing at five o'clock. He had not taken food for some hours, but drank a pint bottle of ale a little while before the operation. A good portion of amylene remained in the inhaler after it had been uncovered for an hour and a half.
There was an examination of the body forty-eight hours after death. The body was rigid. There was a good amount of fat beneath the integuments. The cartilage of the ribs were ossified. The lungs were large, and did not collapse; they completely filled the cavity of the chest, and seemed by their texture to be emphysematous, although there were no large cells on the surface. There was a little congestion at the posterior surface of the left one, otherwise they were not very vascular. There was a little clear fluid in the pericardium. There was a good deal of fat on the surface of the heart, which was somewhat larger than natural. It was removed by cutting the great vessels before it was opened, and in removing it three or four ounces of dark-coloured fluid blood escaped. The right ventricle was somewhat dilated, otherwise the heart was healthy; the walls of the left ventricle seemed very thick, but it was contracted, so as almost to obliterate the cavity. The liver was vascular, dark coloured, and friable. The stomach was healthy, and contained only a little mucus. The organs were not examined. There was no odour of amylene in the body.
Although I used every care and attention in this case which seemed to be possible, I cannot attribute the patient's death to any other cause than the amylene. The failure of the pulse took place at the moment when the operation was performed; but, as the patient was unconscious, I can hardly connect the two events,† (†there are, however, some authorities who would still do so) or I might illustrate the case by one which I witnessed two or three years ago. In that case the Surgeon performed an operation for fistula, before the patient was unconscious, in mistake, and immediately afterwards the patient, a youngish man, went through the process of apparently dying; but, fortunately, gave a gasp and recovered. He then told us what I very well knew, the he had felt the pain of the operation. He said that he did not complain, as he expected to feel it; for he could not believe what had been told him about chloroform.
I believe the patient had emphysema of the lungs. There was no such force used in the artificial respiration as could permanently dilate the air-cells, and the dilation of the right ventricle indicates some chronic obstruction to the pulmonary circulation. In commenting on a case of death from chloroform, which occurred at the Mauritius, I made the following remarks:‡--"The reporter considered that the emphysema was the cause of death, by interfering with expiration, and thus detaining the vapour; and it must be admitted that, if the vapour were not sufficiently diluted with air, the emphysema would increase the danger. At the same time I have had practical experience to show, that when it is sufficiently diluted, it may be safely inhaled, even in extreme cases of emphysema."
(‡London Journal of Medicine, May, 1852.)
The continuance of respiration so long after the heart is paralysed, in the case I have related above, and in some deaths which have happened from chloroform, is an extremely curious event. It proves that some little circulation must be still going on through the brain, and, in fact, the slight fluttering pulse and feeble sounds of the heart once or twice heard indicate this; but, under these circumstances, why does not the [381/382] heart recover itself? If the circulation were going on in the coronary arteries, it might be expected that the blood from the lungs, which has been aerated by respiration and freed from the narcotic vapour, would restore the action of the heart. Dr. Cockle has expressed the opinion, which is very probable, that the blood enters the coronary arteries in a retrograde manner, during the diastole of the ventricles, when the aorta and such great arteries are contracting on their contents; if so, with a very feeble circulation, the elasticity of the aorta, perhaps, cannot sufficiently act to cause a backward current, and perhaps, also, the over-narcotism of the heart is itself an obstacle to the coronary circulation, by the congestion in the capillary system which always attends on narcotism.
The above accident happened in the 144th case in which I have administered amylene. It is impossible to form an average from a single case. I do not know any reason why an accident like the above might not have occurred in one of the early cases in which I was giving chloroform, or, on the other hand, why I might not have been able to go on for four of five years at a time administering amylene, without any approach to an accident. The investigation of this agent has been actively taken up on the Continent, and the extent to which it will ultimately be used will probably not be much influenced by the occurrence I have had to relate.
18, Sackville-street, April, 1857.
