Source: Snow, John. London Med. Gazette, vol. 44, Aug. 17, 1849, pp. 272-77
(part 12).
46. On narcotism by the inhalation of vapours
By John Snow, M.D.
Vice-President of the Westminster Medical Society.
[PART 12]
Further remarks on Dutch liquid--its chemical constitution--its physical properties--its narcotic power compared with that of chloroform--Cases of its administration in tooth-drawing, in midwifery, in cholera--Conclusions.
In a former paper (London Medical Gazette Vol. xliii. p. 331, part 4, 25 August 1848), I gave an account of two or three experiments on small animals with Dutch liquid, by which it was shown that its narcotic properties were of a favourable kind, but that it caused inflammation of the lungs. This latter effect, as I have since ascertained, was occasioned by some impurity--probably sulphurous acid gas--in the specimen of Dutch liquid I then used. I made it myself, by getting the olefiant gas and chlorine to combine in a glass globe, as recommended in Fownes' Chemistry. The olefiant gas was passed through sulphuric acid to separate ether and alcohol, but the sulphurous acid was not separated from it, and I endeavoured to separate that and the hydrochloric acid from the products, when formed, by washing it two or three times in water, but did not succeed, as it since appears. On Mr. Nunnelly recommending Dutch liquid for inhalation last February, it occurred to me that neither the specimen which I had made, nor that used by Dr. Simpson, could have been pure. I accordingly made some more in the same manner as before, but washed it in a weak solution of carbonate of soda previous to distilling it from chloride of calcium. I now got a much less pungent substance,--similar, in fact, to that which I have since received from Mr. Morson and Mr. Bullock. On performing some experiments with it, I found that it possessed the properties which I previously described, with the exception of the irritant ones. I inhaled a little of it myself; but the process of making it being very troublesome and tedious, I had not enough to try its effects in practice till half an ounce was kindly given to me by Mr. Morson on the 20th March, which I used in four cases of tooth-drawing in St. George's Hospital, on the following morning. I have since received several supplies from Mr. Bullock, and have used it in a variety of cases; but, before I describe the results of its application it will be more convenient to give an account of its chemical constitution and those of its physical properties which are intimately connected with its physiological action.
It was discovered in 1795 by the associated Dutch chemists, Bondt, Deiman, Vantroostwyk, and Lauwerenburgh. It is formed by the combination of two volumes of chlorine and two of olefiant gases. The latter, representing one atom, contains four atoms of carbon and four of hydrogen, and is considered to be a hydruret of acetyle,--acetyle being a hypothetic base consisting of four carbon and three hydrogen. When the two atoms of chlorine combine with the hydruret of acetyle, the following is, since the investigations of Regnault, believed to be what takes place. One atom of chlorine displaces an atom of hydrogen, and the hydruret of acetyle is converted into chloride of acetyle, whilst the other atom of chlorine combines with the displaced hydrogen, forming hydrochloric acid, and the two products at the same time uniting, hydrochlorate of chloride of acetyle is the result; and this is the chemical name of Dutch liquid in recent authors. This body is curiously connected with the discovery of chloroform, as was pointed out by Dr. Pereira in a communication on the history of the latter medicine.* (Med. Gaz. vol. xi. p. 953.) Dr. Thomas Thomson, in the edition of his Chemistry published in 1810, gave the name of chloric ether to Dutch liquid, and stated that a solution of it in spirit was useful in medicine as a diffusible stimulant. Some years after this, Mr. Guthrie, a chemist in America, obtained the liquid by the distillation of spirit and water with bleaching powder, which he considered to contain the chloric ether of Dr. Thomson dissolved in spirit; and this product, [272/273] which, in fact, consisted of chloroform and alcohol, was used for some time in medicine under the name of chloric ether. In 1831, Soubeiran found that this preparation did not contain Dutch liquid--the chloric ether of Dr. Thomson; and the following year Liebig also made an analysis of it; but, failing to discover the hydrogen in the chloroform, he considered that it was composed of chlorine and carbon; and after this time the medicine was often called ter-chloride or sesqui-chloride of carbon. There are various chlorides of carbon which have been discovered by Faraday and Regnault; but they are very difficult to make, and I believe that none of them have ever been on sale, either for medical or other purposes, and that the so-called chlorides of carbon which have been used in medicine were all of them solutions of chloroform, of which body Dumas was the first to ascertain the true nature and composition.
Dutch liquid is somewhat heavier than water, having a specific gravity of 1.247. It boils at 180? Fah. It is very sparingly soluble in water, and the specific gravity of its vapour is 3.4484. In sensible properties it very nearly resembles chloroform; and hence probably the reason of Mr. Guthrie, when he discovered the latter substance, mistaking it for Dutch liquid. The odour is not quite so fruit-like as that of chloroform, and the vapour feels less pungent; but the reason of this is that a smaller quantity of vapour is given off from Dutch liquid than from chloroform; for I find that when the two vapours are diluted to the same extent--for instance, till the air contain five per cent and inhaled from a balloon, there is then no difference in the pungency. The physical properties of Dutch liquid which are most intimately connected with its narcotic action, when inhaled, are its volatility and solubility. From some experiments before related it was concluded that in the second degree of narcotism the blood contains one-fiftieth part as much as would dissolve, and in the fourth degree one twenty-fifth part. These experiments have been repeated with the liquid quite free from impurity, and the results obtained were the same.
I have endeavoured to ascertain the solubility of Dutch liquid as accurately as possible, by admitting small quantities of water to air saturated with the vapour, and confined over mercury in a graduated receiver. The average of a number of experiments gives 1.7 volume of vapour as the quantity that one volume of water will dissolve; and, the liquid being 321 times as heavy as its vapour at 100?, it results that, at this temperature, one part of the liquid would require 189 parts of water to dissolve it.
If the average quantity of serum in the body be assumed to be the same as in treating of chloroform, and a calculation be made of the kind there given,* (*Med Gaz Vol. xli. p. 850. [part 1, 19 May 1848]) it will be found that the amount of Dutch liquid in the blood, in the second degree of narcotism, is rather more than twenty minims, and in the fourth degree forty-one minims. In the third degree the amount would be intermediate, viz. about thirty minims. These quantities are nearly twice as large as in the case of chloroform; and this agrees exactly with what I have met with in practice, since nearly twice as much Dutch liquid has been required to cause insensibility as would have been required of chloroform. To estimate the strength of this substance when inhaled, its volatility requires to be taken into account, in addition to the above data. Whilst 100 cubic inches of air at 60? will take up 14 cubic inches of chloroform, they will only take up seven cubic inches of Dutch liquid; and the vapour, moreover, is not so heavy as that of chloroform,--consequently it is not half so volatile. This makes the difference in strength between the two agents still greater. To exhibit more accurately their relative power, the quantity of air may be calculated that a patient would require to breathe, when saturated by either of the two vapours at 60?, in order to be rendered insensible. Eighteen minims is the average amount of chloroform in the blood in the third degree of narcotism, the stage usually required for a surgical operation, and as about as much is expired again without being absorbed, thirty-six minims is about the quantity inhaled before an operation. This would require only 257 cubic inches of air to take it up if saturated at 60?, the air becoming expanded to 294 cubic inches.
Thirty minims of Dutch liquid require to be absorbed, as stated above, to induce the same amount of insensibility, and sixty minims would have to be inhaled. This quantity requires 904 cubic inches of air to allow it to be converted into vapour at 60?, the air being expanded to 967 cubic inches, an amount more than three times as great as requires to be inhaled in the case of chloroform; and consequently Dutch liquid has less than one-third the power of the former when inhaled in a similar way. Sulphuric ether is rather stronger than Dutch liquid--the quantity of air saturated with its vapour that is required to induce insensibility being rather more than 800 cubic inches.
For the reasons given above, Dutch liquid is much slower in its action than chloroform;* and whilst the chief endeavour in giving chloroform is to prevent the air from getting too strongly charged with the vapour, in giving Dutch liquid the endeavour is to get the air to take up sufficient of it. (* A preparation consisting of equal parts of chloroform and spirit was fraudulently introduced into the drug-market last spring, and sold to a considerable extent as Dutch liquid, although not containing any of that body. This counterfeit liquid would cause insensibility with nearly the same rapidity as chloroform.) In one case, indeed, that of an infant in King's College Hospital, on which Mr. Fergusson operated for nævus, it failed to induce insensibility with the inhaler I was using (one contrived for chloroform), although continued for three or four minutes, and rather than cause further delay chloroform was used.
