Source: Snow, John. Assoc. Med. Jour. 1, 10 June 1853, pp. 500-502.
76. "On the administration of chloroform during parturition"
By John Snow, M.D.
It is unnecessary now to employ or allude to any of the abstract reasons which have been given for using or withholding chloroform during labour, since a sufficient number of observations have been made to enable the question to be decided by experience. I believe that no one disputes the power of chloroform to relieve the sufferings attendant on parturition; and, therefore, the only consistent objection that can be made to it is, that some danger or disadvantage may arise from its use. It is well known that, out of the vast numbers of patients to whom this agent has been administered for the performance of surgical operations, a few have unfortunately died whilst inhaling it, or a minute or two afterwards; but it is satisfactory to know that no accident of the kind has happened in the practice of midwifery. This should not be looked upon as a mere coincidence, for there are sufficient reasons for concluding that there is no danger from the exhibition of chloroform during labour by a medical man using ordinary care, even though he may have had no previous experience in its employment. In the first place, the effect which it is necessary to produce in parturition is so much slighter than is required for a surgical operation, that it is not necessary to approach even half way to a point that would be dangerous if it were exceeded; and, in the next place, the chloroform never requires to be given except whilst there is pain, the relief of which serves as a sign for its discontinuance; which sign is not present in exhibiting it preparatory to the commencement of a surgical operation.
There have, however, been some cases in which death has been attributed by certain authors to chloroform, which had been administered during labour. Dr. Ramsbotham relates one such case;* but I doubt whether he would have considered the result to be due to this medicine, if he had had an extensive experience of its use, either in obstetric or any other class of cases.
(*Principles and Practice of Obstetric Medicine. Third edition, p. 169.)
The chloroform was given occasionally, and apparently very judiciously, during the last four or five hours of labour in this case. Dr. Ramsbotham relates that, at the conclusion of the labour, "the uterus contracted well, and the patient appeared comfortable. At the end of an hour and a half, however, distressing dyspnœa came on, attended with excessive lividity of the face, and all the signs of extensive engorgement of the lungs and heart. Her respiration became more natural under the means employed, and in three hours and a half she lay down to rest; but in half an hour she suddenly arose with a return of the most distressing dyspnœa: this was soon followed by convulsions, and almost immediate death." No inspection of the body took place.
A case somewhat similar to the above occurred in the practice of Dr. Murphy, who, however, does not attribute the fatal result to the action of chloroform.†
(† See Lectures on Parturition, p. 474.)
In this case, the chloroform was exhibited very sparingly during the last two hours of labour, the patient not being rendered unconscious. She fell asleep after the expulsion of the placenta, but awoke in two hours with cough and difficulty of breathing. These symptoms increased in spite of treatment, and the patient died a little more than twenty-four hours afterwards. The lungs were found to be greatly congested, and the kidneys were in a pretty advanced stage of granular degeneration.
Fatal congestion of the lungs is one of the results of Bright's disease. I have seen it in the male subject. It is not improbable that, in the case related by Dr. Ramsbotham also, there was either permanent disease or temporary congestion of the kidneys, and the toxemia existed in both cases. The occurrence of convulsions a little before death in the latter case renders this the more likely‡.
(‡ See Association Journal, January 21st, p. 64).
At all events, the symptoms in the above cases do not coincide in the least with the known effects of chloroform, even when exhibited much more freely. It must be remembered also, that the unfavourable symptoms did not commence till an hour or two after the effects of the chloroform had subsided; and in this time the system gets more thoroughly rid of this medicine than of a dose of opium in two or three days.
As chloroform is not a preventive of all the "ills that flesh is heir to", it might be expected that puerperal mania should happen after some few of the many cases in which it is used, especially as it has been inhaled more generally by sensitive and susceptible patients than by others. Dr. Ramsbotham alludes, in a foot-note,** to an attack of puerperal mania "which had supervened on the exhibition of chloroform"; but he does not state at what period the mania commenced; whether, for instance, it was an hour or a month after the inhalation.
(**Opus cit., p. 154)
Other cases, or possibly this same one, have been mentioned in the medical societies; but no particulars have been related. I have been told respecting one case of puerperal mania, that the patient had long been in the habit of inhaling chloroform very freely (taking it often when no one was present), to prevent attacks of epilepsy, to which she was subject.
It was said that, in some of the early cases in which chloroform was employed, the uterine contractions were so much enfeebled by it, that delivery had ultimately to be accomplished by use of the forceps. It is not improbable that the over free use of this agent might lead to such a result; but I believe it would not arise from its judicious use. It has happened that, in all the cases of manual and instrumental delivery in which I have given chloroform, it was exhibited only in consequence of the operation; for the other cases in which I have administered it have all terminated without artificial assistance.
The propriety and advantages of administering chloroform in parturition being admitted, a frequent inquiry is, "In what cases ought it to be employed?" It will be readily conceded that, in cases where the pain is not greater than the patient is willing to bear cheerfully, there is no occasion to use chloroform; but when the patient is anxious to be spared the pain, I can see no valid objection to the use of this agent, even in the most favourable cases. The benefits arising from chloroform in severe cases of labour are experienced in a lesser degree in favourable cases; and the patient may be fairly allowed to have a voice in this, as in other matters of detail which do not involve the chief results of the case. The determination of the kind of labours in which chloroform should be used or withheld is really a matter of not much importance, because, as we pass from cases that are severe and protracted to those which are short and easy, the quantity of chloroform that is used, and the amount of diminution of the common sensibility, and of interference with the mental functions, become so trifling, that very little remains about which to hold a discussion. Indeed, from what I have observed of the continued use of this agent in medical cases, and its use by healthy persons for experiment, I believe that the quantity which is inhaled in a short and easy labour might be continued daily for an indefinite period, without appreciable effect on the health.
The above remarks apply also in some measure to the question as to the period of the labour when the exhibition of chloroform should commence; for, in proportion as the pains are feeble, it must be more sparingly administered. The most usual time when the accoucheur and I have determined that the inhalation should be commenced, has been when the os uteri was nearly dilated to its full extent, and the pains were taking on an expulsive character. In many of the cases which I have attended, it has, however, been commenced much earlier; for the suffering caused by the dilating pains in the first stage of labour is often very great, and the chloroform is consequently of the utmost service when employed at this time.
As regards the manner of giving chloroform, I shall first allude to cases not requiring manual or instrumental assistance. In such cases, when it has been determined to resort to inhalation, the moment to begin is at the commencement of a pain; and the chloroform should be intermitted when the uterine contraction subsides, or sooner, if the patient is relieved of her suffering. It is desirable to give the chloroform very gently at first, increasing the quantity a little with each pain, if the patient is not relieved. The practitioner easily finds, with a little attention, the quantity of vapour which it is desirable to give at any stage of the labour, and in each particular case; his object being to relieve the patient without diminishing the strength of the uterine contractions and the auxiliary action of the respiratory muscles, or with diminishing it as little as possible. At first, it is generally necessary to repeat the chloroform at the beginning of each "pain"; but, after a little time, it commonly happens that sufficient effect has been produced to get the patient over one or two uterine contractions without suffering, before it is resumed.
When the practice of inhalation in midwifery was first introduced by Dr. Simpson, he very naturally adopted the plan which is usually followed in surgical operations, making the patient unconscious at once, and keeping her so to the end of the labour. It was soon found, however, by other practitioners, that this is not necessary; and indeed it would not be safe in protracted cases. Drs. Murphy and Rigby were, I believe, amongst the first to state that relief from pain may often be afforded in obstetric cases, without removing the consciousness of the patient; and I soon observed the same circumstance*.
(*London Journal of Medicine, vol. i, pp. 54, 976)
Some persons indeed have alleged that the pain of labour can always be prevented, without making the patient unconscious of surrounding objects; whilst others have asserted that no relief can be afforded unless unconsciousness be induced. But both these opinions are directly opposed to experience. There are comparatively few cases in which the suffering can be prevented throughout the labour without interfering with consciousness, although there are very many cases in which it can be in this way prevented in the early part of the labour. This difference depends in some measure on the constitution of the patient, but chiefly on the severity of the pain to be prevented. It is in accordance with what is observed in medical and surgical cases, that the pain should be removed in some instances without abolishing consciousness, and that in other instances it should not; for, in certain cases of neuralgia, the pain is so severe, that no material relief can be obtained by chloroform as long as consciousness is retained; and in surgical operations, although it now and then happens that the minor and concluding parts of an operation, such as tying vessels and introducing sutures, can be performed without pain, whilst the patient is consciously looking on, a free incision in the skin can hardly ever be made under similar circumstances without pain.
The external evidence of the uterine contractions continue as before, when the patient is rendered unconscious by chloroform; and the muscles of respiration are called freely into play, to assist the action of the uterus in the second stage of labour. The aspect of the patient under these circumstances, is generally that of one who is suppressing the expression of her sufferings; and any relative or friend who comes in without knowing that chloroform has been given, begins to praise the unconscious patient for her fortitude. On some occasions, indeed, there are groans and cries, as of suffering; but the mind being unconscious of pain, it can hardly be said to exist.
It may be remarked, that complete anæsthesia is never induced in midwifery, unless in some cases of operative delivery. The diminution of common sensibility to a certain extent, together with the diminution or removal of consciousness, suffice to prevent the suffering of the patient during labour; and she never requires to be rendered insensible as in a surgical operation, when the knife may be used without causing a flinch or a cry. The nerves of common sensation must be allowed to retain their functions to a certain extent during labour; otherwise the assistance of the respiratory muscles, which consists of reflex action, or "motion arising from sensation, without the aid of volition", would not take place, even if the contractions of the uterus should still continue.
The effects of chloroform on the brain should not be carried during labour beyond what I denominate the second degree of narcotism, or that condition in which the mental functions are diminished, but not altogether suspended, except when the effect of the vapour is associated with natural sleep. The patient under the influence of chloroform to this extent, has no longer a correct consciousness of where she is, and what is occurring around her, but is capable of being aroused to give incoherent answers, if injudiciously questioned. In this state, the patient will sometimes assist the labour by bearing down voluntarily, if requested to do so, and be otherwise obedient to what is said; and by withholding the chloroform for a few minutes, she at any time becomes quite conscious. As a general rule, it is desirable not to hold any conversation whilst the patient is taking chloroform, in order that her mind may not be excited. The plan mentioned above, of giving the chloroform very gently at first, also has a tendency to prevent its causing mental excitement, the patient coming gradually under its effects. In surgical operations, excitement of the mind can nearly always be avoided by carrying the patient pretty rapidly into a state of insensibility, in which the mental functions are necessarily suspended. But in the practice of midwifery, it is not allowable to cause a state of coma or insensibility, except in certain cases of operative delivery, hereafter to be mentioned.
I nearly always employ, in obstetric cases, the inhaler that I use in surgical operations†.
(†This plan has been described, Med. Gaz., vol. xlii, p. 843)
There is not the same necessity for an accurate means of regulating the proportion of vapour in the air which the patient is breathing during labour, where but a trifling amount of narcotism requires to be induced, as in surgical operations, where a deeper effect is necessary; still I find the inhaler much more convenient of application than a handkerchief, and it contains a supply of chloroform which lasts for some time, thereby saving the trouble of constantly pouring out more. When I do administer chloroform on a handkerchief during parturition, I follow the plan I recommended in a former communication on this subject,‡ of putting only about fifteen minims of chloroform on the handkerchief at one time.
(‡Lond. Journ. of Med., vol. i, p. 54. It should be recollected that minims of chloroform are very different from drops; two minims being equal to nine drops from the lip of a small phial.)
The quantity of chloroform administered during any one pain, never exceeds a very few minims; but the quantity used in the course of a protracted labour is often considerable. Two ounces and a half by measure is the largest amount I have used in one case; but as the apparatus was used, this quantity would go as far as seven or eight ounces employed in the most careful way on a handkerchief. I have not kept any patient continuously unconscious for more than two hours; and eight hours is the longest time I have had to administer chloroform in any case, but it has been continued for a much longer period without ill effects, by Dr. Simpson and others.
Chloroform can be best applied when there is an additional medical man, who has not to attend to the ordinary duties of the accoucheur; but it can be given very well by the accoucheur himself, so as to save the greater part of the suffering of labour; although he perhaps cannot always administer it in the perfect way in which he could, if he had no other duties to divide his attention.
It is probable that the use of chloroform has no particular influence over the duration of labour, in the whole number of cases in which it is employed; but individual labours are occasionally either retarded or quickened by it, according to circumstances. In some cases, the chloroform, even when very moderately employed, diminishes both the strength and the duration of the uterine contractions, and prolongs the interval between them, thereby making the labour somewhat longer--a matter of no consequence, however, as the patient is not suffering in any way. In other cases, the inhalation causes the uterine action to become stronger and more regular, by removing the excess of sensibility by which it has been interfered with. This occurs more particularly in the first stage of labour. In some cases, also, the chloroform seems to act as a direct stimulant to the uterine contractions, increasing their force and frequency--a circumstance at which we need not be surprised, when we remember that both opium and brandy, in moderate quantity, often act in the same manner. Chloroform has also the effect of promoting the dilation of the os uteri in many cases, even when no rigidity exists; and when there is rigidity of the os uteri, the inhalation is of the utmost service, and shortens labour very much. This is the case, also, when there is rigidity of the perineum.
During delivery with the forceps, or by perforation, the chloroform requires to be administered very much in the same way as in ordinary cases. It must be given at each pain, so as to prevent the suffering of the patient without checking the uterine contractions. It generally, however, requires to be given a little more freely than in natural labour. Dr. Murphy has related three cases of delivery by the forceps, and one by perforation,* in which I assisted him, four or five years ago, by giving chloroform and Dutch liquid, which I was trying at the time.
(*Observations on Chloroform in Midwifery.)
The operations were chiefly undertaken on account of deformity of the pelvis; and the patients all recovered very favourably. I have given chloroform in only one case of midwifery in which the knife was used. It was a case of Dr. Murphy's, in which he had to make an artificial os uteri. Of course, under such circumstances the patient is made insensible at the time of operation.
When it is necessary to introduce the hand into the uterus to turn the child, the chloroform requires to be given in a pretty full dose, so as to suspend the uterine contractions; and as soon as the operation of turning is performed, the inhalation should be discontinued for a short time, to allow the action of the uterus to return, and assist in the expulsion of the child. In the autumn of 1849, I administered chloroform in a case of presentation of the shoulder, attended by Mr. French, of Great Marlborough Street, and in a case of presentation of the elbow, attended by Mr. Marshall, of Greek Street, Soho: the operation of turning was performed with singular facility in both cases, although the membranes had been ruptured, and the liquor amnii evacuated some time. The uterus afterwards contracted well in both cases, and expelled the placenta in a few minutes. In a case of natural presentation, in which turning was performed by Dr. Murphy, on account of narrowness of the pelvis, and the impossibility of applying the forceps, the introduction of the hand was difficult from want of space, but the uterus offered no resistance.