Go to Group 14 (# 114-124)
Click to return to Stream 1 - d: John Snow's Publications
Click to continue to Stream 1 - e: Memoir of his friend Benjamin Ward Richardson
 (# 103-113)
(# 103-113) Return to John Snow Publications
Return to John Snow Publications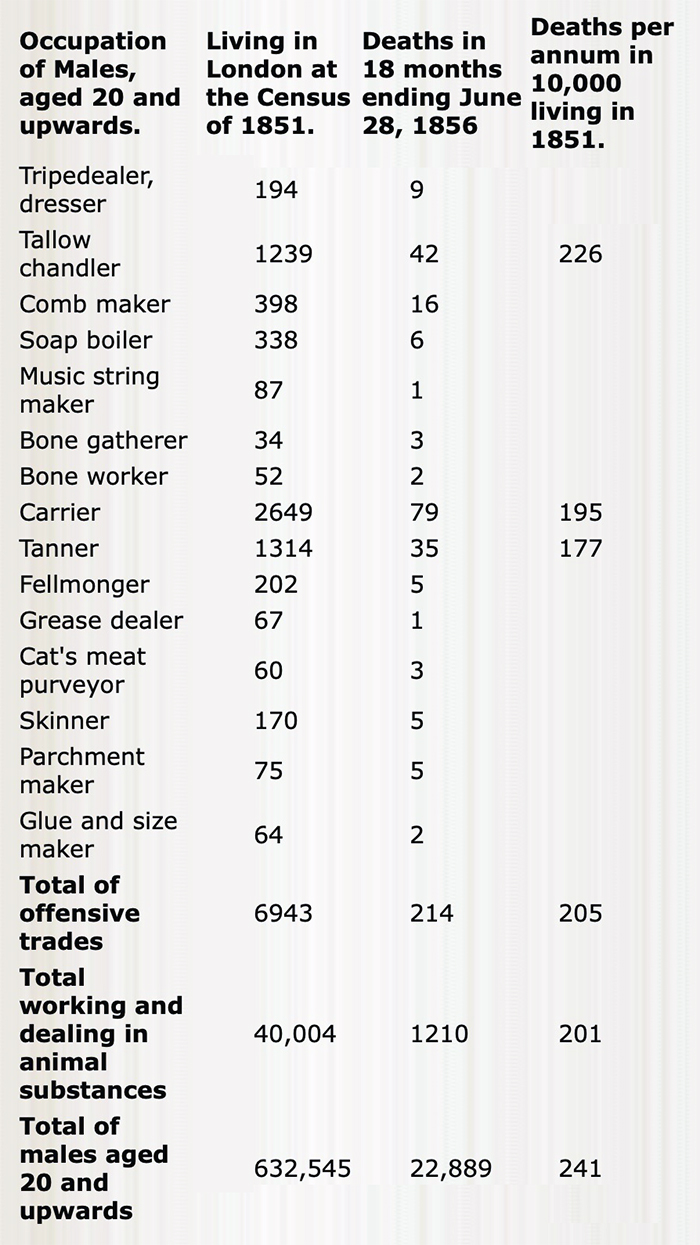