For reasons similar to those which render Dutch liquid slower in its action, when its effects are once produced they are more persistent than those of chloroform. Medicines so volatile as these escape from the system almost exclusively by the lungs; and as the quantity of Dutch liquid in the blood during insensibility is greater than that of chloroform, it would be longer in escaping, even if it could be exhaled at the same rate; but, being less volatile, it cannot. There is a continual tendency to equilibrium between the elastic force of the vapour in the blood and that in the air contained in the pulmonary cells: and if the blood contain, for instance, one-thirtieth part as much of a volatile liquid as it could dissolve, each cubic inch of air which reaches the cells of the lungs is capable of taking up one-thirtieth part as much as would saturate it at 100?; but this quantity is twice as great in the case of chloroform as in that of Dutch liquid. The longer duration of the effects of the latter substance as compared with the former has been very marked in a number of experiments on animals, as well as in practice.
Although, as stated, a greater quantity of Dutch liquid than of chloroform is required to induce insensibility in the first instance, yet in cases requiring the continued inhalation of the vapour there is but little difference in the amount used; since from the more persistent effect of Dutch liquid, it does not require to be repeated so often.
The following are the cases in which I have tried the effects of Dutch liquid:-
1. On March 21, 1849, a young woman, about 25 years of age, inhaled it, in the out-patients' room of St. George's Hospital, previous to having a tooth drawn. She was nervous and hysterical, and was alarmed at the inhalation, although very anxious to avoid the pain. She inhaled from the apparatus described before,* between one and two minutes, when she strongly requested to leave off. (* Vol. xlii. p. 843. [part 7, 17 November 1848]) The tooth, a first lower molar, firmly fixed, was immediately extracted with the forceps by Mr. Parkinson, dresser to the surgeon for the week. The patient cried out slightly as the tooth came out. She said afterwards that the removal of the tooth did not hurt her so much as the lancing of the gum on a previous occasion. In a few minutes the partial stupor caused by the vapour had subsided. This patient was not rendered quite unconscious, but the sensibility, and consequently the pain, were apparently diminished.
2. Another young woman inhaled the Dutch liquid immediately afterwards. She breathed it very steadily. The pulse became increased a little in frequency and force soon after she began to inhale, and the face at the same time became slightly flushed. There was no further symptom, and no alteration in her appearance till nearly four minutes had elapsed, when volun-[274/275] tary motion ceased in the eyes and eyelids, and the pupils were turned upwards. The inhalation was now discontinued when she had inhaled just four minutes. The muscles of the jaw were rather rigid, but the mouth was easily opened by making a little pressure on the chin, and a bicuspid tooth was extracted with the forceps by Mr. Parkinson, without causing the least flinch, cry, or altered expression of countenance on the part of the patient. Immediately after the tooth was extracted she opened her eyes, looking bewildered at first, but in one minute after the inhalation ceased she regained her usual expression, and began to wash out her mouth. She said that she had felt nothing. Three minutes afterwards she left the hospital feeling well. The narcotism, in this case, just reached the third degree, and there was complete immunity from pain, as indeed there generally is under the effects of chloroform carried to the same extent, when it is inhaled slowly. The recovery was as prompt as it usually is from chloroform; but it should be noticed that when the inhalation of that vapour is left off just when the symptoms reach the point indicated in the above case, the patient usually begins to recover immediately, even before there would be time to extract the tooth. Two fluid drachms of Dutch liquid had been put into the inhaler, and it was not quite all used by these two patients. A drachm more was added when the next patient commenced to inhale.
3. This patient was a labouring man, between 30 and 40 years of age. Soon after beginning to inhale he commenced to laugh, and he kept the corners of his mouth stretched so widely apart that it was difficult to make the face-piece fit exactly. In about five minutes he appeared to have lost his consciousness, and he muttered incoherently. He soon afterwards became unruly, and was with difficulty kept in the chair. The conjunctiva remained sensible, and he flinched when a hair of his face was pulled. Although he inhaled a few minutes longer, he did not become further affected; the reason of this being, as I afterwards found, that the Dutch liquid in the inhaler was finished. There was great difficulty in getting the mouth open, not from spasm but from voluntary resistance exerted under the influence of some obscure dream. The patient flinched as the tooth was extracted; but on recovering his consciousness two or three minutes afterwards, he said that he had felt nothing. The truth probably is, that the feeling had been obscure, and there was no recollection of it. He complained, however, of giddiness, and began to look pale and sick. In a few minutes he vomited, and then complained of headache. He was complaining of headache and sickness half an hour afterwards, when I left him, expecting that these symptoms would soon subside. But I afterwards found that they continued so severe, with occasional vomiting, that he was kept in the hospital till the following morning, when he left, but came back in the forenoon, complaining that he could not go on with his work. Mr. Hammerton ordered him some medicine containing ammonia, and directed him to return the next morning if he should not feel well. He did not apply again.
This is the only case in which I have seen Dutch liquid followed by distressing sickness or headache; and the result might have been the same if chloroform or ether had been used, as such symptoms do now and then follow their use, though rarely to the same extent as in this case.
4. In the above cases the water bath of the inhaler was at the temperature of 60?; in this case it was raised to 70?. Fifty minims of the medicine were put into the inhaler, and a little girl, six years old, inhaled for two minutes. At the end of this time she became insensible, the pupils of the eyes being turned upwards. A decayed molar tooth was extracted without causing the least flinch or cry. In about a minute after the inhalation ceased, the child became conscious, but staggered on attempting to walk. She vomited a little, two or three minutes after this, but in a few minutes more was free from sickness, and pretty well. The fifty minims were not all consumed by this patient.
5. The subject of this case was a patient of Mr. Marshall, of Greek Street, in labour with her second child, on April 24. I exhibited twenty minims of Dutch liquid (all I had with me at the time) during the last three or four pains which expelled the fœtus. The [275/276] patient ceased to complain, but continued her expulsive efforts. She was not rendered quite unconscious, but her suffering were greatly alleviated, being, as she said afterwards, much less severe than before, whilst without the inhalation they would have been much greater. Mr. Marshall was present and attending to the labour. In this and the next three cases the vapour was administered by means of a small inhaler, which I commonly use for giving chloroform in midwifery cases; it consists of the same face-piece which forms part of my other inhalers, and of a short curved metallic tube, lined with bibulous paper.
6. Having expressed a wish to Dr. Murphy, Professor of Midwifery in University College, to try Dutch liquid in some cases of labour, I was called on by him on the day on which the last of the above cases occurred, and accompanied him to a patient of Mr. Jakins, of Osnaburg Street, who had been forty-eight hours in this, which was her first labour. Dr. Murphy, who is about to give the particulars of this and the next case to the profession, found it necessary to divide a thick dense band, extending across the vagina, and also to make an artificial os uteri, and deliver with the forceps. Half a drachm of the liquid being inhaled, it gradually induced a state of unconsciousness, during which the speculum vaginæ was introduced; the uterine contractions and slight expulsive efforts continued as before. A little more Dutch liquid was put into the inhaler, from time to time, so as to keep the patient unconscious. The pupils of the eyes were turned upwards during part of the time. No mental excitement or muscular rigidity was occasioned. Dr. Murphy proceeded to make an artificial os uteri, and to divide the ligamentous band. These operations were partly performed when my stock of Dutch liquid, about three fluid drachms, was all used. It had kept up insensibility for about an hour. Chloroform was now given, so as to keep the patient constantly insensible to the end of the delivery. There was little appreciable alteration in the symptoms on passing from the use of one vapour to that of the other. The effects induced were of the same kind, but they were produced with much less inhalation in the case of chloroform; a few inspirations, now and then, with the valve partly open, sufficed instead of the previous more lengthy inhalation, with the valve closed. The delivery was effected with the forceps about an hour after the inhalation of chloroform commenced, half a fluid ounce of which was used, being a larger quantity than was used of Dutch liquid in the same period; but the patient was kept more deeply insensible during the whole of this latter period than in some part of the first hour, when the operation had not yet commenced. The child was born alive, but breathed feebly, and died next day. The placenta was expelled without hæmorrhage a few minutes after the birth of the child. The patient was quite conscious ten or fifteen minutes after the inhalation was discontinued; and after being bandaged and placed in a comfortable posture, she fell asleep, and slept almost uninterruptedly for twelve hours. She recovered favourably.