In other cases in which it is necessary to introduce the hand into the uterus, chloroform is of equal service. On Dec. 26, 1850, I was requested by Mr. Cooper, of Moor Street, Soho, to assist him in a case of retention of the placenta. The patient had given birth to a child two hours before, and Mr. Cooper had introduced his hand, but had been quite unable to bring away the placenta, on account of firm contraction of the uterus, in a sort of hour-glass form. On the chloroform being administered, the hand was easily introduced, and the placenta detached and extracted. There was very little hæmorrhage. I may here state that I have seen hæmorrhage, to any considerable amount, in only one case in which I have given chloroform, and the patient had suffered from it in some of her previous confinements.
It is often asked, whether the chloroform has any effect on the child. It is quite certain that the fœtus must receive a portion of the chloroform into its circulation, as it does of any other medicine which is absorbed into the blood of the mother; and when sulphuric ether was the agent employed, its odour could be perceived in the child's breath after birth. The fœtus must therefore be influenced by the chloroform, though generally to a less extent than its mother, as it receives its dose only at second-hand. It has seemed in some cases that the child was less acutely sensible to the cold air than usual at the time of birth; and when the mother is unconscious from chloroform, I have not seen it kick and scream in the violent way, and grasp the bed clothes with the force, during the first minute after its birth, that is often observed under other circumstance. With these exceptions, no effects of the chloroform on the child can be perceived.
18, Sackville Street, June 1st, 1853.
Return to John Snow Publications
Source: Snow, John. Med. Times and Gazette 7, 8 October 1853, pp. 367-369.
77. "On the prevention of cholera."
By John Snow, M.D.
We cannot hope to prevent any disease unless we have a correct knowledge of its causes. As regards the cholera, many persons, indeed, consider that its causes are well-known, and also the means of its prevention; and they attribute its continued existence and extension entirely to neglect of the requisite measures for its suppression. Every candid observer must admit, however, that a great deal has been done within the last twenty years in the way of presumed sanitary improvement, much of it with the best results as regards the general health of the community, and all of it with the best intentions. Yet the cholera of 1849 was much more fatal than that of 1832, and now, on its third visit to our shores, it is prevailing to a more fatal extent in Newcastle than was ever before witnessed in this country. These circumstances clearly show, that the causes of cholera are not generally well understood, and that the true preventive measures have not been applied.
The first origin of cholera, like that of other epidemic disease, is hid in obscurity, and will probably remain so. It has been proved, however, by various documents quoted by Mr. Scot,* that cholera was prevalent at Madras in 1769, and that it carried off many thousands of persons at various places in the peninsula of India from that time to 1790.
(*Report on the Epidemic Cholera. 1824. P.5.)
From this period we have very little account of the disease till 1814, although, of course, it might exist in many parts of Asia without coming under the notice of Europeans. In June, 1814, the cholera appeared with great severity in the 1st Bat. 9th Regt. N.I. [Native Infantry], on its march from Jaulnah to Trichinopoly, while another battalion which accompanied it did not suffer, although it had been exposed to exactly the same circumstances, with one exception. Mr. Cruikshanks, who attended the cases, and made a report thereon, writes as follows:--
"It was the belief of the natives, strenuously fostered and inculcated by their spiritual guides, that the epidemic was the immediate consequence of the wrath of Heaven, outraged and insulted by the pollution of certain sacred tanks, situated at the village of Cunnatore, in which sepoys of low caste and camp followers had indiscriminately bathed. Such we may not regard as affording a very satisfactory solution of the difficulty; yet it leads, I think, directly to the true point of inquiry. At Cunnatore, the force was so encamped, that while the 5th Native Infantry on the right had their supplies of water from wells, the puckallies of the 9th Native Infantry procured water for that battalion from tanks situated on low ground on the left of the line. The fact, that the disease first broke forth in a day or two after passing Cunnatore; the prevailing opinion of the natives, that it originated there, and that somehow it was connected with the tanks; a desire to discover some one cause confined in its influence and operation to one out of the two battalions; lastly, the difficulty or impossibility of lighting on any other; all these led to inquiry, and to ascertaining with a considerable degree of certainty, that each battalion was supplied with water from a source distinct from the other."†
(†Op. Cit. P. 237.)
The cholera was said not be at Cunnatore at the time.
In 1817, the cholera prevailed with unusual virulence at several places in the delta of the Ganges; and, as it had not been previously seen by the medical men practising in that part of India, it was thought by them to be a new disease. At this time the cholera began to spread to an extent not before known; and, in the course of seven years, it reached eastward to China and the Philippine Islands, southward to the Mauritius and Bourbon, and to the north-west as far as Persia and Turkey. With its progress afterwards in Europe the reader is, no doubt, quite familiar. The cholera travels along the great tracks of human intercourse; it never attacks the crews of ships coming from a country free from cholera to one where the disease prevails till they have entered a port or had intercourse with the shore. Its exact progress from town to town and from country to country has not always been traced, but it has never appeared except where there has been ample opportunity for it to be conveyed by human intercourse. It is quite true, that personal communication cannot always be detected between the new cases and previous ones; but this is only what happens in small-pox, which is proved by inoculation to be a communicable disease. In an interesting account of an epidemic of variola at Corfu, Mr. Spencer Wells writes as follows:--"On the 27th of February, 1852, a case of small-pox occurred in the Jew's quarter at Corfu. Small-pox had been prevalent for some months on the opposite shores of Albania, which were only placed under a quarantine of observation of twenty-four hours. No communication could be traced between any infected person or object from Albania to account for the appearance of the disease in Corfu."‡ .
(‡ Medical Times, current vol., p. 83.) .
Innumerable instances are, however, observed of the communication of cholera by personal intercourse, and hundreds of them of the most convincing kind; as where the first case in a neighbourhood is that of a person newly arrived from a place where the disease was prevailing, and the next cases are those of members of his family or other who attend on him. There is, it is true, what has been considered the other side of the question. Numbers of persons come into near proximity with the sick without contracting the malady; but this only shows that it is not communicated either by contact with the patient or by effluvia given off into the surrounding air; and as there was no right to assume that these two modes, usually denominated contagion and infection, are the only ways in which disease can be transmitted from one person to another, the evidence of the communication of cholera remains unshaken to afford a full explanation of the progress of the disease; indeed, the only explanation of it that can be offered.
It only remains, then, that the mode in which cholera is communicated should be known, in order that the means of arresting its progress may be pointed out. Every disease communicated from one person to another is necessarily caused by some material proceeding from the former and received by the latter. Now, if cholera were one of those disorders which are ushered in by general symptoms, such as fever, we should have no indication of the channel by which the morbid poison is received, whether, for instance, by the alimentary canal, by the lungs, or in some other way, but should be left to determine this point by circumstances unconnected with the pathology of the disease. Cholera, however, always commences with disturbance of the functions of the alimentary canal; all the early symptoms are connected with this canal, and the effects which follow are only the result of what has occurred in it. The exudation of the watery part of the blood into the stomach and bowels causes the faintness and sinking. The blood which remains in the vessels, being too thick to pass readily through the capillaries, both the pulmonary and systemic circulation are impeded; hence the difficulty of breathing, the general coldness, and state of collapse. How far the cramps depend on irritation of the nerves of the alimentary canal, and how far on the want of fluidity and proper circulation of the blood is not very evident; but it is quite certain that they do not depend on any cholera poison circulating in the blood, for the cramps and all the symptoms of collapse disappear for a time on the injection of a weak saline solution into the veins, which merely replaces what has been lost by the bowels. It is evident from this circumstance that the blood is not poisoned in cholera, except in cases of secondary illness, when it becomes charged with urea and other excretory matters, owing to congestion of the kidneys. The primary and essential morbid actions of cholera being confined to the alimentary canal, it follows that the materies morbi of cholera must find access to it by being swallowed, that it must increase and multiply there, and be discharged to be a source of danger to others.
Before pointing out the precautions which these views suggest, it will be well to examine what light they throw on the progress of cholera, and what confirmation they receive from general and particular facts connected with its history. It has been observed, in all parts of the world, that nothing assists the spread of cholera more than want of personal cleanliness. When we consider how free the evacuations from the stomach and bowels of cholera patients often are, both from colour and odour; how suddenly and copiously, and with what force they are generally discharged, it is evident that the hands, both of the patient and his attendants, are liable to be soiled with them. Unless great care is taken to wash the hands frequently, the more especially before taking food, or handling and preparing the food of others, small quantities of the evacuations must necessarily be accidentally swallowed. The influence of dirty habits in aiding the spread of cholera is thus clearly accounted for. It is analogous to what occurs among house-painters in regard to lead-poisoning. Those of cleanly habits escape; while others constantly swallow a little paint with their food, and become affected with colic. The scarcity of water, of course, is an obstacle to cleanliness, even when the inclination prevails; and this has been frequently observed to be connected with the unusual extension of cholera in a town or neighbourhood. The reason why Medical men, and other persons of cleanly habits, who do not stay to eat and drink in the sick room, are scarcely rendered more liable to cholera by their avocations, while it often fares differently with the social visiter, is perfectly explained by the above views. It is evident, also, why the Medical man can make inspections of the dead bodies of cholera patients with impunity; while they who wash and lay out the body often suffer. The Medical man is certain to wash his hands after his operation, while the persons who perform the other offices mentioned, especially among the poor, are almost as certain to neglect that duty. It is obvious that, where a whole family live, night and day, in one small room, in which the cooking is done and the meals are eaten, that the food is very liable to become contaminated, in the event of a case of cholera occurring; and, where several families live in one room, the risk amounts almost to a certainty. Now, under these circumstances, cholera is observed to spread through the family and household; while cases occurring among the well-to-do, who have separate kitchens and sleeping-rooms, are seldom observed to spread the disease. The great havoc which cholera has made in certain asylums for pauper children and pauper lunatics, to which it has gained access, is explained by the crowding which existed, and more particularly by the difficulty of maintaining cleanly habits among these classes of persons. On the other hand, the almost total escape of the inmates of the model lodging-houses in 1849, although inhabited by a class of persons who usually suffer more than others, was due to the excellent arrangements for cleanliness, and the proper separation of apartments and offices required for distinct purposes. About a month ago, certain German emigrants, on their way to America, who had crossed the sea from Hamburg and Rotterdam, where cholera was prevailing, to the port of Hull, and had gone thence by rail to Liverpool, were seized with cholera (some of them fatally) in the latter town; and it is most likely to the well-regulated Emigrant's Home, in which these cases occurred, that the town of Liverpool owes its present freedom from the epidemic.
The colliers of this country suffered much more from cholera than persons in any other occupation whatever, both in 1832 and 1849,--a circumstance which can only be explained by the mode of communication of the malady above pointed out. Pitmen are differently situated from every other class of workmen in many important particulars, as the following reply, which I received a few days ago from the agent to a colliery near Leads will show:--"Our colliers descend at five o'clock in the morning, to be ready for work at six and leave the pit at from one o'clock to half-past three. The average time spent in the pit is eight to nine hours. The pitmen all take down with them a supply of food, which consists of cake, with the addition, in some cases, of meat, and all have a bottle, containing about a quart of 'drink.' I fear that our colliers are no better than others as regards to cleanliness. The pit is one huge privy, and of course the men always take their victuals with unwashed hands." It is very evident, that when a pitman is attacked with cholera while at work, the disease has facilities for spreading among his fellow-labourers such as occur in no other occupation. That the men are occasionally attacked while at work I know, from having seen them brought up from some of the coal-pits in Northumberland in 1831-2, after having had profuse discharges from the stomach and bowels and while fast approaching to a state of collapse.
It is not only when the cholera evacuations are accidentally swallowed in small portions with the food that they have the power of propagating the disease, but also when they are diffused in a very large quantity of water. On former occasions* I adduced several instances in which a violent irruption of cholera in a limited community was caused by the contamination of the water of a well or tank by the contents of drains and cesspools, when there were cholera evacuations in the latter,--instances in which irruptions of cholera among greater numbers of people were connected with a similar contamination of the tidal ditches of Rotherhithe and Bermondsey,--and instances in which whole towns were, more or less, affected by drinking the water of rivers into which the sewers discharged their contents. It was shown that, in the latter case, more particularly when the water was distributed by water-works, the cholera, instead of creeping along in the back streets, and courts, and alleys, inhabited by the poor, became generally diffused among all classes of the community.
(* Medical Gazette, 1849. Vol. II, pp. 730, 745, 923; and Medical Times, 1851. Vol. II, pp. 559, 610.)
This circumstance has just received a fresh illustration at Newcastle and Gateshead.
The Water Company, formed about six years ago for the purpose of supplying these two towns with water from a rivulet and springs at Whittle Dean, about ten miles distant, have lately found their proper sources insufficient for the demands of the population and the various factories, and have been making use of the pipes of a former company to obtain water from the Tyne, at a spot about a mile above the towns. The tide, however, flows for several miles further, and, consequently, carries the sewage past the place where the water is obtained. When the cholera became established in Newcastle, in the early part of the present month, the sewers necessarily conveyed the peculiar evacuation of the disease into the river, and for some days the deaths from cholera increased in a geometrical ratio,--being, on the 13th, 29; 14th, 59; 15th, 101; and they increased in Gateshead in the same proportion. Complaints of the impure state of the water were now more loudly expressed than before; and on this day the Tyne water was discontinued, and the mortality no longer increased in the same frightful manner. It kept at this point, and even a little above it, for a few days, however, before it began to decrease, perhaps on account of impurities still remaining in the pipes and in the cisterns where the latter are used. Besides, it must be borne in mind, that the disease might maintain, by its ordinary means of propagation, the wide dominion it had obtained through the aid of the steam-engine and pipes of the Water Company. The cholera on this occasion has been very fatal among the genteel and well to do classes in all parts of Newcastle and Gateshead, as well as among the poor. Only a few streets in these towns are situated at a low level, for the banks rise very abruptly at a little distance from the river on both sides. A great portion of each town is elevated nearly 200 feet above the river, and some parts are nearly 300 feet high, yet the Water Company above mentioned supplies all these districts, and all have been visited severely by the cholera. The diminished mortality which is taking place now (September 27) is chiefly confined to the lower parts of the two towns. I have obtained the above particulars from a medical friend in Newcastle, and also from the published reports of the meetings of the Town Council and other public bodies.