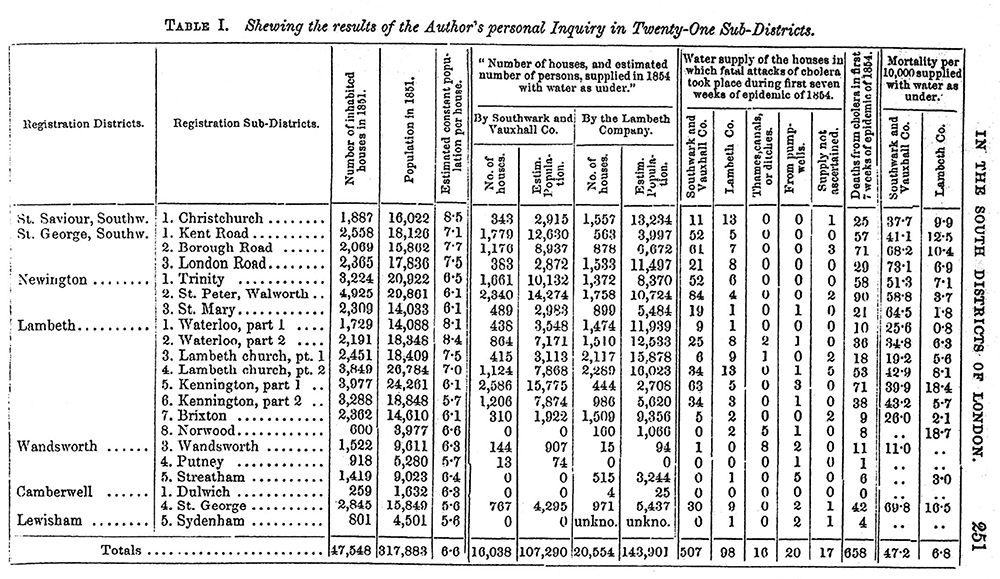
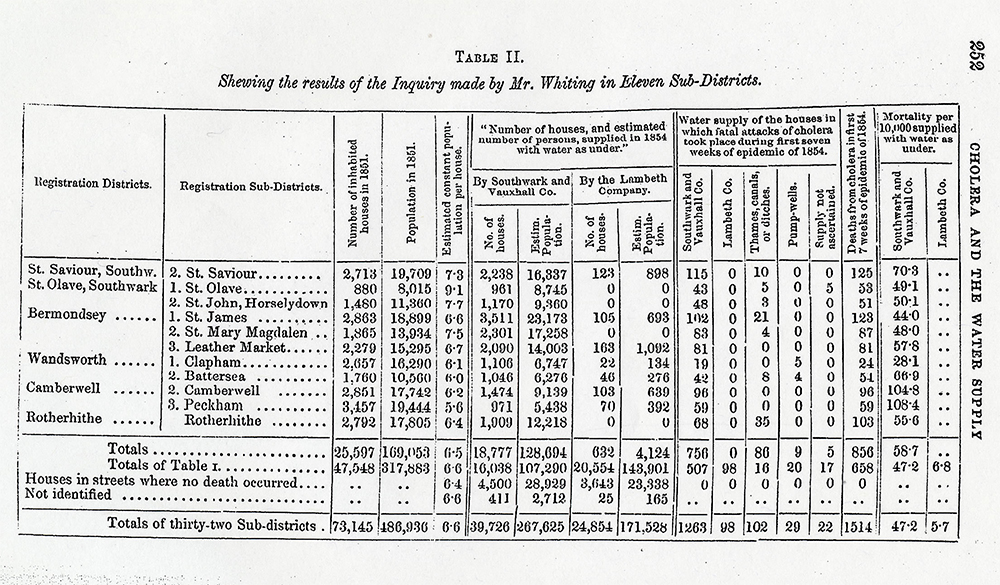
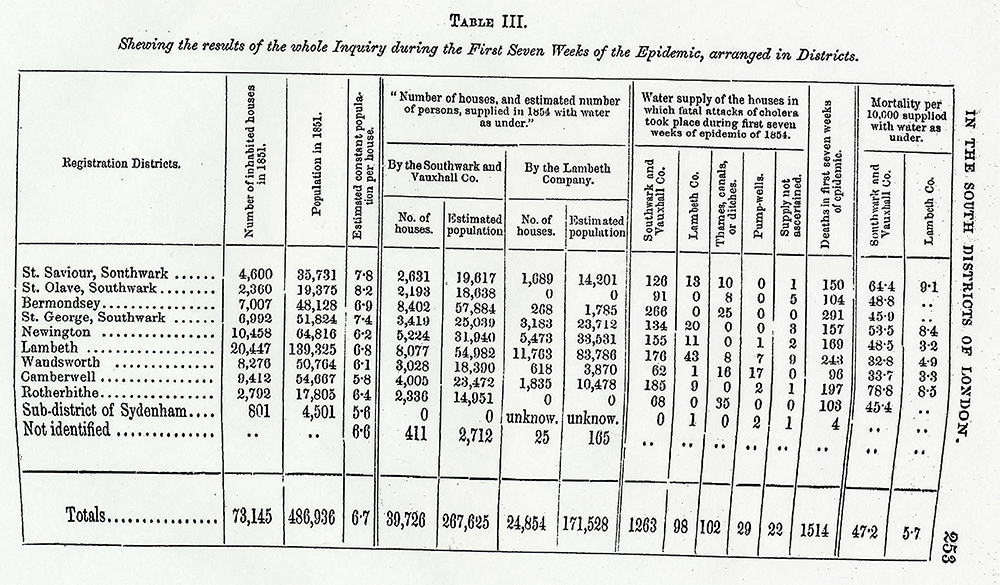