7. On May 18, I administered the Dutch liquid at the request of Dr. Murphy, to a primipara, 35 years of age, who had been 48 hours in labour, when he resolved to deliver with the forceps. Half a drachm was put into the inhaler: the patient objected to the vapour at first, on account of its pungency, but afterwards inhaled readily, and in about two minutes appeared unconscious, the pupils being turned upwards, and the eyelids firmly closed, and resisting the attempt to open them. Dr. Murphy now began to introduce the forceps, and the patient cried out a little: another half drachm of the liquid was put in, and she soon became quiet, and was kept insensible till the birth of the child, which was effected in less than half an hour. She talked in a rambling manner about some ordinary topic once or twice during the inhalation, and also a few minutes after it was discontinued. Two fluid drachms were used in all. The placenta was expelled ten minutes after birth of the child; soon after this the patient vomited; and fifteen minutes after the birth (the time when the inhalation was left off), the patient began to regain her consciousness. She recovered very favourably, and the child is living.
8. The Dutch liquid was administered in a case of cholera that Mr. Marshall Greek Street, requested me to see with him. The patient was a child seven years old, which had been ill twelve hours. The stools were copious and watery, and devoid of fæcal colour or odour; the vomiting was constant and severe; the features were sunken, and the pulse was about 160 in the minute, and so feeble as to be felt with difficulty. There were jactitation and great uneasiness, the latter probably resulting from cramps. Twenty minims were inhaled, which produced a state of unconsciousness and quiet, from which the little girl awoke in ten minutes. The same quantity was again inhaled, with a like effect, and of rather longer duration. The pulse was improved by the inhalation, being rendered stronger and less frequent; but the chief symptoms of the disorder went on as before. The child recovered.
The relief from inhalation of chloroform in cholera has generally been greater than this in the cases I have witnessed, the unconsciousness having generally merged into a natural sleep, of from half an hour to two hours and a half in duration, during which time of course the patients were free both from sickness and spasm. Two of the cases were also under the care of Mr. Marshall. I attribute the different action in the above case to some difference in the state of the patient, rather than in the properties of the narcotic.
9. On July 18, a boy, nine years old, inhaled Dutch liquid in the out-patients' room of St. George's Hospital, from the balloon described in my last communication. Each hundred cubic inches of air in the balloon contained four minims of the liquid, or a small fraction over four cubic inches of the vapour. In two minutes consciousness was removed; he then began to resist the further inhalation, but with a little trouble was got to inhale two minutes longer. He was not narcotized beyond the second degree. Voluntary motion was never abolished, but the sensibility of the conjunctiva was diminished. Two incisor teeth of the first set were extracted without being felt (probably without the inhalation there would have been no great pain). He was laid on the bed, and in two minutes recovered his consciousness, but staggered on getting up. In about ten minutes the effects of the vapour had apparently gone off. He inhaled about 1000 cubic inches, and consequently 40 minims of Dutch liquid; this quantity of chloroform would have rendered an adult twice his weight fully as insensible as he was, if not more so.
The result of my observations and investigations is, that I cannot unite with Mr. Nunnelly in his general praises of Dutch liquid. The only advantage which it possesses over chloroform, in any case, are such as are connected with its slower action and more persistent effects,--properties that Mr. Nunnelly failed to recognize. In all other respects its effects appear to be the same as those of chloroform. It is undoubtedly a very safe anæsthetic; but I doubt very much whether practitioners would be content to wait for its slower action, after they have been accustomed to use chloroform, even if it could be obtained at the same cost, of which there is no prospect. In whatever way Dutch liquid might be used, it would not suddenly occasion a fatal accident without giving due warning; in this respect it resembles ether. Advantages might be taken of its more persistent effect in some operations in the face, in which it is difficult to administer a vapour after the surgeon commences; and also in cases in which the operator is without an assistant, and has to make his patient insensible first, and then to perform his operation. In obstetric practice it would perhaps be more convenient than chloroform, when only one medical man is present, as he might intrust the inhaler to the nurse, and look up two or three times in a minute to give directions; but when there is a practitioner entirely to superintend the inhalation, chloroform has the advantage, as it can be given to the requisite extent just as each pain commences, and the patient can be allowed to recover from its effects, more or less, between every pain.
(To be continued)
Return to John Snow Publications
Source:"On the mode of communication of cholera." London: John Churchill, Princess Street, Soho, , September 1849, 31 pp.
47. "On the mode of communication of cholera," 1849
By John Snow, M.D.
It is not the intention of the writer to go over the much debated question of the contagion of cholera. An examination of the history of that malady, from its first appearance, or at least recognition, in India in 1817, has convinced him, in common with a great portion of the medical profession, that it is propagated by human intercourse. Its progress along the great channels of that intercourse, and the very numerous instances, both in this country and abroad, in which cholera dates its commencement in a town or village previously free from it to the arrival and illness of a person coming from a place in which the disease was prevalent, seem to leave no room for doubting its communicability.
It is quite true that a great deal of argument has been employed on the opposite side, and that many eminent men hold an opposite opinion; but, besides the objection that negative evidence ought not to overthrow that of a positive kind, the instances that are believed to oppose the proofs of communication are reasoned upon in the opinion that cholera, if conveyed by human intercourse, must be contagious in the same way that the eruptive fevers are considered to be, viz., by emanations from the sick person into the surrounding air, which enter the system of others by being inhaled, and absorbed by the blood passing through the lungs. There is, however, no reason to conclude a priori, that this must be the mode of communication of cholera; and it must be confessed that it is difficult to imagine that there can be such a difference in the predisposition to be affected or not by an inhaled poison, as would enable a great number to breathe it without injury in a pretty concentrated form (the immunity not having been earned by a previous attack, as in the case of measles, etc.), whilst others should be killed by it when millions of times diluted. The difficulties that beset this view are of the same kind, but not so great, as those which surround the hypothesis of a cholera poison generally diffused in the air, and not emanating from the sick.
Reasoning by analogy from what is known of other diseases, we ought not to conclude that cholera is propagated by an effluvium. In all known diseases in which the blood is poisoned in the first instance, general symptoms, such as rigors, headaches, and quickened pulse, precede the local symptoms; but it has always appeared, from what the writer could observe, that in cholera the alimentary canal is first affected, and that all the symptoms not referable to that part are consecutive, and apparently the result of the local affection. In those cases in which vertigo, lassitude, and depression precede the evacuations from the bowels, there is no reason to doubt that exudation of the watery part of the blood, which is soon copiously discharged, is already taking place from the mucous membrane; whilst in the cases in which the purging comes on more gradually, there is often so little feeling of illness that the patient cannot persuade himself that he has the cholera, or apply for remedies until the disease is far advanced, this being a circumstance which increases the mortality. The quantity of fluid lost by purging and vomiting, taking into consideration the previous state of the patient, the suddenness of the attack, and the circumstance that the loss is not replaced by absorption, has seemed sufficient, in all the cases witnessed by the writer, to account, by the change it must occasion in the quantity and composition of the blood,* for the collapse, difficulty of breathing, and, in short for all the symptoms, without assuming that the blood is poisoned, until it become so by the retention of matters which ought to pass off through the kidneys, the functions of which are, however, suspended by the thickened state of the blood, which will scarcely allow it to pass through the capillaries. (* The valuable analyses of Dr. Garrod have recently fully confirmed what had been stated in the former visitation of Europe by the cholera, viz., that the solid contents of the blood of patients labouring under this disease are greatly increased in proportion to the water--a state of the blood that is not met with in any other malady. [See Alfred B. Garrod, "On the pathological condition of the blood in cholera," LJM 1 (1849): 409-37])
It is generally assumed that the blood becomes so altered by the cholera poison, that its watery and saline parts begin to exude by the mucous membrane of the alimentary canal; but it is more consonant with experience, both therapeutical and pathological, to attribute the exudation to some local irritant of the mucous membrane; no instance suggesting itself to the writer in which a poison in the blood causes irritation of, and exudation from, a single surface, as in cholera; for the sweating, as the patient approaches to collapse, is only what takes place in other cases from loss of blood, during fainting, and in any state in which the force of circulation is greatly reduced.