In 1831-2 there were no waterworks in Newcastle. It was supplied in an insufficient manner with spring water, which generally had to be carried some distance to the houses from "pants" in the streets. The epidemic cholera was pretty severe at this time. In 1849 Newcastle and Gateshead were plentifully supplied with water unpolluted with sewage, by the Company above-named, who had then no occasion to have recourse to the Tyne. At this period these towns escaped with a very slight visitation from cholera. The existing epidemic, under the circumstances above narrated, has carried off more than six times as many persons in Newcastle during the first four weeks of its presence, as it carried off in a similar period in 1831-2; and more than twice as many in Gateshead.
The absence or deficiency of drainage and the overflowing of cesspools promote the spread of cholera, as of typhoid fever, by permitting the evacuations of the patients and the water in which soiled linen has been washed to flow on the surface, and contaminate everybody who comes in contact with them; but the want of proper drainage is often still more injurious, by causing the liquids which ought to be carried
off to saturate the ground, and percolate into the pump wells and other supplies of water.
The measures for the prevention of cholera which are suggested by the circumstances and views above detailed, may be divided into those which can be carried
out in the presence of the epidemic, and those which, as they require time, should be taken beforehand.
The measures that should be adopted during the presence of cholera are:--
1st. To take care that there is a hand-basin, water, and towel, in every room where there is a cholera patient, and to take care that they are used by the nurse and other attendants,
more particularly before touching any food.
2nd. To immerse the soiled linen of the patient and his bed in water as soon as it is removed, until such time as it can be washed, lest the evacuations should become dry, and be wafted
about as a fine dust.
3rd. To take care that the water employed for drinking, cooking, and preparing food, (whether it comes from a pump-well, or is conveyed by pipes,) is not contaminated
with the contents of cesspools, house-drains, or sewers; or, in the event that water free from suspicion cannot be obtained, to have it well boiled and, if possible, also filtered.
4th. When the cholera prevails very much in the neighbourhood, to have all the provisions which are brought into the house well washed with clean water, and exposed to a temperature of at least 212º Fahr., or to make them undergo at least one of these processes.
5th. When a case of cholera appears among persons living in a crowded room, the healthy should be removed to another apartment where it is practicable, leaving
only those who are useful to wait on the sick.
6th. As it would not be practicable to clean out coal-pits and establish privies and lavatories in them, or even to provide the means of eating a meal with anything like common decency, when the cholera makes its appearance, the time of working should be divided into periods of four hours instead of eight, so that the pitman might go home to their meals, and be prevented from taking food in the mines.
The measures which can be taken beforehand to provide against a visitation of cholera, are,--
7th. To effect good and sufficient drainage.
8th. To provide the inhabitants with an ample supply of water, which is quite free from contamination with the contents of sewers, cesspools, and house-drains, or the refuse of people
who navigate the rivers.
9th. To provide model lodging-houses for the vagrant class, and sufficient house-room for the poor generally.
10th. To inculcate habits of personal and domestic cleanliness among the people everywhere.
The advice and direction which are issued respecting cholera by authority, are directed almost entirely against dirt and nuisances; but, unfortunately, they are perfectly silent respecting that particular kind of dirt which does the mischief. The Board of Health directs its attention more particularly to offensive effluvia, as a supposed cause of cholera. When the ready means for the communication of this disease exist, it often happens, for very evident reasons, that offensive gases are not altogether absent; but it has been satisfactorily proved, that the effluvia arising from the decomposition of vegetable and animal matters have nothing whatever to do with cholera.
The communicability of cholera ought not to be disguised from the people under the idea that the knowledge of it would cause a panic, or occasion the sick to be deserted. English people would not desert their friends or relatives in illness, though they should incur danger by attending to them, but the truth is, that to look on cholera as a "catching" disease which one may generally avoid by a few simple precautions, is a much less discouraging opinion than that which supposes it to depend on some mysterious state of the atmosphere in which we are all of us immersed and obliged to breathe.
18, Sackville-street.
Return to John Snow Publications
Source: Snow, John. Med. Times and Gazette 7, 5 November 1853, pp. 485-86. [Letter to Ed.].
78. "The late deaths from chloroform."
To the Editor of the Medical Times and Gazette
Sir,--The late deaths from chloroform, occurring nearly at the same time in different public institutions, have naturally attracted considerable attention; and they seem to call for some inquiry, whether means may not be adopted to prevent such accidents, or, at all events, render them of more rare occurrence. In concluding his account of the late fatal case at St. Bartholomew's Hospital, your reporter says:--"It is mournful, indeed, to consider, that, from cases such as the last three or four which it has been our lot to record, the practical surgeon gains no knowledge calculated to authorise the hope, that in future the like tragedies will be of less frequent occurrence." The case at St. Bartholmew's Hospital might at first sight seem to justify and require these observations, for the chloroform was administered by a medical man of eminence appointed to the duty, and in the constant habit of performing it. The vital organs of the patient were all sound, and she had taken the chloroform before without ill effects. There are circumstances, however, which lead me to a different conclusion from that of your reporter.
When the air a person breathes does not contain more than 4 or 5 per cent of vapour of chloroform, insensibility is induced very gradually; and I have found in numerous experiments on animals, that when vapour of this strength is continued till they are destroyed, death takes place very slowly. The breathing first becomes embarrassed, and then ceases; but the heart continues to beat for one or two minutes afterwards. During this interval, the animal can be easily restored by artificial respiration; and it often happens that, when the action of the heart is about to cease, the animal makes a gasping inspiration or two, which renew the circulation and cause spontaneous recovery if the chloroform is not continued. On the other hand, when animals are made to breathe air containing 8 or 10 per cent or upwards of chloroform, death takes place very quickly, and the circulation of the blood is arrested at the same time as the breathing, and, indeed, in some cases, before the breathing. A very few inspirations of air, containing 10 per cent of vapour of chloroform, have the effect of paralysing the heart, as I ascertained by giving chloroform to rabbits, by means of artificial respiration, after the chest was laid open.*
(*See London Journal of Medicine, April, 1852.)
Now, on examining the history of all the recorded cases of death from chloroform, it is ascertained, that the fatal event did not arise, in any instance, from the too long administration of vapour sufficiently diluted with air. In all the cases, the circulation has been arrested by the immediate action of the chloroform, owing to the circumstance, that the air which the patient was breathing just before he died or became moribund, has been too highly charged with vapour. It is evident, therefore, that the first consideration in giving chloroform should be, to take care that the vapour contained in the air which the patient is breathing shall at no time much exceed five per cent. So far from this being the case, however, it is seldom that any thought is taken of the quantity of vapour in the air breathed by the patient. It is generally considered sufficient to know that the patient has enough air to support respiration; and, indeed, the chloroform is usually given in such a manner that no knowledge is obtained, and no command exercised over the proportion of vapour in the air. This is certainly the state of matters when the chloroform is given on a handkerchief, or piece of lint; and I believe that the kind of inhaler used at St. Bartholomew's Hospital affords no means of either knowing or regulating, even approximately, the proportion of vapour in the air which the patient inhales. The chloroform may appear to be administered with it exactly in the same manner, when the process is, in fact, very different. So far, therefore, from having no hope that accidents from chloroform will be of less frequent occurrence, we have every reason to conclude that, with additional pains and attention, they may be almost, if not altogether, prevented.
Some persons direct their attention too exclusively to the pulse while giving chloroform. If the vapour were sufficiently diluted with air it would exert no great influence over the pulse, even if it were continued till the breathing should cease; and if it were not sufficiently diluted it might stop the pulse suddenly, without previous warning, when the information would come too late. The pulse is, therefore, but of secondary importance, as an indication of the effects of chloroform. The breathing, and the state of the eyes and eyelids, afford the best indication of the condition of a patient under chloroform; but there is no particular occasion for going into detail on this subject at present; for it does not appear that any accident has happened from the practitioner misunderstanding the state of the patient, and going on too long. The cause of accident has always been, that the vapour, being too strong, has acted so quickly, that there was not time to judge its effects.
While I do not participate in the melancholy forebodings of the writer who has reported the case in last week's Medical Times and Gazette, I cannot concur in the opinion of those who think that giving chloroform for a surgical operation is a very trifling matter, requiring no particular skill; and that it is merely necessary to spill a quantity of the agent on a towel or handkerchief, and make the patient quickly insensible. It is quite true, that this mode of proceeding answers in a great number of cases without any ill result; but it is attended all the time with some amount of risk, and the patients should be considered rather to escape from danger than not to incur any. In certain patients, the amount of chloroform which must be absorbed at one time, to prevent pain, and keep them from struggling during an operation, is not very far short of what would cause death; and, in nearly all cases, a larger amount of chloroform must be used than would be fatal, if it were taken too quickly.
It is obvious, therefore, that the exhibition of chloroform in operations must always be a process of some delicacy, and requiring care. With due skill and attention, however, there is every reason to conclude that the danger from chloroform may either be altogether abolished, or reduced to an amount too small to be estimated.
All the chief organs were found to be in a healthy state in the patient who died in the Royal Infirmary of Edinburgh, as well as in the patient at St. Bartholomew's. In the case at University College Hospital there was fatty degeneration of the heart. This, however, is a very common affection; and many patients who have all the signs of it, as far as they are known, undergo the effects of chloroform without ill consequences. On reviewing the recorded cases of death from chloroform, now between thirty and forty in number, the patients appear to have possessed an amount of health and strength quite on average with the multitude who have taken chloroform in operations with the best results. Consequently, the condition of the patient has not been the chief cause of accident. It should still, however, be a matter of attention, not so much in order to prohibit the chloroform, as to use, if possible, additional care; for a patient with diseased heart, would undoubtedly have a less chance than others to recover from an overdose of chloroform, should he unfortunately be submitted to it. When a patient liable to syncope, with weak or intermitting pulse, and arcus senilis of the cornea, requires to undergo an operation of any consequence, there would probably be as much danger from the pain and mental disturbance accompanying it, as from chloroform carefully administered. In such cases, I take care to carry the effect of vapour no further, and to keep it up no longer, than is imperatively necessary; and if the operation, on account of its being about the mouth, require to be performed in the sitting posture, I have the patient placed horizontally immediately afterwards.
I am, etc.
18, Sackville-street, Oct. 31.
John Snow.
Return to John Snow Publications
Source: Snow, John. Times 11
November 1853, p. 8, column D, [Letter to Ed.].
79. "The water supply at Newcastle."
To the Editor of the Times.
Sir,--I shall be obliged if you will allow me to make a few remarks on the letter of Mr. Main, in the Times of this morning. I feel assured that the Registrar-General did not make his forcible observations on the influence of the impure water supply of Newcastle and Gateshead, during the late epidemic of cholera, on insufficient grounds, and that he will be able to substantiate them, if necessary, when the period arrives for another quarterly report. In the meantime, however, the subject is one which may affect the lives of thousands in other towns; and the impression which the letter of your correspondent is likely to make on those who are unacquainted with the history of cholera and the details of the late epidemic at Newcastle ought not to remain unchecked.
Except in speaking of one place--Greenhow terrace--the secretary of the water company groups cholera and diarrhœa together, and says nothing whatever of the deaths. He informs us, for instance, that in the union workhouse, supplied with the company's water, there were 48 cases of cholera and diarrhœa out of 540 inmates; and that in the barracks, supplied with spring water, 415 cases of diarrhœa occurred among 519 inmates. All this I believe is true; but there are some important facts not included in the above statement. I have been informed, on good authority, that 10 persons died of cholera in the union workhouse--a high mortality in such a limited number of persons; while in the barracks there was no death, no case of cholera, and no person seriously ill. The circumstance of 415 soldiers consenting to take a dose or two of pleasant cordial medicine for diarrhœa is certainly not without interest, but has little to do with an inquiry like the present. If anything worse than this had happened to the customers of the Water Company, their secretary would hardly have felt called upon to write an apology.
Mr. Main expresses some regret for the necessity, as he terms it, of obtaining water from the Tyne in the neighbourhood of the sewers, and speaks of a desire on the part of the company to do better in the future; but, according to the figures he has adduced, he has no grounds for these sentiments. His numbers prove too much; they make it appear that there was less cholera and diarrhœa in houses supplied with the Tyne water, so much complained of by the inhabitants both for its colour and flavour, than in houses supplied with good spring water. According to the table Mr. Main has introduced, there were 28 cases of cholera and diarrhœa in the houses supplied with the company's water in certain streets he mentions, these 28 cases being 19 per cent of the inhabitants. In the other houses in the same streets which were supplied with spring water there were seven cases, which are 15 per cent of the 45 inhabitants. But it is not so stated; for another place, named Greenhow-terrace, in the outskirts of the town, and not supplied at all by the company, is added to the houses in which spring water is used, and by this means the cases are made to reach 28 per cent of the inhabitants.
If Mr. Main had told his readers the number of cases of cholera, or still better, the number of deaths from cholera in houses supplied by the company and with spring water respectively, the information, though very limited, might have been of some service; but the figures he has given are of none. He states that Dr. Waller Lewis abandoned his inquiry into the relative effects of different kinds of water, frankly stating he could make nothing of it. I cannot conceive that an inquiry of this nature, if carefully and properly conducted, would be without results of some kind; and I trust that the medical profession in Newcastle will take it up, and conduct it to its conclusion. They are quite competent to make this inquiry without assistance either from the General Board of Health or the water company. The inquiry is not one of mere local interest; it is connected with a more important point in the propagation of cholera, and is therefore of interest to all mankind.
It is little to the purpose that certain places in the neighbourhood of Newcastle and Gateshead, to which the supply of the water company does not extend, have been severely visited by cholera. There have doubtless been causes for this. No one supposes either that water is the only medium for the propagation of cholera, or that the Tyne is the only water capable of being contaminated with the contents of drains and cesspools. Spring water has often been thus adulterated by some accidental leakage in time of cholera, with very fatal results.
The fatality of cholera, in all the three epidemics which Newcastle and Gateshead have suffered, has borne a close relation, inversely, to the purity and abundance of the water-supply, and there is nothing in the communication of Mr. Main to indicate that a minute and detailed inquiry throughout these two towns would overthrow the conclusion which naturally flows from these general facts.
I am, Sir, your obedient servant,
John Snow, M.D.
Sackville-street, London, Nov. 10.
Return to John Snow Publications
Source: Snow, John. Med.
Times and Gazette 8, 25 Febuary 1854, pp. 180-182.
80. "The principles on which the treatment of cholera should be based."
By John Snow, M.D.