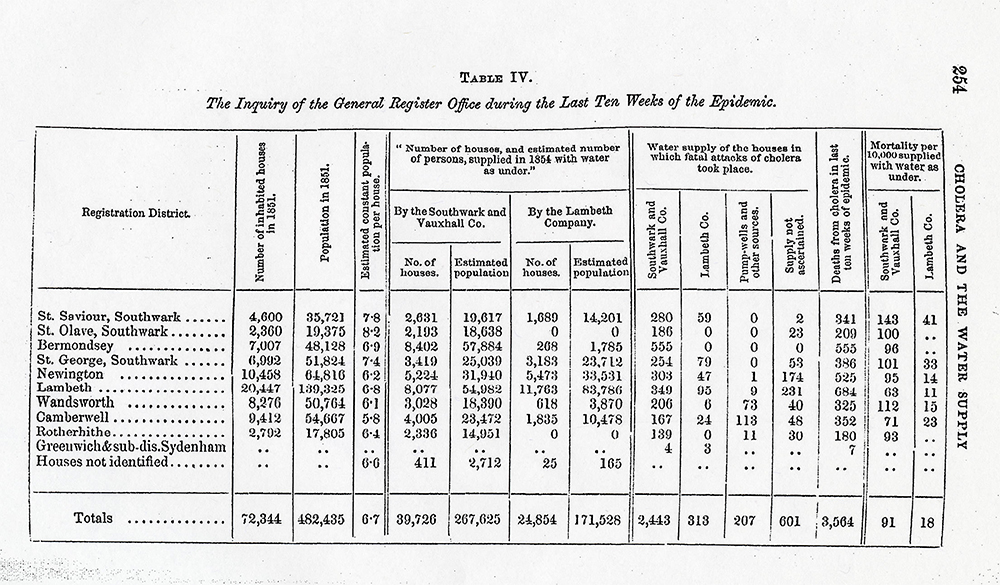
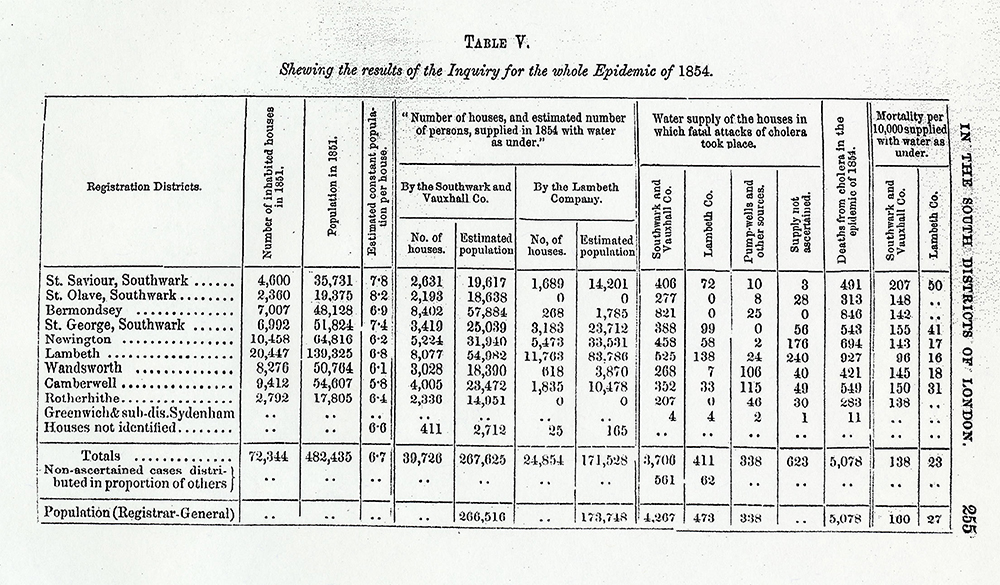
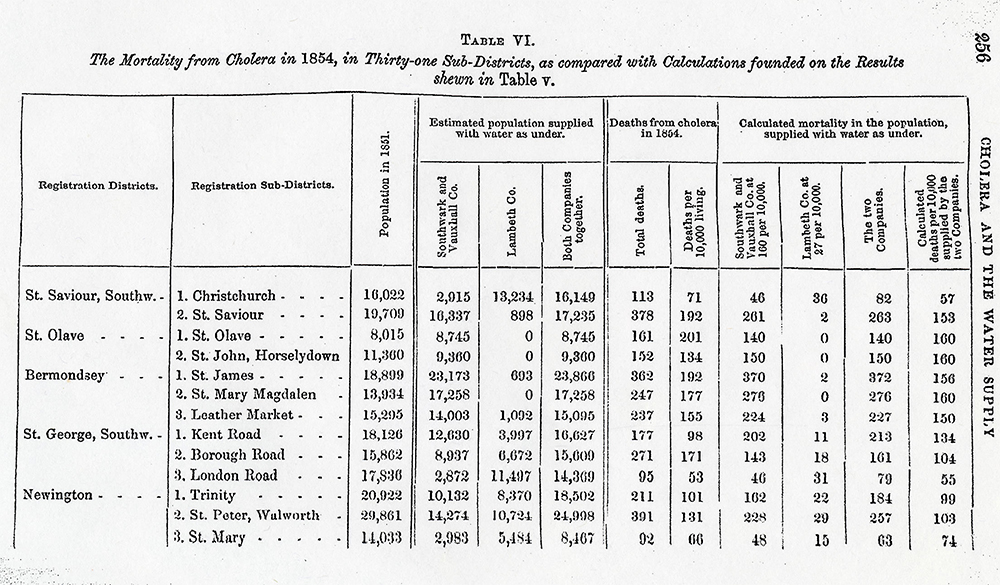