Having rejected effluvia and the poisoning of the blood in the first instance, and being led to the conclusion that the disease is communicated by something that acts directly on the alimentary canal, the excretions of the sick at once suggest themselves as containing some material which, being accidentally swallowed, might attach itself to the mucous membrane of the small intestines, and there multiply itself by the appropriation of surrounding matter, in virtue of molecular changes going on within it, or capable of going on, as soon as it is placed in congenial circumstances. Such a mode of communication of disease is not without precedent. The ova of the intestinal worms are undoubtedly introduced in this way. The affections they induce are amongst the most chronic, whilst cholera is one of the most acute; but duration does not of itself destroy all analogy amongst organic processes. The writer, however, does not wish to be misunderstood as making this comparison so closely as to imply that cholera depends on veritable animals, or even animalcules, but rather to appeal to that general tendency to the continuity of molecular changes, by which combustion, putrefaction, fermentation, and the various processes in organized beings, are kept up.
Whilst it is matter almost of certainty that intestinal worms are in this way communicated, it is never possible to trace the communication from one person to another: hence, if this be the mode of the propagation of cholera, there must often be great difficulty in detecting it. That a portion of the ejections or dejections must often be swallowed by healthy persons is, however, a matter of necessity. The latter even are voided with such suddenness and force that the clothes and bedding scarcely fail to become soiled, and being almost devoid of colour and odour, the presence of the evacuations is not always recognized; hence they become attached unobserved to the hands of the person nursing the patient, and are unconsciously swallowed, unless care be taken to wash the hands before partaking of food: or if the person waiting on the sick have to prepare food for the rest of the family, as often happens, the material of communication here suggested has a wider field in which to operate; and where the patient, or those waiting on him, are occupied in the preparation or vending of provisions, the disease may be conveyed to a distance, and into quarters having apparently no communication with the sick.
All the observers who have recorded their opinions on the subject, agree in attributing a great influence to want of personal cleanliness in increasing the prevalence and fatality of cholera. Dr. Lichtenstädt, in a work on Cholera published in 1831, states, "that at Berditscher, in Volhynia, a place of a few thousand inhabitants, no less than 900 were attacked in thirty-one days. Amongst 764 of these were 658 Jews, and only 106 Christians, although the Jewish population is far from being proportionally so great; and among the Christians the deaths were 61.3 per cent., while among the Jews they were 90.7 per cent. The only reason assigned by the reporter for these extraordinary differences is the excessive disregard of cleanliness among the Jewish inhabitants."* (* Edin. Med. and Surg. Journal, vol. xxxvii.) The first appearance of cholera in many of the towns of this country in 1832 was in the courts and alleys to which vagrants resort for a night's lodging, where it often lingered for some time before spreading to the more cleanly part of the people.
The views here explained open up to consideration a most important way in which the cholera may be widely disseminated, viz., by the emptying of sewers into the drinking water of the community; and, as far as the writer's inquires have extended, he has found that in most towns in which the malady has prevailed to an unusual extent this means of its communication has existed. The joint town of Dumfries and Maxwell-town, not usually an unhealthy place, has been visited by the cholera both in 1832 and at the close of last year with extreme severity. On the last occasion the deaths were 317 in Dumfries, and 114 in Maxwell-town, being 431 in a population of 14,000. The inhabitants drink the water of the Nith, a river into which the sewers empty themselves, their contents floating afterwards to and fro with the tide. Glasgow, which has been visited so severely with the malady, is supplied, as I understand, with water from the Clyde, by means of an establishment situated a little way from the town, and higher up the stream, and the water is professed to be filtered; but as the Clyde is a tidal river in that part of its course, the contents of the sewers must be washed up the stream, and, whatever care may be taken to get the supply of water when the tide is down, it cannot be altogether free from contamination. In the epidemic of seventeen years ago, the cholera was much more prevalent in the south and east districts of London, which are supplied with water from the Thames and the Lea, where these rivers are much contaminated by the sewers, than in the other parts of the metropolis differently supplied. And this is precisely what has occurred again, as will be shewn further on.
The opinions now made known have been entertained by the author since the latter part of last year, and were mentioned by him to several medical gentlemen in the winter,--amongst others, to Dr. Garrod and Dr. Parkes; but he hesitated to publish them, thinking the evidence in their favour of so scattered and general a nature as not to be likely to make a ready and easy impression. Within the last few days, however, some occurrences have come within his knowledge which seem to offer more direct proof, and have induced him to take the present course.
In Thomas Street, Horsleydown, there are two courts close together, consisting of a number of small houses or cottages, inhabited by poor people. The houses occupy one side of each court or alley--the south side of Trusscott's Court, and north side of the other, which is called Surrey Buildings, being placed back to back, with an intervening space, divided into small back areas, in which are situated the privies of both the courts, communicating with the same drain, and there is an open sewer which passes the further end of both courts. Now, in Surrey Buildings the cholera has committed fearful devastation, whilst in the adjoining court there has been but one fatal case, and another case that ended in recovery. In the former court the slops of dirty water poured down by the inhabitants into a channel in front of the houses got into the well from which they obtained their water, this being the only difference that Mr. Grant, the Assistant-Surveyor for the Commissioners of Sewers, could find between the circumstances of the two courts, as he stated in his report to the Commissioners. The well in question was supplied from the pipes of the South London Water Works, and was covered in on a level with the adjoining ground; and the inhabitants obtained the water by a pump placed over the well. The channel mentioned above commenced close by the pump. Owing to something being out of order, the water for some time past occasionally burst out at the top of the well, and overflowed into the gutter or channel, afterwards flowing back again mixed with the impurities; and crevices were left in the ground or pavement, allowing part of the contents of the gutter to flow at all times into the well, and when it was afterwards emptied a large quantity of black and highly offensive deposit was found in it.
The first case of cholera in this court occurred on July 20th, in a little girl, who had been labouring under diarrhœa for four days. This case ended favourably. On the 21st of July, the next day, an elderly female was attacked with the disease, and was in a state of collapse at ten o'clock the same night. This patient partially recovered, but died of some consecutive affection on August 1. Mr. Vinen, of Tooley Street, who attended these cases, states that the evacuations were passed into the beds, and that the water in which the foul linen would be washed would inevitably be emptied into the channel mentioned above. Mr. Russell, of Thornton Street, Horsleydown, who attended many of the subsequent cases in the court, and who, along with another medical gentlemen, was the first to call the attention of the authorities to the state of the well, says that such water was invariably emptied there, and the people admit the circumstance. About a week after the above two cases commenced, a number of patients were taken ill nearly together: four on Saturday, July 28th, seven or eight on the 29th, and several on the day following. The deaths in the cases that were fatal took place as follows:--One on the 29th, four on the 30th, and one on the 31st July; two on August 1st, and one on August the 2nd, 5th, and 10th respectively, making eleven in all. They occurred in seven out of the fourteen small houses situated in the court.
The two first cases on the 20th and 21st may be considered to represent about the average amount of cases for the neighbourhood, there having been just that number in the adjoining court, about the same time. But in a few days, when the dejections of these patients must have become mixed with the water the people drank, a number of additional cases commenced nearly together. The patients were all women and children, the men living in the court not having been attacked; but there has been no opportunity hitherto of examining into the cause of exemption, as the surviving inhabitants had nearly all left the place when the writer's attention was called to this circumstance.
In Albion Terrace, Wandsworth Road, there has been an extraordinary mortality from cholera, which was the more striking, as there were no other cases at the time in the immediate neighbourhood; the houses opposite to, behind, and in the same line, at each end of those in which the disease prevailed, having been free from it. The row of houses in which the cholera prevailed to an extent probably altogether unprecedented in this country, constituted the genteel suburban dwellings of a number of professional and tradespeople, and are most of them detached a few feet from each other. They are supplied with water on the same plan. In this instance the water got contaminated by the contents of the house-drains and cesspools; the cholera extended to nearly all the houses in which the water was thus tainted, and to no others.