(Read at the Medical Society of London, January 21, 1854)
Without clear and definite ideas on pathology there can be no fixed principles of therapeutics; and the absence of any settled opinions respecting the nature of cholera is the cause of the various and contrary plans on which it is treated. It is, I believe, the more prevalent opinion, that the cholera poison acts on the whole system through the blood, and that the local symptoms are the effect of the general disease. In a paper I read to the Society, some time ago, on the mode of communication of cholera, I expressed my conviction that the cholera poison acts solely on the alimentary canal; but I did not enter on the consideration of the influence which this view of its pathology ought to have on the treatment of the disease.
In the greater number of epidemic, or what may be termed self-propagating diseases, the morbid poison appears to enter the blood in some way, and, after multiplying during a period of so-called incubation, it affects the whole system. Such is undoubtedly the case in small-pox, measles, scarlet-fever, and the various kinds of continued fever; but it must be remarked, that in all these diseases the illness always commences by general symptoms, as headache, rigors, fever, and lassitude; and the symptoms more particularly indicating the disease appear only afterwards. Cholera, on the other hand, commences with an effusion of fluid into the alimentary canal, without any previous illness whatever. Indeed, after this fluid has commenced to flow away as a copious diarrhœa, the patient often feels so little indisposed that he cannot persuade himself that anything serious is the matter. There are some cases, it is true, in which dizziness, singing in the ears, faintness, and a sense of sinking and uneasiness in the abdomen occur before any discharge makes its appearance from the alimentary canal; but this is just what happens in certain cases of hæmorrhage into the bowels, where all the symptoms of loss of blood are felt some hours, it may be, before that fluid makes its appearance in the stools. It is contrary to all analogy that a morbid poison, or indeed a poison of any kind, if present in the blood, should show its effects on a single tract of mucous membrane, without first producing any symptoms whatever of its presence.
The symptoms which follow the affection of the alimentary canal in cholera are exactly those which this affection is adequate, and, indeed, could not fail to produce. The analyses which have been made of the blood of cholera patients, show that the watery fluid effused into the stomach and bowels is not replaced by absorption, or is replaced only to a small extent. The experiments of Dr. O'Shaughnessy and others during the cholera of 1831-32, show that the amount of water in the blood was very much diminished in proportion to the solid constituents, and that the salts of the blood were also diminished. The experiments of Dr. Garrod and Dr. Parkes in the spring of 1849, were more numerous and exact.*
(* See London Journal of Medicine, May, 1849)
The amount of water in the blood of healthy persons is on the average 785 parts in 1000, whereas in the average of the analyses performed by Drs. Garrod and Parkes it was only 733 parts, while the amount of solid constituents of the blood relatively to the water was increased from 215--healthy standard--to 267. The globules, together with the albumen and other organic constituents of the serum, amount in the healthy state to 208 parts in 1000, while in the blood of cholera patients they amounted to 256 parts. The saline constituents in 1000 parts of blood are somewhat increased on account of the great diminution of water; but when estimated in relation to the other solid ingredients, or to the whole quantity existing in the healthy body, the amount is diminished. Dr. Garrod is of opinion that a chemical analysis will determine whether or not a specimen of blood has been derived from a cholera patient.
The stools and vomited matters in cholera consist of water containing a small quantity of the salts of the blood, and a very little albuminous substance. The change in the blood is precisely that which the loss by the alimentary canal ought to produce; and, indeed, it is physically impossible that the alteration in the blood can be caused in any other way. The sweating which takes place in an advanced stage of the disease may increase the density of the blood to a trifling extent; but it does not come on till the blood is already altered, and is only a consequence of the diminished force of the circulation, like the sweating met with in collapse from hæmorrhage or severe injuries, and in faintness from venesection.
The loss of water from the blood causes it to assume the thick tarry appearance so well known to all who have opened a vein in cholera. The diminished volume of the blood causes many of the symptoms of a true haemorrhage, as debility, faintness, and coldness; while these effects are much increased by its thick and tenacious condition, which impedes its passage through the pulmonary capillaries, thereby reducing the contents of the arteries throughout the system to the smallest possible amount, as indicated by the thready pulse. The interruption to the pulmonary circulation occasioned by the want of fluidity of the blood, is the cause of the distressing feeling of want of breath. Proofs of the obstructed circulation through the lungs generally remain after death, in the distended state of the pulmonary arteries and right cavities of the heart. The deficient supply of blood to the various organs, and its unfitness to pass through the capillaries, are the cause of the suppression of the renal, biliary, and other secretions. The cramps appear to consist chiefly of reflex action caused by the irritation and probably the distension of the bowels.
If any further proof were wanted than those above stated, that all the symptoms attending cholera, except those connected with the alimentary canal, depend simply on the physical alteration of the blood, and not on any cholera poison circulating in the system, it would only be necessary to allude to the effects of a weak saline solution injected into the veins in the stage of collapse. The shrunken skin becomes filled out, and loses its coldness and lividity; the countenance assumes a natural aspect; the patient is able to sit up, and for a time seems well. If the symptoms were caused by a poison circulating in the blood, and depressing the action of the heart, it is impossible that they should thus be suspended by an injection of warm water, holding a little carbonate of soda in solution.
It has often been contended that the collapse of cholera cannot be the mere result of the purging and vomiting, because, in some of the most rapid and malignant cases, the amount of the stools and vomited fluid is less than in milder and more protracted ones, or even in some cases in which the patient recovers. But in the most rapid and malignant cases there is sufficient loss of aqueous fluid by the alimentary canal to alter the blood into the thick tenacious state peculiar to this disease; and the fact of more purging occurring in other cases which are more protracted only proves that, in these latter, absorption from the stomach and intestines has not been altogether arrested, or that the stools have been diluted with fluids drunk by the patient. The loss of fluid in every case of fully developed cholera must be sufficient to cause the thickened state of the blood which is the cause of the algide symptoms, and the amount of malignancy of the case must depend chiefly on the extent to which the function of absorption is impaired. If absorption were altogether arrested in every case of cholera from the beginning, the amount of discharge from the alimentary canal would not equal that of a fatal hæmorrhage, for the thickened blood which remains behind is certainly not able to maintain life so well as the same quantity of healthy blood. Indeed, it is easy to calculate the amount of fluid separated from the blood, by means of the analyses previously quoted, and others which have been made of the cholera stools. In some analyses of these evacuations performed by Dr. Parkes* the average composition in 1000 parts was found to be 982.4 water and 17.6 solids; consequently, the problem merely is to find how much of such a fluid requires to be subtracted from blood consisting of water 785 and solids 215, in 1000 parts, in order to reduce it to blood, consisting of water 733 and solids 267.
(* London Journal of Medicine, Loc. Cit.)
The answer to this problem is, that 208.5 parts would require to be subtracted from 1000 parts of blood. M. Valentin has estimated the average amount of blood in the human adult at thirty pounds; and, therefore, the whole quantity of fluid that requires to be effused into the stomach and bowels, in order to reduce the blood of a healthy adult individual to the condition in which it is met with in the collapse of cholera is, on the average, 100 ounces, or five imperial pints. This calculation may be useful as indicating the amount of fluid, which ought not to be exceeded in the injection of the blood-vessels.
The evidence of the mode of propagation of cholera--which there is not time to discuss on the present occasion--confirms the above facts respecting the pathology of the disease, by showing that the cholera poison enters the alimentary canal by being accidentally swallowed, and there becomes multiplied. It is most probable that all morbid poisons having the property of propagating themselves are more or less organized; and if it be objected that the cholera poison cannot be recognized by the microscope in the feces or in the alimentary canal after death, it must be remembered, that the matter of small-pox cannot be distinguished from so much harmless pus; and it is only by their origin and effects that we can distinguish this and other morbid poisons.
It is pretty obvious, for the reasons stated above, that what we have to deal with in cholera is, a low form of organic action going on upon the interior surface of the stomach and intestines. The morbid poison so multiplying or reproducing itself probably acts as an irritant, and causes the great effusion of watery fluid and the arrest of absorption which produce all the mischief in this disease; or, what is still more probable, if the materies morbi have a cellular structure, is, that it withdraws the fluid from the blood circulating in the capillaries by a power analogous to that by which the epithelial cells of the various organs abstract the different secretions in the healthy body.
At all events, whatever be the intimate nature of the morbid action we have to combat in treating cholera, it is situated on the inner surface of the alimentary canal, and our remedies should be directed to act on that part rather than to be absorbed; and should be so contrived as to come in contact, if possible, with every part of the mucous membrane of the whole alimentary canal. The medicines should be such as have the property of destroying low forms of organised beings, and of arresting fermentation, putrefaction, and other kinds of molecular change in organic matter.
A line of practice which seems to fulfil the indications just mentioned is related to have been followed in Spain with great success in 1833. Don Pedro Vazquez--its originator--published a pamphlet on the subject at Seville, in 1833, and another in the following year. The treatment consisted in giving about a quarter of a pint of olive oil, and repeating the dose two or three times at short intervals, with the intention, as the author says, of varnishing the interior of the stomach and intestines, to defend them against the action of a bad bile, by which he supposed the disease to be occasioned. It is not surprising that, with such an erroneous pathology for its basis, this treatment made no progress in countries where medicine is better cultivated than in Spain; but I consider it well deserving of a further trial on different grounds from those on which it was introduced. Prepared animal charcoal is an agent which I think deserves a more extended trial than it has yet received. Its antiseptic properties, and its power of preventing the rusting of iron and other forms of oxidation render it probable that it might counteract the effects of the cholera poison.
Sulphur, which has been recommended as a remedy for cholera by Mr. Grove, is very likely to be of service, judging of it from the power it possesses of destroying the lower forms of organized beings belonging both to the vegetable and animal kingdoms. The three agents just mentioned have the advantages that they may be given in large doses without fear of injury to the patient; and, from their physical condition, would be likely to be diffused over every part of the alimentary canal. Sulphurous acid, and the hyposulphite of soda, which have been recommended in cholera, would be likely to be beneficial for the same reasons that sulphur is advisable; but they would be less likely to pass along the whole tract of the intestines, on account of their solubility, except in cases where the function of absorption is quite in abeyance.
Some of the essential oils, and more particularly oil of cajeput, have had a considerable reputation in the treatment of cholera, as also have camphor and creosote. Now, all these agents are highly antiseptic, and also possess the property of preventing mouldiness and other low forms of organisation; and it is, no doubt, by a similar power that they are useful in cholera. Creosote has the additional recommendation, that it acts as an astringent in ordinary diarrhæa. If the view I take of the pathology of cholera be correct, these remedies should be intimately diffused in an emulsion, to insure, if possible, their application to the whole surface of the stomach and bowels. Chloroform resembles creosote, camphor, and the essential oils, in its antiseptic and medicinal properties; and it has gained some reputation as a remedy for cholera, when introduced into the stomach. Administered in the way of inhalation, it is merely useful in relieving the cramps, and has no effect on the progress of the malady; while, if cholera were a blood disease, it would be by inhalation that this and every other volatile medicine ought to be exhibited.
The benefit which has been observed in many cases from calomel, no doubt, arises from its direct action on the cholera poison in the alimentary canal, and not from its being absorbed. It has often been matter of regret to Medical men, that calomel and other medicines are not absorbed in cholera; but this regret is needless, as they do not require to be absorbed. If calomel be given in cholera, it should obviously not be in pills, but as a powder, in order that it may be diffused as extensively as possible over the mucous membrane. There are two plans of treatment having a considerable number of advocates, although they appear of an opposite nature. I allude to the saline treatment, consisting chiefly of draughts containing carbonate of soda; and the treatment of sulphuric acid. It is quite possible, however, that either of those plans, when commenced in time, may have the effect of destroying the cholera poison, or neutralising its action. There are many kinds of molecular changes in organic matter--low organic processes, as they may be called, which can be checked either by an alkali or a mineral acid. I feel great pleasure in being able to explain how cholera may probably be treated beneficially on very different plans; for, if this were not the case, the character of the Medical Profession for correct and trustworthy observation would be very much in danger. Making every allowance for the difficulty of the subject, unless cholera patients can be benefited by medicines which hold very different places in the classification of materia medica, it must be admitted that the literature on the treatment of this disease would be little creditable to us as scientific observers.
When we consider that the materies morbi [an outdated medical term referring to the substances or factors that cause disease] of cholera finds its proper seat and sustenance only in the alimentary canal of the human being, and produces no effect apparently on the domestic animals, by which it must often be accidentally swallowed, it is probable that very slight causes often prevent its action in the first instance; and there is very good evidence that medicines of no great power will generally arrest its effects if given early, in such cases as commence gradually. Without assuming either that all the cases of diarrhæa which accompany an epidemic of cholera would pass into the developed malady if unchecked, or that every case of cholera commences with what seems an ordinary diarrhæa, when we reflect how generally the history of cholera cases begins with an ordinary an ordinary looseness, and how seldom the cases of simple diarrhæa which come under treatment during an epidemic pass into cholera, it is pretty evident that the ordinary remedies for diarrhæa have the effect of curing many cases of cholera in the early stage. As it cannot for a moment be supposed that such medicines as the pulvis cretæ compositus cum opio can have the effect of arresting a disease caused by a morbid poison circulating in the blood, all the evidence of the benefits of house-to-house visitation among the poor during an epidemic confirms the view of the pathology of cholera with which I commenced this paper, viz., that the disease consists primarily and essentially of a morbid action in the alimentary canal. The great difficulty in ascertaining the effect of treatment in cholera consists in the circumstance, that the disease cannot be distinguished with certainty, except in a very advanced stage. If we could not recognise typhus fever till the patient had lapsed into the state of stupor from which the disease is named, we should be able to show fewer recoveries from that complaint than from cholera. One effect of not perceiving that the real seat of cholera is the alimentary canal, is to cause the treatment directed to the bowels to be left off too soon, and the attention of the practitioner to be engrossed by what are only the secondary effects of the disease. When called to a patient in a state of collapse from hæmorrhage, the first consideration of the Medical man is to prevent any further loss of blood; and, in the collapse of cholera, the chief effort should still be, to prevent any more of that effusion which has brought the patient to the condition in which we find him. It has appeared to me, that the cases which prove fatal in the stage of collapse are generally lost through the continuance of the purging; and I have seen several patients, who appeared about to recover, suffer a relapse, and sink from a return of this symptom.