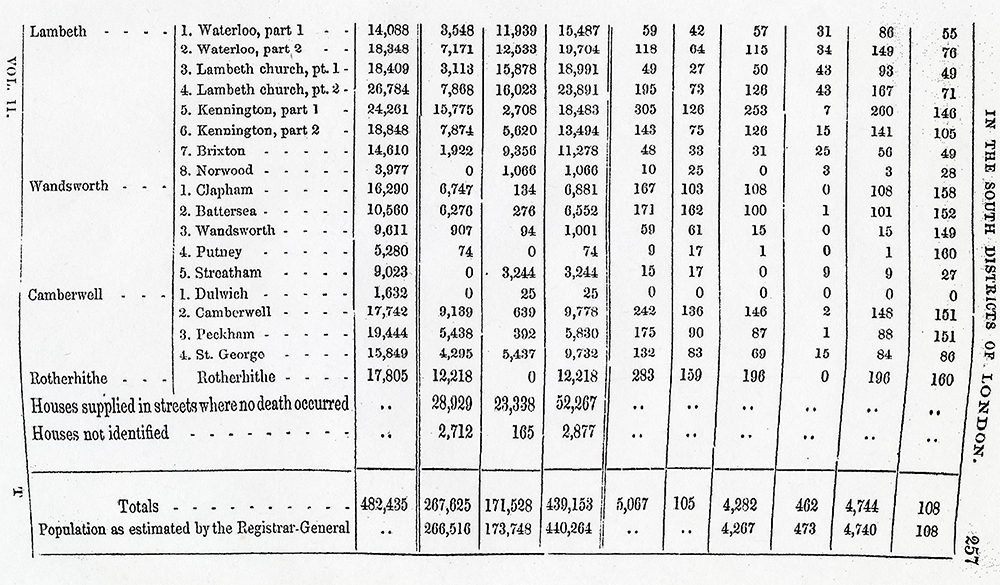
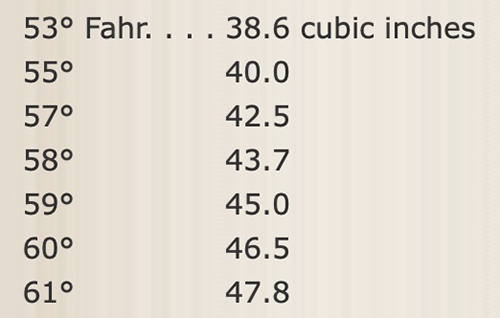
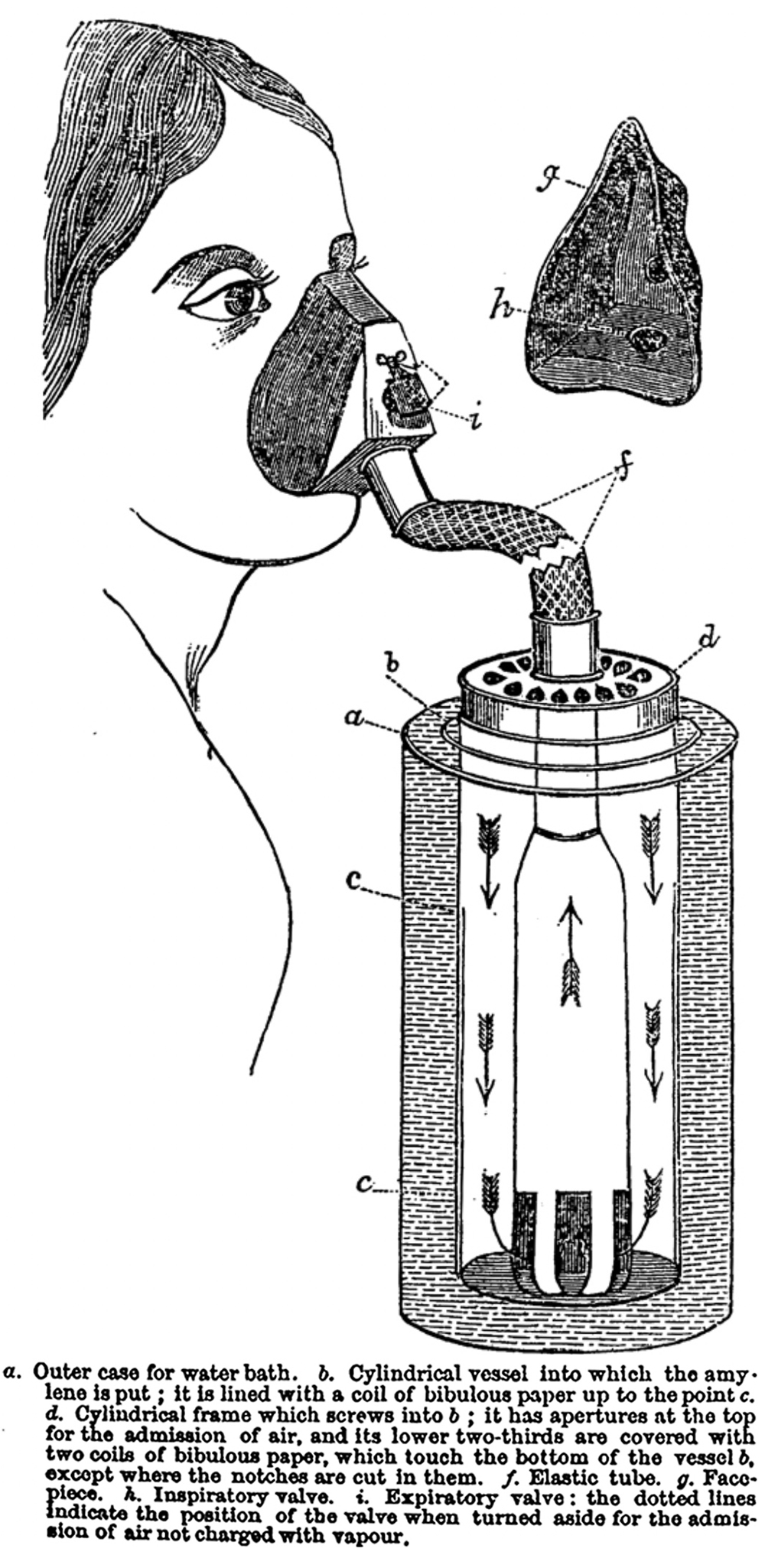
 (# 114-124)
(# 114-124)