These houses are numbered from 1 to 17 in Albion Terrace, and are supplied with water from a copious spring in the road in front of the terrace, the water of which is conducted by a brick barrel drain between Nos. 7 and 8, to the back of the houses, and then flows right and left to supply tanks in the ground behind each house, the tanks being made of brickwork and cement, covered with a flat stone, and connected with each other by stoneware pipes six inches in diameter. A leaden pipe conveyed water from each tank to a pump situated in the back-kitchen. There is a cesspool behind each house, under the privy, and situated four feet from the water-tank. The ground was opened, and the drains examined under the superintendence of Mr. Grant, the Assistant-Surveyor, behind the houses No. 1 and No. 7. The cesspools at both these places were quite full, and the overflow-drain from that at No. 1 choked up. At this house the respective level of the cesspool and the water-tank were measured, and the top of the overflow-drain from the cesspool was found to be fifteen inches above the top of the tank, and the intervening ground was very wet. The overflow-drain mentioned above had no bottom, or one so soft that it could be penetrated with a stick; and it crossed at right angles above the earthenware pipe of the water-tank, the joints of which were leaky, and allowed the water to escape. Behind No. 7, Mr. Grant found a pipe for bringing surplus water from the tanks, communicating with a drain from the cesspool; and he found a flat brick drain laid over the barrel drain before mentioned, which brings the water from the spring. It appears, from a plan of the property, that this drain, which is continued in a direction [16/17] towards the sewer in Battersea Fields, brings surface-drainage from the road, and receives the drains from the cesspools, the house-drains from the sinks in the back kitchens, and the surplus water, or some of it, from the [water-]tanks. There is every reason to believe that this drain is stopped up, but that has not yet been ascertained; at all events, it was unable to convey the water flowing into it during the storm on July 26th, as it burst near the house No. 8, and inundated the lower premises of that and the adjoining house, No. 9, with fetid water; and it was from this time that the water, which had occasionally been complained of before, was found by most of the people in these seventeen houses to be more or less impure or disagreeable. The water broke out of the drain again at No. 8, and overflowed the kitchens, during a heavy rain on August 2nd. It should be particularly remarked, that the [water-]tanks are placed on the same level, so that pumping from one will draw water from the others, and that any impurity getting into one tank would consequently be imparted to the rest.
The first case of cholera occurred at No. 13, on July 28th (two days after the bursting of the drain), in a lady who had had premonitory symptoms for three or four days. It was fatal in fourteen hours. There was an accumulation of rubbish in the cellar of this house, which was said to be offensive by the person who removed it; but the proprietor of the house denied this. A lady at No. 8 was attacked with choleraic diarrhœa on July 30th: she recovered. On August 1st, a lady, age 81, at No. 6, who had had some diarrhœa eight or ten days before, which had yielded to her own treatment, was attacked with cholera; she died on the 4th with congested brain. Diarrhea commenced on August 1st, in a lady aged 60, at No. 3; collapse took place on the 5th, and death on the 6th. On August 3rd, there were three or four cases in different parts of the row of houses, and two of them terminated fatally on the same day. The attacks were numerous during the following three or four days, and after that time they diminished in number. More than half the inhabitants of the part of the terrace in which the cholera prevailed were attacked with it, and upwards to half the cases were fatal. The deaths occurred as follows; but as some of the patients lingered a few days, and died in the consecutive fever, the deaths are less closely grouped than the seizures. There was one death on July 28th, two on August 3rd, four on the 4th, two on the 6th, two on the 7th, four on the 8th, three on the 9th, one on the 11th, and one on the 13th. These make twenty fatal cases; and there were four or five deaths besides amongst those who were attacked after flying from the place.
The fatal cases were distributed over ten out of the seventeen houses, and Mr. Mimpriss, of Wandsworth Road, who attended many of the cases, and to whose kindness the writer is indebted for several of these particulars, states that cases occurred in the other seven houses, with the exception of one or two that were empty, or nearly so. There were five deaths in the house No. 6, and one of a gentleman the day after he left it, and went to Hampstead Heath. The entire household, consisting of seven individuals, had the cholera, and six of them died.
There are no data for showing how the disease was probably communicated to the first patient, at No. 13, on July 28th; but it was two or three days afterwards, when the evacuations from this patient must have entered the drains, having a communication with the water supplied to all the houses, that other persons were attacked, and in two days more the disease prevailed to an alarming extent.
The water was found to be polluted by the contents of the drains and cesspools to a great extent. That removed by Mr. Grant from the tank behind No 1, had, when first taken out, an odour distinctly stercoraceous. It is less offensive now, at the end of twelve days, than when it was removed. It does not become clear on standing, owing to a kind of fermentation going on in it, which prevents the mud from entirely settling to the bottom of the vessel. After being filtered through paper, it is quite clear, but retains a slight disagreeable taste, and froths on being agitated. On evaporating 1000 grains to dryness, there is a residue of nearly two grains over and above the residue of salts obtained by evaporating water obtained from a pump which is supplied from the same spring. This excess consists, there is no doubt, of soluble organic matters, the exact nature of which has not been determined. In the water-tank behind No. 7, there was a dark-coloured offensive deposit, six to nine inches deep, although the depth of the tank was only two feet. There was also a scum on the surface of the water. Some of the deposit, which was removed, has been undergoing putrefactive fermentation, and giving off sulphuretted hydrogen, ever since, having a tendency to expel the cork from the bottle in which it is kept. It possesses the odour of privy-soil very distinctly. Various substances have been found in it which escape digestion, as the stones and husks of currants and grapes, and portions of the thin epidermis of other fruits and vegetables. Little bits of paper were likewise found. Some of the water removed from this tank continued to ferment till a day or two ago, but is now quite clear and transparent; and although there are some portions of the fibrous structures of vegetables lying at the bottom of the bottle in which it is contained, the water itself has neither taste nor smell, and cannot, by either physical or chemical examination, be distinguished from that of the spring whence it originally proceeded. This circumstance shews, in a remarkable manner, the power of spontaneous putrefaction to free water from all impurities of an animal or a vegetable nature.
Many of the patients attributed their illness to the water: this is here mentioned as shewing that they had drank of it, and at the same time found that it was impure. As explaining how persons might drink of such water before finding out its impurity, it may be stated that the grosser part of the material from drains and cesspools has a tendency, when mixed with water, to settle rapidly to the bottom. The only houses supplied with the same water, after passing the tanks in Albion Terrace, were four in Albion Street; but three of these have been empty for months, and the fourth is inhabited by a gentleman who always suspected the water, and would not drink it. There were two or three persons attacked with cholera amongst those who came to nurse the patients after the water was condemned, and who, consequently, did not drink it; but these person were liable, in waiting on the patient, to get a small portion of the evacuations into the stomach in the way first pointed out; and there might be food in the houses previously prepared with the tainted water. It is not here implied that all the cases in Albion Terrace were communicated by the water, but that far the greater portion of them were; that, in short, it was the circumstance of the cholera evacuations getting into the water which caused the disease to spread so much beyond its ordinary extent.
The mortality in Albion Terrace is attributed by Dr. Milroy, in a published report to the General Board of Health, chiefly to three causes: firstly, to an open sewer in Battersea Fields, which is 400 feet to the north of the terrace, and from which the inhabitants perceived a disagreeable odour when the wind was in certain directions; secondly, to a disagreeable odour from the sinks in the back kitchens of the houses, which was worse after the storm of July 26; and lastly, to the accumulation in the house No. 13 before alluded to. With respect to the open sewer, there are several streets and lines of houses as much exposed to any emanations there might be from it, as those in which the cholera prevailed, and yet they were quite free from the malady, as were also nineteen houses situated between the sewer and Albion Terrace. As regards the bad smells from the sinks in the kitchen, their existence is of such every-day, and almost universal prevalence, that they do not help to explain an irruption of cholera, like that under consideration; indeed, offensive odours were created in the thousands of houses, in London, by the same storm of rain on July 26th; and the two houses in which the offensive smell was greatest, viz. Nos. 8 and 9,--those which were flooded with the contents of the drain,--were less severely visited with cholera than the rest; the inhabitants having only had diarrhœa or mild attacks of cholera. The accumulation in the house No. 13 could not affect the houses at a distance from it. It remains evident, then, that the only special and peculiar cause connected with the great calamity which befel the inhabitants of these houses, was the state of the water, which was followed by the cholera in almost every house to which it extended, whilst all the surrounding houses were quite free from it.