Unless it is determined to inject the veins, or, as Mr. Henry Lee has suggested, the arteries, with a very weak saline solution, it is clear that the patient cannot recover from the state of collapse, except by the absorption of watery fluids from the alimentary canal. To allow the drinking of cold water, for which there is a great desire, is in accordance both with reason and experience. The greater part of it is generally vomited, but that is of no consequence. On the other hand, reason and experience are just as much opposed to hot air-baths and other attempts to raise the heat of the surface, which can only have the effect of increasing the symptoms of asphyxia, so long as the blood remains so thick and tenacious, that it can hardly circulate either through the pulmonary or systemic capillaries. The results obtained, by injecting the blood-vessels in 1832, were so far encouraging, that it is somewhat surprising that this practice was hardly resorted to in 1849. The cause of its failing in most cases was, that the liquid injected flowed away almost immediately by the alimentary canal; in future, it would therefore be desirable to continue the treatment directed against the affection of the stomach and bowels, at the same time that the blood-vessels are injected. As regards the nature of the injected fluid, Dr. Garrod has very properly suggested, that a solution should be employed which resembles as much as possible the portion of the blood which has been lost; and he recommends that the phosphate of soda should be used, rather than the carbonate, which has generally been employed.
The so-called consecutive fever, which comes on after certain cases of cholera, is caused by the retention of excrementitious matters in the blood, owing to the kidneys not resuming their functions. It must be looked on rather as a sequela than an essential part of the disease, and I have nothing to offer to the Society respecting its treatment.
In bringing this short paper to a conclusion, it will be perceived that I have no plan of treatment to offer which promises any great results in the more severe and fully-developed cases of cholera, and, indeed, that I have suggested nothing in the way of treatment that is new. The view of the pathology, however, which I have endeavoured to establish, has a tendency to circumscribe and define the objects of treatment. I have endeavoured to prove that the seat and action of the materies morbi of cholera is the interior of the alimentary canal, and the principles of treatment resulting from this view of the disease may be briefly recapitulated as follows:--
1st. Medicines should be chosen which have the effect of preventing the various kinds of molecular change in organic matter.
2nd. They should be administered with a view to their action in the stomach and bowels, and not to their being absorbed.
3rd. The medicines should be given in such quantities and in such form as to insure as much as possible their application to the whole surface of the alimentary tube.
4th. These remedies should be continued until there is no danger of a relapse.
5th. It is useless and injurious to attempt to bring the patient out of the state of collapse by stimulants and the application of heat, and we should give watery drinks, and be content to wait till they are absorbed, unless in desperate cases, when it might be desirable to inject into the blood-vessels a weak saline solution resembling "the portion of the blood which has been lost."
18, Sackville-street.
Return to John Snow Publications
Source: Snow, John. Medical Times and
Gazette 8, 10 June 1854, p. 606, [Letter to Ed.].
81. "On the recent death at St. George's Hospital, while the patient was beginning to inhale chloroform."
To the Editor of the Medical Times and Gazette
Sir,--I shall be obliged if you will allow me to make a few remarks respecting the recent death at St. George's Hospital, while chloroform was being inhaled. Mr. Cæsar Hawkins was kind enough to inform me of the circumstance, and I was present at the autopsy on the following day, when I obtained about six ounces of blood and a portion of lungs and liver for chemical examination. The blood was put into a flask, to which a hard glass tube calculated to bear a red heat was attached, and beyond this a tube moistened inside with solution of nitrate of silver. The flask was heated in the water-bath, a portion of the tube through which the air and vapour had to pass being kept red-hot. No precipitate of chloride of silver was formed, although the process was continued some hours. It was interrupted once, in order to break up the coagulum. The portion of lung, and subsequently the portion of liver, were cut in pieces, and treated in the same manner, with a similar negative result.
When an animal has been killed with chloroform, that compound can be very easily detected by the above process in all parts of the body, even for seven or eight days after death.*
(*See Medical Gazette, Vol. XLVI., p.324.)
I have also detected it readily in a portion of the muscles of a leg removed under the influence of chloroform to the usual extent; in fact, I have obtained a distinct precipitate of chloride of silver from the hundredth part of a grain of chloroform when mixed with six ounces of blood. It is evident, therefore, that the patient at St. George's Hospital must have inhaled only an extremely small quantity of chloroform; indeed, this is the opinion of the Medical men who were present at the time of her death. The inhaler was only applied for a minute and a half, and the valve which admits the air unmixed with vapour was only one-third closed; moreover, Mr. Potter informs me that the patient, who was much agitated, seemed to breathe very little, and he was talking to her, with a view to calm her apprehension, the moment before she died. I have never met with a patient who became insensible until the valve in question was much more than one-third closed, however free the breathing might be. A few days ago, I inhaled chloroform from a similar instrument with the valve one-third closed, and although there were two drachms and a-half of chloroform in the inhaler, and I breathed in the ordinary manner, I was able to observe the time by a watch for eight or nine minutes, and then merely fell asleep.
The case in question appears to have been one of sudden death; the immediate cause of its occurring at the moment when it did occur being probably mental emotion. In this respect it resembles the case of Mr. Badger, which occurred at Mr. Robinson's in 1848. The average number of sudden deaths in England and Wales from 1838 to 1842 was 3600 per annum, or one in 138 of the total deaths. In a certain number of such cases there is rupture of an aneurism or some other evident cause of death; but, in the majority of instances, there is nothing to indicate the immediate cause of dissolution. Mental emotion of some kind is frequently the immediate cause of sudden death. Several cases of this kind have come within my own knowledge, and within the last few days it is related in the newspapers, that "upon the occasion of the recent announcement of a free discharge to the convicts of the Newgate Prison, Dublin, under sentence of penal servitude, so overjoyed were four of them at the sudden intelligence that they dropped dead."
It is not surprising, therefore, that among the great numbers of patients to whom chloroform has been administered during the last six or seven years, two of them should have died suddenly while just beginning to inhale. Patients are known to have died just after being placed on the operating-table, before chloroform was introduced; and it appears that the same accident is still liable to occur, for it unfortunately happens, in many cases, that the intended inhalation of chloroform does not prevent fear. It cannot be supposed, however, that the inhalation of this agent increases the patient's fear, for should he not be more afraid of the pain than of the chloroform, he of course would decline to inhale it; nor can it be supposed that the chloroform increases the effects of fear, for it is matter of daily observation that, as soon as the patient gets so far under its influence as to be unconscious, the pulse, which had been very rapid from apprehension, greatly subsides to nearly its natural frequency.
As regards the post-mortem inspection in the case under consideration, there is nothing which throws any particular light on the cause of death. There was some amount of fatty degeneration of the heart, but not sufficient to account for death. The right cavities of the heart were not empty, as in the kind of syncope produced by loss of blood or anæmia; and it is impossible to ascertain whether or not they were greatly distended at the time of death, for the artificial respiration, and carrying the body down a number of stairs, while the blood was in a liquid state, might displace part of it. It is sufficiently probable that these cavities became over-distended while the patient was in fear and scarcely breathing, and that the action of the heart was thus arrested. The lungs contained a moderate quantity of blood, and neither indicated death by pure syncope nor by pure asphyxia. The brain was somewhat congested, which is quite consistent with death from mental emotion, though no great indication of it. The fluid state of the blood does not indicate anything, for in the human subject the blood generally remains fluid in cases of sudden death from whatever cause. In small animals, such as dogs, cats, and guinea-pigs, the blood generally coagulates, though loosely, in the heart and blood-vessels, after they have been killed by chloroform; and, if the vessels are opened immediately after death, the blood that escapes coagulates firmly. The truth is, that narcotics do not cause death by producing any physical or chemical change in the blood.
The only circumstances to guide us to the cause of death in the above case, are the symptoms just before dissolution, and the fact that the patient did not inhale enough chloroform to produce any effect whatever. In commenting on a case of death not caused by chloroform, it would be somewhat out of place to enter on the consideration of the cause of accidents by this agent, and the way in which they may be avoided; indeed, I have already treated of these subjects in former communications.
I am, etc.
John Snow, M.D.
18, Sackville-street, May 29.
Return to John Snow Publications
Source: Snow, John. Medical Times and
Gazette 9, 12 August 1854, p. 170. [Letter to Ed.].
82. "Cholera in the Baltic Fleet."
To the Editor of the Medical Times and Gazette.
Sir,--I have for some time been halting between two opinions respecting the manner in which the cholera had been introduced into the Baltic fleet,--whether by the capture of prizes which might have had cholera on board, or by drinking the water of the Baltic containing the evacuations of the cholera patients at St. Petersburg and Cronstadt.
A paragraph in your Journal of today [5 August 1854], page 152, inclines me, however, to adopt the latter opinion. The paragraph is as follows:--"The only ships which suffered from cholera are those which proceeded up to Cronstadt. The smaller vessels, especially the paddle squadron, have enjoyed a high standard of health," etc. They were the smaller steamers, I believe, that have been engaged in the capture of prizes, and not the large ships that proceeded up to Cronstadt, where the cholera was prevailing. These ships, we know, had no communication with the shore at Cronstadt, or with the enemy's shipping; and as experience is, in my opinion, entirely opposed to the view that the morbid matter of cholera passes through the atmosphere, except for a very limited distance, and that very rarely, the method I have pointed out is probably that by which the cholera was introduced. I am not able to say positively that the water of the Baltic was used on board the ships, and this is one reason of my writing, as I think it desirable that the point should be clearly ascertained. It has been publicly stated that the water in the upper part of the Baltic is quite fresh in the early part of summer, and that it was unnecessary to spend time in obtaining water from the shore. I have also been privately told that the sailors prefer the Baltic water to that which has been stored, and which tastes of the cask.
If the fleet in the Baltic had succeeded in avoiding the cholera, it is probable that London would have escaped the present epidemic of the disease, for the trade with the Baltic is suspended, and the communication between the Thames and that sea is almost confined to the fleet. Although we cannot trace the commencement of the present epidemic in London to an individual case, as the epidemic of 1848-1849 can be traced to John Harnold, of the steam-ship Elba, we know that the first cases occurred in persons residing, or being employed on board the shipping in the river, and among others near the river side. The cholera also appeared about the same time in an emigrant-ship and a troop-ship, soon after leaving the Thames. The following occurs in the last return of the Registrar-General:--
"In the same sub-district (St. James, Bermondsey,) at 10, Marine-street, on 24th July, a mate-mariner, aged 34 years, 'Asiatic cholera (101 hours,) after premonitory diarrhœa (16½ hours.)' The medical attendant states:--'This patient was chief-mate to a steam-vessel taking stores to and bringing home invalids from the Baltic fleet. Three weeks ago he brought home in his cabin the soiled linen of an officer who had been ill. The linen was washed at his house and returned.'"
This was not one of the first cases, and therefore I do not quote it as actually introducing the cholera into London, but only to show the kind of intercourse that has been going on between the Baltic and the Thames. It is probable that a few simple regulations respecting this intercourse might have kept London free from the cholera, and inflicted no hardship on anybody; but, unfortunately, the chief advisers of Government in sanitary matters have had their minds occupied about drain-pipes and bad smells, and have neglected the specialities connected with the propagation of individual diseases.
As regards the evidence which I conclude that the materies morbi of cholera is contained in the evacuations of the patients, and that it may retain its power of communicating the disease after being diluted with large quantities of water, I beg to refer the reader to former papers in the Medical Times and Gazette.*
(*Med. Gaz., 1849, Vol XLIV, p. 730, etc.: Med. Times, Dec. 1851; Med. Times and Gaz., 1853, Vol. VII., p. 367.)
I will, at present, only notice an objection which has been made to the latter part of my view,--that relating to the water. It has been said, that the cholera poison would be rendered inert by the large dilution, or, if not, that every one drinking the contaminated water should have the disease. One answer meets both parts of the objection. A substance cannot be diluted beyond the ultimate particles of which it consists. The morbid matter of cholera, like the pus of small-pox and other morbid poisons, owes its properties, no doubt, to cells; and there is no more reason why diluting with water should necessarily destroy their activity, than that it should destroy the ova of fishes; and there is also no reason why every one who dips a pail into the water should draw a prize.
--I am, etc.
John Snow, M.D.
Sackville-street, Aug. 5
[The full paragraph on p. 152 of the 5 August number reads as follows:
"Health of the Baltic Fleet.--The only ships which suferred from cholera are those which proceeded up to Cronstadt. The smaller vessels, especially the paddle squadron, have enjoyed a high standard of health, the percentage of sick not averaging more than 2½. Sulphuric acid has been extensively tried. It was much liked by the patients, and taken, freely diluted, greedily. We are promised full accounts of its effects in future letters."]
Return to John Snow Publications
Source: Snow, John. Med. Times and Gazette 9, 2 September 1854, pp. 247-248.
83. "Communication of cholera by Thames water."
To the Editor of the Medical Times and Gazette.
Sir,--I have been engaged, during the last ten days, in an inquiry which promises to yield very conclusive evidence respecting the mode of propagation of cholera. You are, no doubt, aware, that there is an Act of Parliament requiring those Water Companies of the Metropolis which obtain their supply from the River Thames, to procure it at some point above the reach of the tide, and, consequently, free from the sewage of London. A certain time, which is not yet expired, was, however, allowed for the completion of the necessary works. The Lambeth Water Company, which formerly obtained their supply from a point near Hungerford Suspension-bridge, completed their works at Thames Ditton [near Hampton Court Palace] upwards of a year ago, and have ever since distributed water perfectly free from the sewage of London. The Southwark and Vauxhall Water Company, which, along with that just named, supplies the greater number of houses on the south side of the Thames, still obtain their supply from Battersea-fields, near Vauxhall. The mortality from cholera was much less during the epidemic of last autumn, in the districts to which the new supply of water extended, than in those districts which are exclusively supplied by the Southwark and Vauxhall Company. This will be seen on referring to a table in the return of deaths in London, for the week ending the 26th of November, 1853. Soon after the commencement of the present epidemic, the difference in the mortality of the respective sets of districts was equally apparent,--a difference which did not exist in 1849.
In order to ascertain clearly on what this difference in mortality depended, it was necessary to make an inquiry in detail. The only districts which are supplied exclusively with the water from Thames Ditton, are such distant places as Balham, Streatham, Dulwich, and Sydenham, whose freedom from the epidemic might be attributed to other causes than the mere absence of the polluted water. In the districts of Lambeth, Newington, and St. George, Southwark, the customers of the two Companies are so intimately mixed with each other, that two adjoining houses have very often a different supply of water; and it was, therefore, impossible to determine what kind of water was used in the houses in which the deaths from cholera occurred, except by an inquiry on the spot. I consequently resolved to call at each house where there had been a death from cholera; and Mr. Farr has been kind enough to allow me to take a copy of the addresses of those cases which have not been published in the weekly returns. I have gone over the sub-districts of Lambeth, called Kennington, first part, and Kennington, second part, as regards the deaths from cholera which occurred down to August 12; and the sub-districts, Waterloo, first part, and Waterloo, second part, to August 19th. The following are the results I have obtained:--
Kennington, First Part
Kennington, Second Part
Waterloo, First Part
In Waterloo, second part, 27 deaths have occurred in 24 houses, which are supplied as follow:--
If the cases are enumerated instead of the houses in this last sub-district, the return is as follows:--
According to the returns made by the water companies to Parliament and to the Board of Health, there are quite as many houses supplied by the Lambeth as by the Southwark and Vauxhall Company, in the above districts; and both Companies supply alike all kinds of houses,--those of the rich and the poor indiscriminately. It is evident, therefore, that, in the sub-districts to which the inquiry has extended, the people having the improved water supply enjoy as much immunity from cholera as if they were living at a higher level, on the north side of the Thames; and I ascertained that in two of the instances where the water supply afterwards turned out to be of the improved kind, the cases could be traced to personal communication with previous ones.
I intend to continue the inquiry, extending it to the other sub-districts in which the two water companies are intermixed, and to bring it down to the 26th inst. After this date, I am informed by Mr. Farr that the supply of water at the house in which every fatal attack of cholera may occur, will be returned by the Registrars in all the Districts on the South of the Thames. An amount of information will thus be obtained that will be very conclusive. In the mean time, I have considered that the inquiry, even in its present stage, is too important to be withheld from the Profession, at a season when every week is adding so much to the mortality from cholera.
I must say a word on the nature of the water supplied by the Southwark and Vauxhall Company. It is not worse, either physically or chemically, than the water that has generally been supplied to town populations. It undergoes a coarse kind of filtration before it is distributed, and it passes with careless observers for being quite clear, though it is not so in reality. It contains organic matter, both in solution and suspension, and deposits a small quantity of whitish flocculent matter on standing. It also contains a much larger quantity of chlorides than Thames water obtained above the reach of the London sewage. As the Chelsea Water Company obtain their supply from almost the same part of the Thames, and have in every epidemic very much less cholera in their district, I may as well explain, that they filter their water much better than the Southwark and Vauxhall Company, and no doubt rid it to a much greater extent of the cholera evacuations which pass down the sewers into the Thames. I am, etc.
18, Sackville-street, Aug., 1854.
John Snow.
Return to John Snow Publications
Source: Snow, John. Med. Times and
Gazette 9, 23 September 1854, pp. 321-322, [Letter to Ed.].
84. "The cholera near Golden Square and at Deptford"
To the Editor of the Medical Times and Gazette.
Sir,--As soon as I became acquainted with the situation and extent of the late outbreak of cholera in Broad-street, Golden Square, and the adjoining street[s], I suspected some contamination of the water of the much frequented street-pump in Broad-street, near the end of Cambridge-street: but on examining the water, on the evening of the 3rd inst., I found so little impurity in it of an organic nature, that I hesitated to come to a conclusion. Further inquiry, however, showed me that there was no other circumstance or thing common to the circumscribed locality in which this sudden increase of cholera occurred, and not extending beyond this locality, except the water of the above pump. I found, moreover, that the water varied, during the next two days, in the amount of organic impurity it contained; and I concluded that, at the commencement of the outbreak, it might have been still more impure. I requested permission, therefore, to take a list at the General Register Office of the deaths from cholera registered during the week ending September 2, in the sub-districts of Golden-square, Berwick-street, and St. Ann's, Soho. Eighty-nine deaths from cholera were registered during the week, in the three sub-districts. Of these, only six occurred in the four first days of the week, four occurred on Thursday, the 31st ult., and the remaining seventy-nine on Friday and Saturday. I considered, therefore, that the outbreak commenced on the Thursday; and I made an inquiry, in detail, respecting the eighty-three deaths registered as having taken place during the last three days of the week. On proceeding to the spot, I found that nearly all the deaths had taken place within a short distance of the pump. There were only ten deaths in houses situated decidedly nearer to another street pump. In five of these cases the families of the deceased persons informed me that they always sent to the pump in Broad-street, as they preferred the water to that of the pumps which were nearer. In three other cases the deceased were children who went to school near the pump in Broad-street. Two of them were known to drink the water, and the parents of the third think it probable that it did so. The other two deaths, beyond the district which this pump supplies, represent only the amount of mortality from cholera that was occurring before the eruption took place. With regard to the deaths occurring in the locality belonging to the pump, there were 61 instances in which I was informed that the deceased persons used to drink the pump water from Broad-street, either constantly or occasionally. In 6 instances I could get no information, owing to the death or departure of every one connected with the deceased individuals; and in 6 cases I was informed that the deceased persons did not drink the pump water before their illness.
The result of this inquiry, then, is, that there has been no particular outbreak or prevalence of cholera in this part of London except among the persons who were in the habit of drinking the water of the above-mentioned pump-well.
I had an interview with the Board of Guardians of St. James's parish, on the evening of the 7th inst., and represented the above circumstances to them. In consequence of what I said, the handle of the pump was removed on the following day. The number of attacks of cholera had been diminished before this measure was adopted, but whether they had diminished in a greater proportion than might be accounted for by the flight of the great bulk of the population I am unable to say. In two or three days after the use of the water was discontinued the number of fresh attacks became very few.
I have not thought it necessary to inquire into the very large number of deaths that occurred in the week ending Sept. 9, as I deem the above inquiry sufficient to establish the cause of the outbreak. I have, however, inquired respecting a few deaths in that week, which took place a little further from the pump than the others; and I found that, in all the cases but one, the persons had been drinking water from that pump. A great number of work-people who were employed in and near Broad-street died of cholera at their own homes in other parts of London. Mr. Marshall, surgeon, of Greek-street, was kind enough to inquire respecting seven workmen, who had been employed in the manufacture of dentists' materials at Nos. 8 and 9, Broad-street, and who died at their own homes. He learned that they were all in the habit of drinking water from the pump, generally drinking about half a pint once or twice a-day, while two persons who reside constantly on the premises, but do not drink the pump water, have only had diarrhœa.
The pump-well in Broad Street is from 28 to 30 feet in depth, and the sewer, which passes a few yards from it, is 22 feet below the surface. This sewer proceeds from Marshall-street, where some cases of cholera had occurred before the great outbreak.
I am of opinion that the contamination of the water of the pump-wells of large towns is a matter of vital importance. Most of the pumps in this neighbourhood yield water that is very impure and I believe that it is merely to the accident of the cholera evacuations not having passed along the sewers nearest to the wells that many localities in London near a favourite pump have escaped a catastrophe similar to that which has just occurred in this parish.
In the autumn of 1848, when cholera had just commenced in London, a number of cases occurred about Bridge Street, Blackfriars; and it was found by Mr. Hutchinson, Surgeon, of Farringdon Street, that the well of St. Bride's pump had a communication with the Fleet ditch, up which the tide flows. I have a strong impression that many a case of typhoid fever occurring in a respectable neighbourhood has its origin in the water of the neighbouring pump.
On the 12th instant, I went to Deptford, to make inquiries respecting a most fatal outbreak of cholera which had taken place there, being confined to two streets, called New Street and French's Fields. I found that this outbreak of cholera was caused by an accidental contamination of the drinking water, occurring in an unusual manner. The people in these two streets, in which about ninety deaths from cholera occurred in a few days, have the water of the Kent Water-works; but for three or four weeks before my inquiry, they told me that the water, when it first came in, had generally smelt highly offensive, and frothed like soap-suds. They had been in the habit of throwing away a few pailsful of what first came in, and retaining that which came afterwards, and was pretty clear. On inquiring in all the surrounding streets, viz., Wellington Street, Old King Street, and Hughes' Fields, I found that there had been no alteration in the water. I conclude, therefore, that some leakage had taken place into the pipes supplying these two streets, during the intervals when the water was not turned on. There are no sewers in these streets, and the refuse of all kinds, consequently, saturates the ground in which the pipes are laid. There were a few cases of cholera in and near New Street just before the great outbreak.
I have very nearly concluded the inquiry respecting the comparative influence of the water of the Lambeth Water Company and that of the Southwark and Vauxhall Company, of which I gave some account in the Number of the Medical Times and Gazette of the 2nd inst. The result, which I shall communicate when completed, will show that among the population having the impure water of the Thames, from Battersea Fields, the mortality from cholera has been ten times as great as among the population having the improved water from Thames Ditton.
I am, Sir, etc.
John Snow, M.D.
18, Sackville Street, September, 1854.
Return to John Snow Publications
Source: Snow, John. Med. Times and
Gazette 9, 7 October 1854, pp. 365-366.
85. "On the communication of cholera by impure Thames water."
By John Snow, M.D.
I have now completed the inquiry of which I gave some account in a letter published in the Medical Times and Gazette of Sept. 2. I have called at every house in which a death from cholera had occurred and been registered during the first seven weeks of the present epidemic, in all the sub-districts to which the supply of the Lambeth Water Company extends. In the cases of persons removed to a workhouse or any other place after the attack, I have extended the inquiry to the house in which the attack commenced. In a few cases the address of persons removed to a workhouse was not known; in a few other instances the individuals were of such an itinerant character that it was impossible to ascertain where the illness might have been contracted. These cases are placed, with a few others which could not be found, in the column of the accompanying table for deaths where the water supply was not ascertained.
There were very few instances in which I could at once get the information I required. Even when the water rates are paid by the residents, they can seldom remember the name of the Water Company till they have looked for the receipt. In the case of working people who pay weekly rents, the rates are invariably paid by the landlord or his agent, who often lives at a distance, and the residents know nothing about the matter. It would, therefore, have been impossible for me to complete the inquiry if I had not found that I could distinguish the water of the two Companies with perfect certainty by a chemical test. The test I used is founded on the great difference in the quantity of chloride of sodium contained in the two kinds of water. On adding solution of nitrate of silver to a gallon of the water of the Lambeth Company, obtained at Thames Ditton, beyond the reach of the sewage of London, only 2.28 grains of chloride of silver are obtained, indicating the presence of .95 grains of chloride of sodium in the water. On treating the water of the Southwark and Vauxhall Company in the same manner, 91 grains of chloride of silver are obtained, showing the presence of 37.9 grains of common salt per gallon. Indeed, the difference in appearance on adding nitrate of silver to the two kinds of water is so great, that they can be at once distinguished without any further trouble. This test is not liable to any fallacy. The Lambeth water may become impure by remaining in a butt without cover, but the quantity of chlorides is not increased; and, on the other hand, the water of the Southwark Company may become perfectly free from organic impurity by spontaneous putrefaction, but the quantity of chloride of sodium remains unaltered. The common salt is, I believe, part of that which has passed through the kidneys and bowels of the two millions and a-quarter of inhabitants of London. I do not, of course, attribute any ill effects to this common salt, and I found it of great use in conducting the inquiry. When the resident could not give clear and conclusive evidence about the Water Company, I obtained some of the water in a small phial, and wrote the address on the cover, when I could examine it after coming home.
The number of deaths from cholera down to August 26, in the sub-districts which are partly supplied by the Lambeth Water Company, was 642. Of these I found that the water supplied to the house in which the attack took place was, in 509 instances, that of the Southwark and Vauxhall Water Company; in 93 cases it was that of the Lambeth Company; and in the remaining 40 instances it was from other sources, or the supply was not ascertained.
I hope shortly to learn the number of houses in each sub-district supplied by each of the Water Companies respectively, when the effect of the impure water in propagating cholera will be shown in a very striking manner, and with great detail. In the mean time, in order to be able to compare the mortality from cholera among the customers of each Company, with the entire number of houses supplied by each of them respectively, I thought it desirable to extend the inquiry to Rotherhithe, Bermondsey, Camberwell, and certain parts of Southwark, which are supplied by the Southwark and Vauxhall Company alone. I was unable by myself to execute this part of the inquiry before the commencement of the winter session, but I was fortunate enough to obtain the assistance of a medical man, Mr. John Joseph Whiting, L. A. C., who took great pains with this part of the inquiry. The inquiry thus extended reached over the whole of the districts on the south side of the Thames, except those of Greenwich and Lewisham. As regards most of the sub-districts, to which the water of the Lambeth Company does not extend, the personal inquiry reached only to the first four weeks of the epidemic, viz., to August 5, and the remaining cases are calculated to have been supplied by the Company, or to have obtained water from ditches, etc., in the same proportions as those occurring previously. The sub-districts in which the numbers are partly made up by calculation, are marked with an asterisk in the accompanying table.
In the instances placed in the column for pump-wells and springs the houses were not supplied by either Water Company. There are a few houses in the suburbs which have a pump-well in addition to the Water Company's supply, but I have not indicated this in the table. I shall, however, state the circumstance in the list of deaths from cholera, which I intend to have reprinted from the Weekly Returns of the Registrar-General. The cases in which water was obtained direct from the Thames by pailsful or from the river Wandle, the Surrey Canal, or ditches, are included in a separate column.
The accompanying table shows that, during the first seven weeks of the present epidemic, 1224 fatal attacks of cholera occurred in houses supplied with the impure water of the Southwark and Vauxhall Water Company, obtained at Battersea Fields, and that only 93 fatal attacks occurred in houses having the improved water supply from Thames Ditton. The entire number of houses supplied by the Southwark and Vauxhall Company, according to a return made to the General Board of Health in 1850, was 34,217, and the number supplied by the Lambeth Company, according to the same return, was 23,396. The number of houses supplied by both Companies has increased with the extension of the Metropolis, but it is pretty certain that the proportion continues nearly the same, and for the sake of comparison, the number of houses may be supposed to remain the same also. Now, 34,217 ÷ 1224 = 28, and 23,396 ÷ 93 = 251. So that while a death from cholera had occurred in 1 house in every 28 supplied by the Southwark and Vauxhall Company, a fatal attack of cholera had occurred in only 1 out of 251 of the houses supplied by the Lambeth Company. The mortality, in short, to August 26, was just nine times as great in the houses supplied by the former Company as in those supplied by the latter.
There is another way in which the beneficial influence of the improved water on the progress of cholera may be shown. On referring to the Population Table of the late Census [as of March 30, 1851], it will be found that the districts and sub-districts which are partly supplied with water by the Lambeth Company contained 41,984 houses, inhabited and uninhabited; and that the population amounted to 271,987. At the end of last year the Lambeth Company supplied 25,583 houses, the population of which must have been about 165,000. But 93 deaths from cholera, the number which occurred in the population so supplied in these districts, is a proportion very little exceeding the mortality which had occurred at that time in the most elevated and favoured districts of the Metropolis, and much less than had happened in the West districts of London. It should be recollected, also, that a great portion of the population in the South districts are very poor, and are surrounded by all the conditions which have been generally supposed to favour cholera.