Although there are a great number of pumps, supplied by wells, in this metropolis, yet by far the greater part of the water used for drinking and for culinary purposes is furnished by the various Water Companies. On the south side of the Thames the water works all obtain their supply from that river, at parts where it is much polluted by the sewers; none of them obtaining their water higher up the stream than Vauxhall Bridge,--the position of the South London Water Works. Now as soon as the cholera began to prevail in London, part of the water which had been contained in the evacuations of the patients would begin to enter the mains of the Water Works: whether the materies morbi of cholera,--which, it has been shewn, there is good reason for believing is contained in the evacuations,--would be sent round to the inhabitants, would depend on whether the water were kept in the reservoirs till this materies morbi settled down or was destroyed; or whether it could be separated by the filtration through gravel and sand, which the water is stated to undergo. Notwithstanding this filtration, the water in this part of town is not always quite clear, and sometimes it has an offensive smell when clear. The deaths from cholera in this district, which contains a very little more than a quarter of the population, have been more numerous than in all the other districts put together; as will be seen by the following table, taken from the reports of the Registrar-General. Out of the 7466 deaths in the metropolis, 4001 have occurred on the south side of the Thames, being nearly eight to each thousand of the inhabitants.
That division of London called the East District in the registration reports, is supplied with water entirely by the East London Water Company. In the Cholera of 1832 and 1833 the reservoirs of the company at Old Ford were entirely filled from the river Lea when the water flowed up with the rising tide from the Thames, in the neighbourhood of Blackwall; and the river Lea itself receives some large sewers. The Company have since obtained water from near Lea Bridge, above the reach of the tide; but whether they still supply themselves in part from the river at Old Ford, where their chief works and reservoirs are still situated, and if so, to what parts of their district the water so obtained is sent, cannot be here stated, for want of exact information.
The cholera has prevailed to a considerable extent in the East districts, as will be seen by the Table, though not so much as on the south of the Thames.
The North districts have suffered very little from cholera as yet. St. Pancras and Islington, which comprise a great portion of this division, are supplied with the New River water, which is brought from Hertfordshire. Hackney is supplied by the East London Water Works; Hampstead by sources of its own; and Marylebone, which will again be alluded to, chiefly by the West Middlesex Water Works.
The whole of the Central Districts are likewise supplied from the New River, and this part of the town has suffered much less from cholera, hitherto, than the south and east divisions; although many portions of it are quite on a par with the worst parts on the south of the Thames as regards overcrowding and bad smells.
The West Districts, together with Marylebone, are supplied with Thames water by the West Middlesex, Grand Junction, and Chelsea Water Works. The West Middlesex Company obtain their water above Hammersmith, and the Grand Junction at Brentford; both these places, and especially the latter, are, by the meandering course of the river, several miles above London; and unless, perhaps, at certain parts of the tide, are free from sewage water, except that of certain towns,--as Richmond, Barnes, etc.--in which the cholera has not yet been prevalent. The Chelsea Company, which supply Chelsea, Pimlico, Westminster, and part of Brompton, get their water at Chelsea, only one or two miles above Vauxhall; but they take great pains to filter it carefully. It will perhaps be remarked that the dilution of the cholera poison in the Thames would most likely render it innocuous; but as far as can be judged from analogy, the poison consists probably of organized particles, extremely small no doubt, but not capable of indefinite division, so long as they retain their properties.
It will probably be objected to the views advanced in this paper, that animal poisons, when swallowed, are generally destroyed in the stomach by the process of digestion; and, indeed, it is not improbable that the material which gives rise to cholera is often thus destroyed, and its effects resisted, since the complaint is very often observed to come on when the digestive powers have been weakened by a fit of drunkenness.
It should be observed, that the mode of contracting the malady here indicated does not altogether preclude the possibility of its being transmitted a short distance through the air; for the organic part of the fæces, when dry, might be wafted as a fine dust, in the same way as the spores of cryptogamic plants, or the germs of animalcules, and entering the mouth, might be swallowed. In this manner, open sewers, as their contents are continually becoming dry on the sides, might be means of conveying cholera, independently of their mixing with water used for drinking. Mr. Russell, of Horsleydown, who attended the two first cases of the disease occurring in London last autumn--that of John Harnold, a seaman just arrived from Hamburgh, where the disease was prevailing, and that of a man named Blenkinsopp, who came, after the death of the former, to lodge and sleep in the same room, and had the cholera eight days after him*--states, that the next cases in Horsleydown, which commenced three or four days after wards, were in a situation a little way removed from that of the two preceding, and having no apparent connection with it, except that an open sewer, up which the tide flows, runs past both places, and the sewage from the houses in the first neighbourhood is, when the tide rises, carried past those in the second . (* Some serious mistakes respecting these cases have crept into the documents furnished to Dr. Parkes by the General Board of Health, as subject matter for his inquiry into the bearing of the earliest cases of cholera on the question of contagion; as will be evident from a comparison of the following quotations from Dr. Parkes's paper, with the accompanying statement of the real circumstances:--
"The Elbe steamer left Hamburgh on the 22d September, and arrived in the river [Thames] on the 25th. A seaman, named John Harnold, left the vessel, and went to live at No. 8, New Lane, Gainsford Street, Horsleydown. On the 28th of September he was seized with symptoms of cholera, and died in a few hours. It is stated in a letter to the General Board of Health, from Mr. Russell, who attended the patient, that all the characteristic symptoms of cholera were present. Mr. Bowie, who inquired on behalf of the Board into the particulars of the case, corroborated this statement. This may, then, be considered as an undoubted case of cholera."
"If the disease was imported thus from Hamburgh, it did not spread in Horsleydown. Two days subsequently, indeed, Mr. Russell was sent for to a patient in the same house, who fancied he had cholera; but, on examining into particulars, it turned out that the individual in question had been greatly alarmed at the death of the seaman, and was suffering more from the effects of fear than anything else. He was quite well in a few hours. No other person was taken ill in the house or immediate neighbourhood, although, if the second case had not been inquired into, a vague story of communicated disease might have arisen in the neighbourhood."
Now, the illness and death of John Harnold took place on the 22nd of September, and not on the 28th, and Mr. Russell attended the next case in the same room on September 30th. There were, in this latter case, rice-water evacuations, and, amongst other decided symptoms of cholera, complete suppression of urine from Saturday to Tuesday morning, and the patient vomited incessantly for twenty-four hours after this, and after wards had consecutive fever. Mr. Russell had seen a great deal of cholera in 1832, and had no doubt of this being a genuine case; and he [28/29] has seen a great deal of the disease lately, and still continues of the same conviction.
The mistake in the date alone at which the first case occurred, alters the bearing of all the facts submitted to Dr. Parkes, even should the particulars of all the other cases be correct. The writer accidentally detected the errors pointed out in this note by having to call on Mr. Russell in his inquiries respecting Surrey Buildings.)
These opinions respecting the cause of cholera are brought forward, not as matters of certainty, but as containing a greater amount of probability in their favour than any other, in the present state of our knowledge. Nearly all medical men admit a cholera poison, whatever their opinions may be with respect to contagion; and many of them even speak of the purging as an effort of nature to get rid of the poison: they cannot, then, in either case, suppose that the evacuations are free from it, or that, being swallowed, the stomach should always have the power of destroying it, and preventing its producing its peculiar effects; therefore the views here stated seem to have a fair claim to the consideration of the profession. At all events, the mode of communication of cholera is a question of the most vital importance with respect to its prevention. Who can doubt that the case of John Harnold, the seaman from Hamburgh, mentioned above, was the true cause of the malady in Blenkinsopp, who came, and lodged, and slept, in the only room in all London in which there had been a case of [29/30] true Asiatic cholera for a number of years? And if cholera be communicated in some instances, is there not the strongest probability that it is so in the others--in short, that similar effects depend on similar causes?