During the first four weeks of the present epidemic, 563 persons died of cholera in London. Of these it has been ascertained, by a personal inquiry at every one of the houses in which the attack took place, that no less than 268 of the fatal attacks took place in houses supplied with water by the Southwark and Vauxhall Company. A great part of the remaining deaths occurred in persons living or working among the shipping of the Thames, and who almost invariably draw their water direct from the river. During these four weeks there were but ten deaths from cholera in houses supplied with water by the Lambeth Water Company; although it has been shown above that they supply fully two-thirds as many houses as the other Company. The cholera was consequently eighteen times as fatal among the population supplied with the water from Battersea Fields as among that with the purer water from Thames Ditton, during these four weeks, although this latter population is intimately mixed with the former.
It may, indeed, be confidently asserted, that if the Southwark and Vauxhall Water Company had been able to use the same expedition as the Lambeth Company in completing their new works, and obtaining water free from sewage, the present epidemic of cholera would have been confined in a great measure to persons employed among the shipping, and to poor people, who get water by pailsful direct from the Thames or tidal ditches. It is quite obvious, that the mischief caused by the water of the Southwark Company is not confined to the cases occurring in the houses so supplied; for there are few people who take no food or drink except in their own houses; and persons, in all parts of London, have been attacked with cholera, after visiting the south districts of the town. The disease of course does not always stop with the cases produced directly by the water, but among poor people of not very cleanly habits; and where a whole family is confined to one or two small rooms, other cases follow the first in rapid succession. In many instances two or three deaths have occurred within a few days; and even where but a single death has occurred among poor people, I have seldom inquired without hearing of other cases more or less severe in the same house, and about the same time.
The cholera of 1849 was much more fatal in London than that of 1832; the present epidemic has been more fatal in the districts supplied exclusively by the Southwark and Vauxhall Company than that of 1849; and if the Lambeth Company had not changed their source of supply the mortality in London would have much exceeded that of 1849. There is one circumstance, however, that ought to prevent any expression of blame or recrimination for the propagation of cholera in this way; it is this,--that the persons who have been most instrumental in causing the increase of cholera, are precisely those who have made the greatest efforts to check it, and who have been loudest in blaming what they considered the supineness of others. In 1832, there were few water-closets in London. The privies were chiefly emptied by nightmen, a race who have almost ceased to exist; or a portion of the contents of the cesspool flowed slowly, and after a time, into the sewers. By continued efforts to get rid of what were called the removable causes of disease, the excrement of the community has been washed every year more rapidly into the river from which two-thirds of the inhabitants, till lately, obtained their supply of water. While the fæces lay in the cesspools or sewers, giving off a small quantity of unpleasant gas having no power to propagate specific diseases, they were spoken of as dangerous and pestilential nuisances; but, when washed into the drinking-water of the community, they figured only in Sanitary Reports as so many grains of organic matter per gallon.
In 1832, the Borough of Southwark was supplied with water taken from the Thames near London-bridge, and sent direct to the houses, without any intervening reservoir; and this was the part of London which suffered most from cholera at that time. The Water Company, some time afterwards, discontinued this source of supply, to join with a Company obtaining water at Battersea-fields; but the increasing pollution of the Thames surpassed the efforts to get cleaner water, and the water at Battersea was soon worse than it had been at London-bridge. It is somewhat remarkable, that almost everything that has been done with a view to check the progress of cholera has had the effect of increasing it. Flushing the sewers, which was carried on in 1849, has certainly not been repeated during the present season; but increased quantities of water have been supplied at more frequent intervals, causing the water-butts to overflow for hours together, and having the effect of washing the evacuations of the cholera patients more quickly into the river, from whence they were distributed again to the community sooner than usual; as the increased quantity of water sent out did not permit it to remain the usual time in the settling reservoirs. Owing to this increase of the supply, the water of the Southwark and Vauxhall Company has been more than usually dirty, and full of living things, during the last few weeks.
These circumstances prove very clearly, that a disease is not to be prevented except by a correct knowledge of its real cause; and that it is to the improvement of the science of Medicine, by the study and observation of Medical men, that society must look for the diminution of mortality; and not to the ill-directed efforts of benevolent individuals among the non-medical part of the community.
18, Sackville-street, Oct. 2, 1854.
Return to John Snow Publications
Source: Snow, John. Transactions of the Epidemiological Society. Journal of Public Health and Sanitary Review 1, 1855, pp. 16-24. [Paper delivered 2 May 1853].
86. "On the comparative mortality of large towns and rural districts, and the causes by which it is influenced."
Paper read before the Epidemiological Society of London, on May 2, 1853. Published as part of the Transactions of the Epidemiological Society.
By John Snow, M.D.
It is well known that the average duration of life in the large towns of this country is much less than amongst the rural population. This depends, as most persons are aware, partly on the smaller number of persons who attain to old age in large towns, and partly on the greater mortality in infancy and early childhood. For instance, rather more than forty per cent of the deaths which take place in London occur under five years of age; nearly forty-eight per cent of the deaths in Birmingham, fifty-one per cent in Manchester, and fifty-two per cent in Liverpool, occur before the same age; consequently more than half the children that are born in the last two towns die before they are five years old. In Wiltshire, on the other hand, the deaths under five years comprise but thirty-one and a-half per cent of the deaths at all ages; in Surrey, not including the metropolitan part of it, the deaths under five are not quite thirty-one per cent of the whole; and in the united district of Guildford, Farnham, and Hambledon, in the more distant and rural part of Surrey, the deaths under five years do not quite reach twenty-nine per cent of the whole number of deaths. When the deaths under five years of age are considered, in relation to the population of the districts in which they occur, the difference between the large towns and rural districts appears still more striking. For instance, the deaths during this period of life in Liverpool are 176 annually for each 10,000 of the inhabitants; whilst in Surrey they are only 58, or less than one-third the number.
It is perhaps not very generally known that, at one period of life, a rule pretty generally obtains just the reverse of that considered above; and that the mortality is greater in the rural districts than amongst the inhabitants of London and certain other large towns.
On glancing the eye over the table below, showing the mortality of London, as contrasted with that of the extra-metropolitan part of Surrey, at various periods of life, it will be observed that the mortality of the country population rises at a certain period above that of the town. In the first part of the table [No. I], in which the deaths at different ages are compared with the total mortality, the proportion of deaths in Surrey begins at five years to rise above that of London, and continues above it to the age of twenty-five. Amongst females, this elevation of the mortality in Surrey is greater than amongst males. In the second part of the table [No. II], in which the mortality at different ages is compared with the entire population, the deaths from ten to fifteen are higher for both sexes in Surrey than in London, and from fifteen to twenty-five they are higher for the female sex. After the age of twenty-five the mortality of London rises again above that of Surrey, and continues above it till about sixty or seventy years of age, when it falls again, on account of the smaller number of persons who attain to old age in the metropolis. The greatest number of deaths amongst males in any decennial period, after the age of five years, occur in London between thirty-five and forty-five years of age; whilst in Surrey they occur between sixty-five and seventy five, or thirty years later. Amongst females, however, the greatest mortality in any decennial period, after the age of five, takes place in London from sixty-five to seventy-five, and in Surrey from seventy-five to eighty-five, only ten years later.
The first two parts of this table have been calculated from the tables of population and mortality in the ninth annual report of the Registrar-General. The third part of the table [No. III], where the mortality is shewn with reference to the numbers living at each of the ages specified, is copied from the ninth annual report of the Registrar-General before-mentioned, where the numbers are ready worked out. Examined in this point of view, it is only in the female sex that the mortality of Surrey rises above that of the metropolis. This takes place between the ages of ten and twenty-five, to a considerable extent, as shown by the table and the diagram by which it is illustrated.*
(* Illustrative diagrams were illustrated at the meeting of the Epidemiological Society, at which this paper was read.)
If some of the most unhealthy parts of the metropolis are compared with the more distant and rural part of Surrey, the mortality at the period of life immediately succeeding to puberty, is found to be still more in favour of the town and against the country, comparing it even with the numbers living at that particular age. This is the case in both sexes, but in the most marked degree in the female sex. For instance, the annual deaths in Sr. Giles', amongst males, between the ages of fifteen and twenty-five, in the seven years 1838 to 1844 inclusive, were [0].589 per cent or not quite fifty-nine in 10,000, and in Clerkenwell they were [0].769 per cent or not quite seventy-seven in 10,000; whilst in the registration district comprising Guildford, Farnham, and Hambledon, in Surrey, the mortality was [0].775 per cent or over seventy-seven in 10,000. Amongst females, the annual mortality at this period of life was only sixty-eight in 10,000 in St. Giles', and sixty-three in 10,000 in Clerkenwell; whilst in the Guilford district it was at the rate of ninety in 10,000 living at the same period of life.
In some of the large manufacturing towns, as Manchester and Liverpool, the mortality is high at every period of life, when compared with those living at each period, but in the first ten years after puberty it is low as compared with the total mortality; for instance, the annual deaths in Manchester, in both sexes, between the ages of fifteen and twenty-five, during the seven years alluded to, were 586 in 10,000 deaths at all ages, and in Liverpool 548, whilst in Wiltshire they were 825.
In Manchester and Liverpool, the greatest mortality in any decennial period, subsequent to five years of age is from thirty-five to forty-five in males, the same as in London--that is comparing, the deaths at this decennial period with the whole deaths, or with the whole population; but in females the greatest mortality is from twenty-five to thirty-five, whilst in London it is from sixty-five to seventy-five,--forty years later. In Sheffield it is the same as in Manchester and Liverpool. In Huddersfield the greatest mortality amongst females is also from twenty-five to thirty-five, whilst amongst males it is from sixty-five to seventy-five, the same as amongst males in Surrey. In Leeds the greatest mortality in adults of both sexes is from fifteen to twenty-five, although there are two districts within twenty miles of it, viz., the Pateley Bridge and the Skipton districts, in which the chief mortality is from seventy-five to eighty-five, or sixty years later than at Leeds. I once lived at Pateley Bridge, near to the church, and remember that a great proportion of the funerals were those of old people, who died, as it was said, of old age, without having had any medical attendance. In the ninth annual report there are six Lancashire towns standing in one dreadful row, at page 232, in all of which the greatest mortality in adult life, in both sexes, is between the ages of fifteen and twenty-five, as at Leeds: they are Blackburn, Preston, Chorley, Rochdale, Bury, and Bolton. Stockport and Macclesfield, in Cheshire, are also in the same predicament. At Nottingham, although a manufacturing town, the highest mortality amongst adults is from sixty-five to seventy-five, in both sexes, or fifty years later than in the towns just enumerated. The highest mortality amongst adults in Birmingham is from thirty-five to forty-five in males, and from sixty-five to seventy-five in females, the same as in London, to which it nearly approaches in point of general salubrity.
The circumstance previously alluded to of the lower rate of mortality amongst young persons, in some of the worst districts of London, than in the most salubrious parts of Surrey, is of considerable interest. There has long been a popular impression that living in town is of itself injurious to people of all ages; and there are hundreds of young men with limited means and not much leisure, who spend a good deal, both of money and of time, in getting a little way out of town every evening by omnibus or other means, and returning in the morning, for the benefit, as they suppose, of their health, whilst they are just of the age when the mortality is less in the town than out of it. If they obtained exercise or fresh air by the journey, it might be an advantage; but it is doubtful whether they do.
It is pretty generally believed that the excess of mortality in large towns, over that of rural districts, is chiefly if not altogether due to certain physical conditions, which might be removed by what are called sanitary measures. In fact, this excess of mortality is sometimes spoken of as the removable part of the mortality of the towns. Now, I do not deny either the necessity or utility of well devised measures of sanitary reform; and, in a former paper, I endeavoured to show how such measures might assist in preventing the spread of cholera; but I would suggest that the chief causes of the difference of mortality between the town and the country are not the external physical conditions alluded to. If the excess of deaths in London over those in Surrey depended altogether on chiefly in overcrowding, want of drainage, noxious effluvia, or deficient or bad supply of water, they ought to affect persons of every age, more or less; and although people, might be better able to resist such influences at one period of life, than at another, they cannot be the cause why young men and women are absolutely subject to a lower mortality in Clerkenwell and St. Giles' than in the healthiest parts of the country.
That the higher mortality of towns does not arise merely from living in the towns, is apparent on examining one town with another. From some of the figures given above, it will have been noticed that a very great difference exists in the mortality of various towns. London, which is prodigiously larger than any of the great provincial towns, has a much lower mortality than they have. Bath, Brighton, Wolverhampton, and Norwich, are almost the only towns with 50,000 inhabitants that have a lower mortality than London; and 50,000 is only about two per cent of the population of this metropolis. In London, the mortality amongst females, between fifteen and twenty-five years of age, is lower than in the rural districts; but in the towns w[h]ere textile fabrics are manufactured, the mortality at this period is higher. It is most likely that the mortality at every period of life is influenced more by the habits, occupations, and pecuniary circumstances of the people, than by any other causes. Indeed, when the vital statistics of different trades and occupations have been collected, this has been shown to be the case.
By examining the registration returns of the causes of death, we may expect to arrive at the circumstances which influence the mortality in town and country.
The tenth annual report of the Registrar-General contains tables of the causes of death, in the year 1847, for the metropolis and large divisions of the country, arranged according to the ages in the mortality tables in the ninth report, from which I have quoted above. I have compared the table for London with that for the South Midland division, adjoining to London, which comprises part of Middlesex, and the counties of Hertford, Buckingham, Oxford, Northampton, Huntingdon, Bedford, and Cambridge. The population is chiefly rural, but includes that of the towns of Oxford, Cambridge, and Northhampton, besides the considerable suburban districts of Brentford and Edmonton.
The diseases which are most fatal in infancy and early childhood, are bronchitis and pneumonia, convulsions, diarrhœa, hydrocephalus, hooping-cough, and the irruptive fevers. On reducing the number of deaths in 1847, from each of these disease, in London and the South Midland district, to a per centage of the entire population of each place, I find that every one of them is more fatal in London than in the country district, many of them being considerably more than twice as fatal.
The following table shews the deaths from the above-named diseases, under five years of age, in 100,000 of the population in London and the South Midland district respectively.
The diseases which cause the mortality between 15 and 25 to be higher in the South Midland district than in London, are typhus and phthisis. The deaths in 1847 from typhus in London were 144 to 100,000 of the population, whilst in the South Midland district they were 169. Between the ages of 15 and 25 they were 19 in London and 34 in the South Midland, or nearly twice as many. The deaths from phthisis at all ages were 319 in London, and 298 in the South Midland district; but between the ages of 15 and 25 these proportions are reversed, being 57 in London and 72 in the South Midlands. It is necessary to consider phthisis in the two sexes separately, for there is a wide difference between London and the country in the proportion in which this disease affects males and females. The deaths amongst males [22/23] from phthisis in London, in 1847, were 172 in 100,000 of the population, and in females 146; in the South Midland district the numbers were 124 males and 173 females; the proportions being just reversed, and the deaths from phthisis in the county district amongst females being just one more than amongst males in London. On ascertaining the deaths from phthisis in each sex, in town and country, between the ages of 15 and 25, it is evident how much this disease contributes to reverse the ordinary relation of mortality at this period. In London, the numbers are--males, 25; females, 46. In the South Midland district--males, 25; females, 46. So that, in the country district, a considerable proportion of the females who die of phthisis die earlier than the males, and earlier than both males and females in London. It will be recollected that it is more particularly in females that the country mortality rises above that of London at the period just succeeding puberty. It is chiefly to phthisis that the great mortality previously alluded to, in early adult life, in many of the manufacturing towns, is due.
The great mortality amongst infants in large towns is no doubt very much due to improper nourishment and want of proper attention in general. More children are deprived of breast milk in London than in the country: the vice of dram-drinking, so common amongst women belonging to the working classes in large towns, is almost unknown in rural districts; and this habit must influence such children as are suckled. In the country, also, the people have some traditional knowledge of the way in which an infant ought to be fed, whilst the poor people in large towns give it "anything that is going," to use their own expression, and feed it with the most stimulating and indigestible food. All these causes cannot fail to increase the frequency of convulsions, hydrocephalus, and diarrhœa. Another cause of the great mortality of infants in large towns is that the various infectious diseases are constantly present, and the children nearly always have them whilst young. Hooping cough and measles are much more fatal in infancy than in children a little more advanced; and in rural districts, where these diseases pay only occasional visits, a certain number of the children escape being attacked by them till a period when they are but little dangerous. In proof of the earlier average attack of these infectious diseases in large towns, I may adduce the fact, that the deaths from scarlet fever between the ages of 10 and 20 are much greater in the South Midland district than in London, the proportions being--South Midland 62, and London 38, in 1,000,000 of the population; whilst, under the age of 5, this disease is much more fatal in London than in the South Midlands.
I believe that the reason of the continued fevers which are grouped together under the name of typhus being more fatal in the country than in London, is similar to that just mentioned, only operating in the opposite direction. Typhoid fever is much less fatal in childhood, when it passes under the name of infantile remittent, than in adult life; and one sees it often enough in children to render it probable that a considerable number of the population of towns gain an immunity from it in after life, by having passed though it at an earlier and safer period.
The greater prevalence of phthisis amongst males in London than in the rural districts, may be easily explained by the in-door employments generally followed, as contrasted with the exercise in the open air of the country; but how can we explain the greater mortality of this same disease in the country amongst females? One prevalent theory of the cause of phthisis is, that it is occasioned or promoted by deficient ventilation; and, as far as males are concerned, in town and country, the facts support the theory. But, amongst females, the disease is more fatal in the rural districts than in London; although it cannot be supposed that the females in the country suffer more from confinement indoors, or want of fresh air, than in London. The causes of phthisis are involved in great obscurity; but my own impression of the probable cause of its great fatality amongst young women in the rural districts is, that it arises from insufficient nourishment. Poverty and misery have at all times been the lot of a great portion of mankind, and they fall most heavily upon those who cannot obtain employment. When a piece of bacon or cheese reaches the cot of the peasant, it must be reserved for the man, to enable him to work for his family, who must often be content with a scanty allowance of meal and potatoes. The boys often get a little work and food at the neighbouring farm, whilst the girls must still remain at home till old enough for domestic service; and the health often gives way at the time when the girl should change into a woman.
I have been able to give but a very brief outline of a very extensive and important subject, but I hope that the labours of the members of the Epidemiological Society will, sooner or later, make up in a great measure for my deficiencies.
THE END
Go to Group 8 (# 87a)
Click to return to Stream 1 - d: John Snow's Publications
Click to continue to Stream 1 - e: Memoir of his friend Benjamin Ward Richardson
 (# 76-86)
(# 76-86) Return to John Snow Publications
Return to John Snow Publications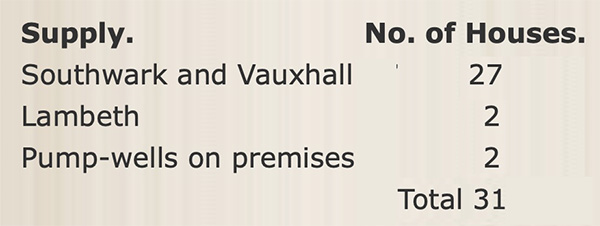
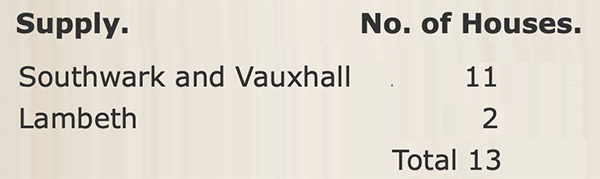
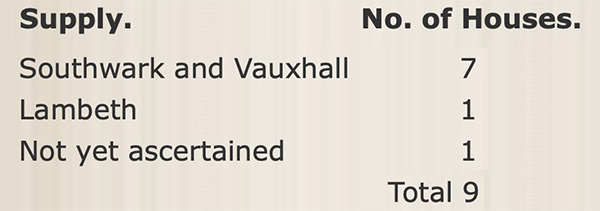
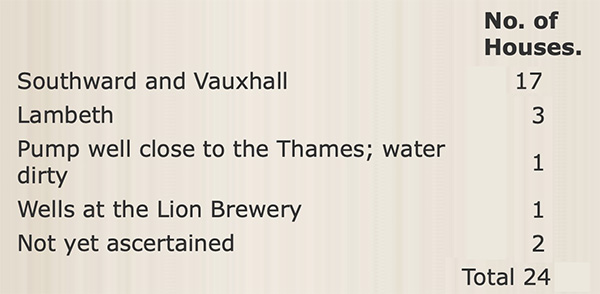
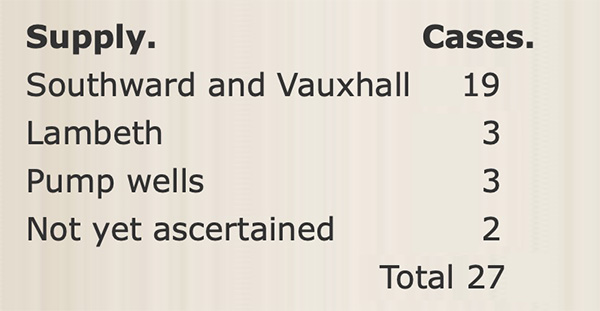
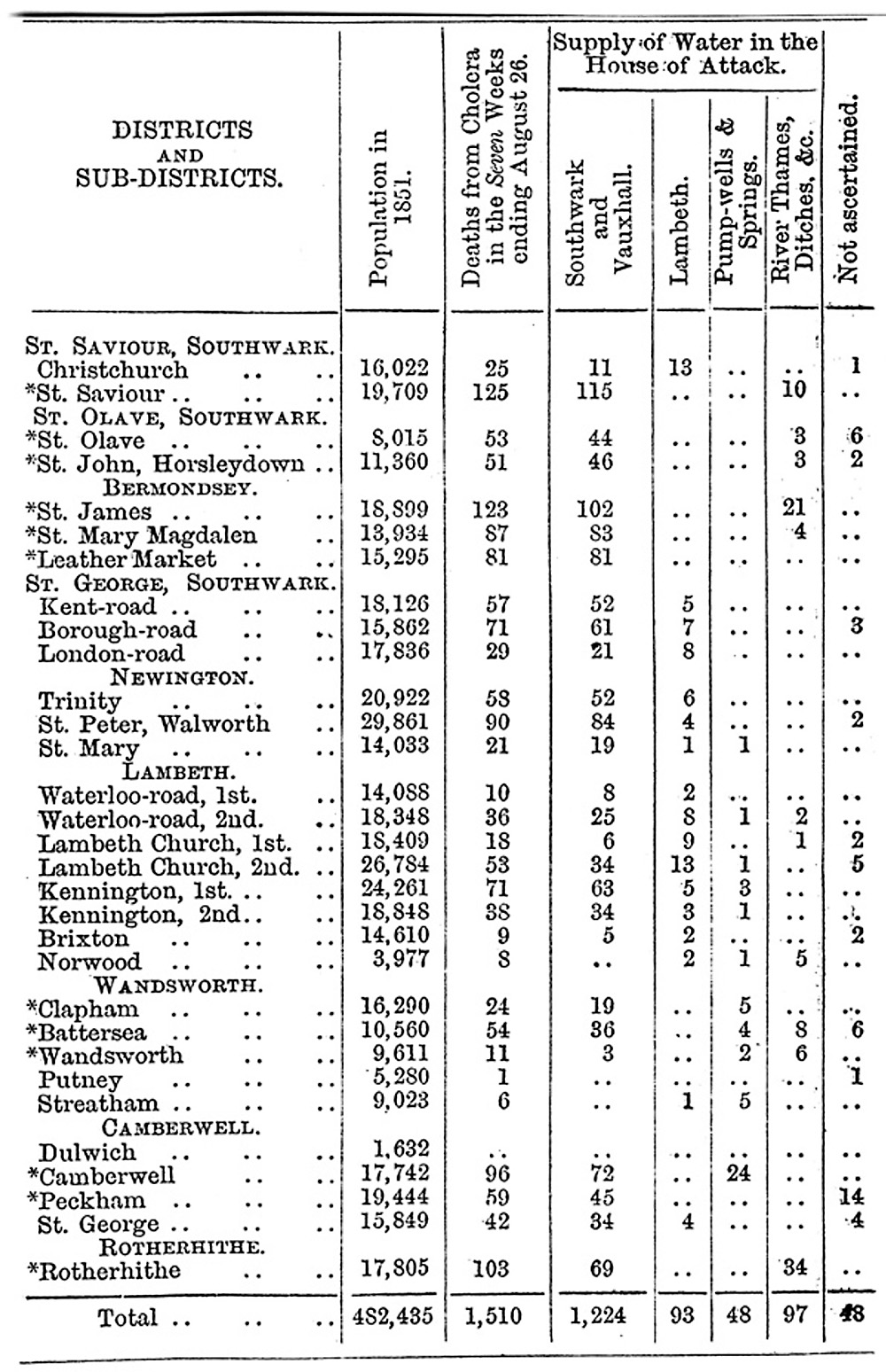
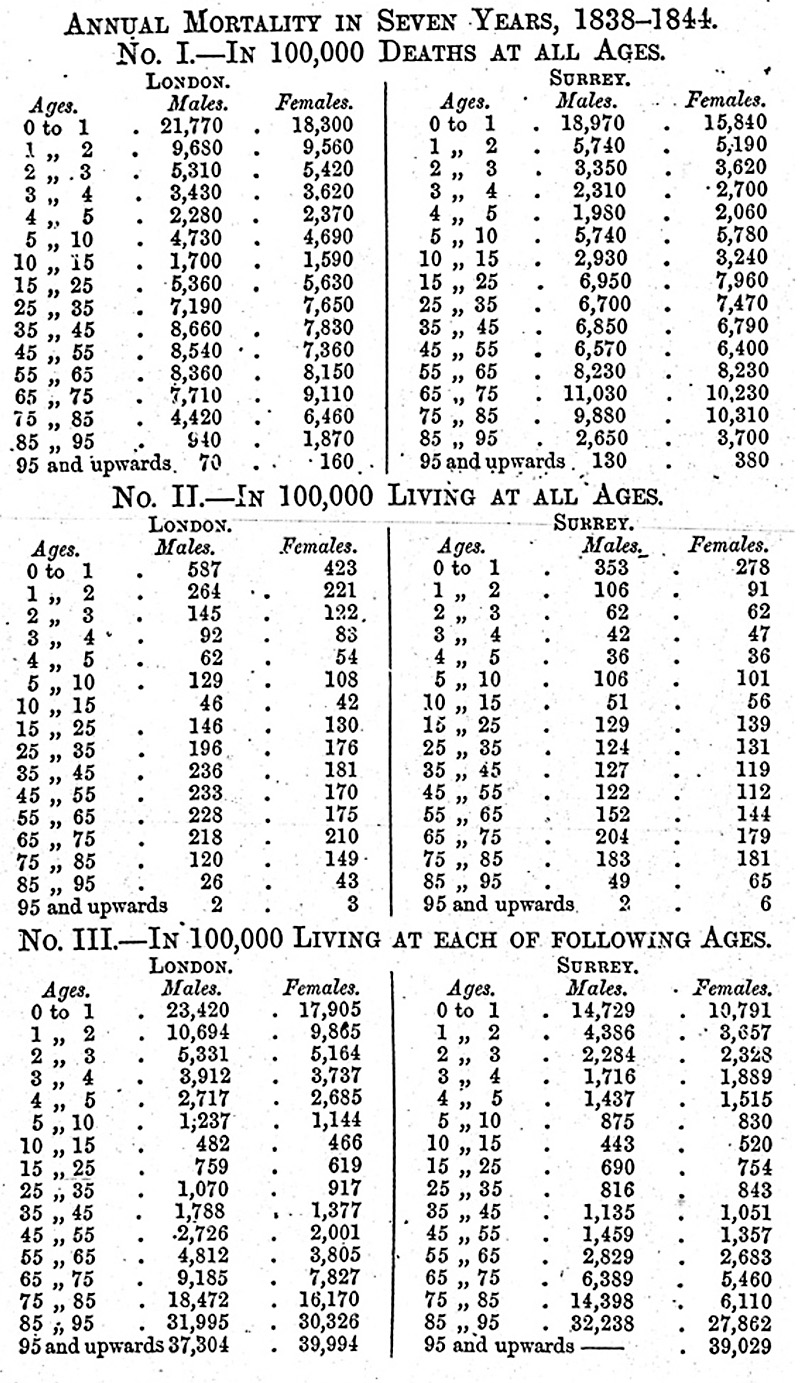
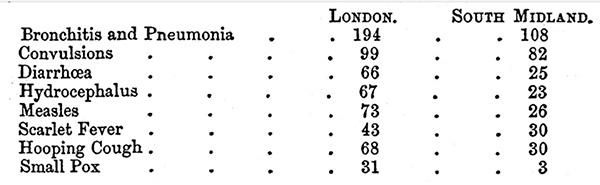
 (# 87a)
(# 87a)