The belief in the communication of cholera is a much less dreary one than the reverse; for what is so dismal as the idea of some invisible agent pervading the atmosphere, and spreading over the world? If the writer's opinions be correct, cholera might be checked and kept at bay by simple measures that would not interfere with social or commercial intercourse; and the enemy would be shorn of his chief terrors. It would only be necessary for all persons attending or waiting on the patient to wash their hands carefully and frequently, never omitting to do so before touching food, and for everybody to avoid drinking, or using for culinary purposes, water into which drains and sewers empty themselves; or, if that cannot be accomplished, to have the water filtered and well boiled before it is used. The sanitary measure most required in the metropolis is a supply of water for the south and east districts of it from some source quite removed from the sewers.
It would have been more satisfactory to the author to have given the subject a much more extensive examination, and only to have published his opinions in case he could bring forward such a mass of evidence [30/31] in their support as would have commanded ready and almost universal assent; but being preoccupied with another subject, he could only either leave the inquiry, or bring it forward in its present state, and he has considered it to be his duty to adopt the latter course, and allow his professional brethren to decide what there may be of value in his opinions; and he will be happy to receive any information bearing on the points discussed in his paper.
Frith Street, Soho,
Aug. 29, 1849.
Return to John Snow Publications
Source: Snow, John. London Med. Gazette, vol. 44, Sep.15, 1849, pp. 504-05. [letter to ed.]
48. The cholera at Albion Terrace
Correspondence.
Sir,--If you will allow me to make a few brief remarks on the statements respecting the cholera at Albion Terrace, Wandsworth Road, contained in a letter which you have quoted in one of your leading articles, in the last No., I shall be much obliged, both on account of the great medical importance of the occurrences to which these statements relate, and because they contradict, in some points, the particulars which I collected with great pains and trouble, and which you honoured me by quoting in the review at another page. If the whole of the report by Mr. Grant, the Surveyor, had been published, instead of the very brief and scarcely correct abstract, you would have perceived that his knowledge of the circumstances was of a much more exact and comprehensive nature than that of the "member of a family long resident upon the terrace," who is himself evidently not aware of the careful manner in which the subject has been investigated.
To save space, I will merely give the replies, without copying the letter.
1. The common supply of water to all the houses was contaminated with the contents of the drains and cesspools, and therefore the water could not be unaffected in any of the houses, although it might appear to be so.
2. The inhabitants escaped with their lives out of seven of the seventeen houses, but not without cholera or choleraic diarrhœa as regards several of the seven, and, indeed, I was informed by Mr. Mimpriss, surgeon, who lives opposite, that scarcely a house was unaffected, but one or two that were empty, or nearly so. With respect to the water being used without intermission in some of the houses, it must be remarked that soon after the second disturbance of the water, to be mentioned immediately, the surviving inhabitants began to leave the terrace, and in a short time the houses were all closed.
3. Avoiding the water whilst it was turbid might not prevent the mischief, especially according to the view I take of it.
4. The communication between the drains and the water pipes continued open, and a week after the first bursting of the drain it burst in a second thunderstorm, overflowing again the lower premises of the houses 8 and 9. This was on August 2d. A gardener employed to clear away the debris on both occasions, referred to his book for the dates when I called on him. He was then ill, and said that he was recovering from an attack of cholera, which came on after the second job at the terrace. Between the first bursting of the drains on July 26th, and that on August 2nd, there bad been three cases of cholera, one of which had already terminated fatally, and a case of choleraic diarrhœa. On the morning after the second storm three or four persons were attacked, and the attacks continued numerous for three or four days.
5. The greater part of the attacks did not occur on any one day, and therefore could not be within a few hours of the removal of the rubbish. I have not been able to ascertain the exact day on which the
rubbish was removed, as, not thinking that a material point, I did not inquire at an early period. Dr. Milroy, in his report to the General Board of Health, stated that the removal of it took place on the 30th or
31st July, about which time only one or two attacks took place; but a gentleman, on whom I called to-day, living in the house adjoining that from which it was removed, thinks it was on August 2nd, and the morning
after this there were three or four persons attacked. There are several houses in the Wandsworth Road which remained free from cholera, although they are nearer to No. 13, from which the offensive rubbish was removed, than several of those in which the disease raged so fearfully,--for instance, than Nos. 1 to 4 inclusive in Albion Terrace,--but the regurgitation of the contents of the drains into the water on August 2nd, at a time when these drains contained cholera evacuations, affected the water of all these seventeen houses, and of these exclusively.
I shall not at present make any remarks on the way in which the water might cause the spread of the cholera in this row of houses, but intend shortly to lay before the readers of the Medical Gazette, with your permission, a variety of details, collected from different parts of the country which show the connection between tainted water and the extension of cholera, and also the great freedom from cholera, both now and in 1832, enjoyed by certain large towns--as Birmingham, Bath, and Cheltenham, which have a plentiful supply of water that is totally unmixed with the contents of sewers.--I remain, sir,
Your obedient servant,
John Snow
Frith Street, Soho,
Sept 15, 1849.
This correspondence was followed a week later by the same letter, published again in the London Medical Gazette, perhaps because of its importance, September 21, 1849.
Return to John Snow Publications
Source: Snow, John. London Med. Gazette, vol. 44, 2 November 1849, pp. 745-752, 30 November 1849, pp.
923-929.
49-50. "On the pathology and mode of communication of cholera."
Reasons for considering cholera a local affection of the alimentary canal--proofs of its communicability--difficulties in the way of the ordinary doctrine of contagion. Cholera poison is contained in the evacuations, and communicates the disease by being swallowed: illustrations of this in the houses of the working classes--in mining districts. Cholera communicated by drinking water: cases illustrating this. Difference of elevation in London influences cholera only through the drinking-water. Communication of cholera through the water in York, Exeter, Hull.
Writers on cholera, however much they may have differed in their views concerning the nature of the disease, have generally considered it to be an affection of the whole body, and consequently due to some cause which acts, either on the blood or the nervous system. The following are the reasons which have led me to entertain the opinion that cholera is, in the first instance at least, a local affection of the mucous membrane of the alimentary canal; an opinion which I thought almost peculiar to myself when I was first led to adopt it, but which, as I have since been informed, others were beginning to entertain.
In those diseases in which there is reason to conclude that a morbid poison has entered the blood, there are symptoms of general illness, usually of a febrile character, before any local affection manifests itself; but so far as I have been able to observe or to learn from carefully recorded cases, it is not so in cholera. On the contrary, the disease begins with the affection of the bowels, which often proceeds with so little feeling of general illness, that the patient does not consider himself in danger, or apply for advice till the malady is far advanced. It is true that, in a few cases, there are dizziness and faintness before discharges from the bowels actually take place, but there can be no doubt that these symptoms depend on the exudation from the mucous membrane, which is soon afterwards copiously evacuated. With respect to certain rare cases of cholera without purging, Dr. Watson has remarked in his Lectures, that when the bodies of such patients have been opened, the characteristic fluid was found in the bowels. Another reason for looking on cholera as a local disease is, that the affection of the stomach and bowels is sufficient to explain all the general symptoms. The evacuations, in the cases I have witnessed, have always appeared sufficient to account for the collapse, when the suddenness of the attack is considered, and the circumstance that absorption is probably suspended. The thickened state of the blood arising from the loss of fluid accounts for the symptoms of asphyxia, by the obstruction it must occasion in the pulmonary circulation. The recent analyses of the blood of cholera patients, by Dr. Garrod, afford the strongest confirmation of this view; for he found it to contain a much greater amount of solid materials in proportion to the water, than in health or other diseases. If there has been more purging in some of the less severe cases than in the rapidly fatal ones, it only shows that, in the former, absorption has been still going on, or else that some of the fluids which have been swallowed have passed through the bowels. The drain of fluid into the alimentary canal suspends the urinary secretion, either totally or in great part, and the kidneys become congested from the altered state of the blood: hence any little urine that is secreted is albuminous; and if the kidneys do not soon recover from the congestion, urea accumulates in the blood in those cases in which the patient survives the stage of collapse. Although in a great number of cases the symptoms of cholera manifest themselves suddenly, and are not amenable to any known treatment, yet in other cases the disease commences gradually with diarrhœa, and in this stage there is evidence to show that it can usually be cured by the ordinary remedies for diarrhœa. Now this circumstance is a strong reason for concluding, that the mischief in cholera is at first confined to the mucous membrane; for it is not easy to conceive that chalk, and opium, and catechu, could neutralize or suspend the action of a poison in the blood. [745/746] Indeed, diseases caused by a morbid poison in the blood, such as the eruptive fevers, cannot be cut short, either by local or general means, but run a definite course.
An important part of the pathology of every disease is the knowledge of its cause. To ascertain the cause of cholera, we must consider it not only in individual cases, but also in its more general character as an epidemic. On examining the history of cholera, one feature immediately strikes the inquirer--viz. the evidence of its communication by human intercourse. In its progress from place to place it has nearly always followed the great channels of human intercourse. In spreading along the highways in India, it often spared the villages that were situated at a little distance from the main road, on either side. When a body of troops were attacked with it on their march, it often remained with them through countries having a very different climate and physical character from that in which they contracted the malady; and they often communicated it to towns and villages previously free from it. In extending itself to a fresh island or continent, the cholera has always made its appearance first at a sea-port, and not till ships had arrived from some infected place. Crews of ships approaching a country in which the disease was prevailing, have never been attacked until they have had communication with the shore. The cholera, moreover, in progressing from one place to another, has never travelled faster than the means of human transit, and usually much slower. Such are the general considerations which show that cholera is communicated by human intercourse; and there are besides instances so numerous of persons being attacked with the disease within a day or two after immediate proximity to the sick, that it seems impossible to attribute the circumstance to mere coincidence. On the other hand, there are a number of facts which have been thought to oppose this evidence: numerous persons hold intercourse without becoming affected, and a great number take the disease who have had no apparent connection with other patient. These facts, however, have always been examined with the conviction that cholera, if communicable, must be contagious in the same way that the eruptive fevers are believed to be--viz. by effluvia given off from the patient into the surrounding air, and acting on other persons either directly or through the medium of fomites. But with a fresh pathology of the disease this opposing evidence requires to be reconsidered, and will, in the sequel, be found to afford the strongest confirmation of the communication of the disease.
In the meantime we have arrived at two conclusions--first, that cholera is a local affection of the alimentary canal; and secondly, that it is communicated from one person to another. The induction from these data is that the disease must be caused by something which passes from the mucous membrane of the alimentary canal of one patient to that of the other, which it can only do by being swallowed; and as the disease grows in a community by what it feeds upon, attacking a few people in a town first, and then becoming more prevalent, it is clear that the cholera poison must multiply itself by a kind of growth, changing surrounding materials to its own nature like any other morbid poison; this increase is the case of the materies morbi of cholera taking place in the alimentary canal.
The instances in which minute quantities of the ejections and dejections of cholera patients must be swallowed are sufficiently numerous to account for the spread of the disease; and on examination it is found to spread most where the facilities for this mode of communication are greatest. Nothing has been found to favour the extension of cholera more than want of personal cleanliness, whether arising from habit or scarcity of water, although the circumstance hitherto remained unexplained. The bed linen nearly always becomes wetted by the cholera evacuations, and as these are devoid of the usual colour and odour, the hands of persons waiting on the patient become soiled, and unless these persons are scrupulously cleanly in their habits, and wash their hands upon taking food, they must accidentally swallow some of the excretion, and leave some on the food they handle or prepare, which has to be eaten by the rest of the family, who amongst the working classes often arrive to take their meals in the sick [746/747] room: hence the thousands of instances in which, amongst this class of the population, a case of cholera in one member of the family is followed by other cases; whilst medical men and others, who merely visit the patients, generally escape. The post-mortem inspection of the bodies of cholera patients has hardly ever been followed by the disease that I am aware, this being a duty that is necessarily followed by careful washing of the hands; and it is not the habit of medical men to be taking food on such an occasion. On the other hand, the duties performed about the body, such as laying it out, when done by women of the working class, who make the occasion one of eating and drinking, are often followed by an attack of cholera; and persons who merely attend the funeral, and have no connection with the body, frequently contract the disease; in consequence, apparently, of partaking of food which has been prepared or handled by those having duties about the cholera patient, or
his linen and bedding.
It has been found that the mining population of this country has suffered more from cholera than any other, and there is a reason for this. There are no privies in the coal pits,* (*Dr. D. B. Reid, in Second Report of Commissioners for inquiring into the state of large towns and populous districts. Appendix, part ii, p. 122), and I believe that this is true of other mines: as the workmen stay down the pit about eight hours at a time, they take food down with them, which they eat, of course, with unwashed hands, and as soon as one pitman gets the cholera, there must be great liability of others working in the gloomy subterranean passages to get their hands contaminated, and to acquire the malady; and the crowded state in which they often live affords every opportunity for it to spread to other members of their families. There is also another cause which favours the spread of cholera amongst many of the mining populations, to which I shall have to allude shortly, in treating of the water.
With only the means of communication which we have been considering, the cholera would be constrained to confine itself chiefly to poor and crowded dwellings, and would be continually liable to die out accidentally in a place, for want of the opportunity to reach fresh victims; but there is often a way open for it to extend itself more widely, and that is by the mixture of the cholera evacuations with the water used for drinking and culinary purposes, either by permeating the ground and getting into wells, or by running along channels and sewers in to the rivers.* (*See review in Med. Gaz. present volume, p. 466.)
The part of the metropolis most severely visited by cholera in 1832, was the Borough of Southwark, in which 97 persons in each 10,000 of the population were carried off, being nearly three times the proportion of deaths that occurred in the rest of London. Now the population of Southwark at that time (such of them as did not use pump-water), were supplied by the Southwark Water Works with Thames water obtained at London Bridge, and sent direct to their dwellings without the intervention of any reservoir. The Thames has since become more polluted by the gradual abolition of numbers of cesspools in the metropolis, and the Southwark Water Works have been removed to Battersea, a little further from the sewers. I am endeavouring to compile a full account of the recent epidemic in London, in its relation to the water, but as it is not yet complete I must here be content with citing certain instances of severe visitation, or of exemption from its ravages.
There are two courts in Thomas Street, Horsleydown, exactly resembling each other; the small houses which occupy one side of each court being placed back to back, and the privies for both courts being placed in the intervening back areas, and emptied into the same drain which communicated with an open sewer passing the end of both the courts. In Trusscott's Court, as one of them is called, there was but one death from cholera, whilst in the other, named Surrey Buildings, there were eleven deaths. In this latter court the refuse water from the houses got into the well from which the people obtained their water. The succession of the cases illustrates the mode of communication. There were first two cases in Surrey Buildings, the evacuations of these patients being passed into the bed, as I was in-[474/748]formed by Mr. Vinen, of Tooley Street, who attended them; in a few days after, when the water in which the soiled linen had been washed must have become mixed with that in the well, a number of cases commenced nearly together in all parts of the small court. The instance of Albion Terrace, Wandsworth Road, was a still more striking one of the communication of cholera by means of water. As the account of the occurrence was quoted in a Review in the Medical Gazette,* (*Present vol., p. 468)and some further particulars supplied by me in a note† (†Ibid., p. 504), I need not now relate the particulars, but will briefly state that, owing to a storm of rain and thunder, such a connection was established between the drains and water, that, on a case of cholera occurring in any one of seventeen houses, the evacuations might enter the water supplied to all the others. Such a case did occur, and in a short time the prevalence of cholera was such as I believe had not before been known in this country; whilst at the same time there was but little of the disease at the time, or I believe since, in the surrounding streets and houses. I will take this occasion to remark that we have now an explanation of the reason why the cholera has on some occasions increased very much immediately after a thunder storm, and on other occasions has very much diminished. The cause of this lies in the rain, and not in the thunder. In some places drains containing cholera discharges would be made to overflow into a brook or river, or other source from which water was obtained, whilst in other places drinking-water already contaminated would be nearly altogether washed away, and replaced by a fresh supply.
Dr. Lloyd mentioned some instances of the effects of impure water at the South London Medical Society, on August 30th‡ (‡See Report in Med. Gaz., p. 429). In Silver Street, Rotherhithe, there were eighty cases, and thirty-eight deaths, in the course of a fortnight early in July last, at a time when there was very little cholera in any other part of Rotherhithe. The contents of all the privies in this street ran into a drain which had once had a communication with the Thames; and the people got their supply of water from a well situated very near the end of the drain, with the contents of which the water got contaminated. Dr. Lloyd has informed me that the fœtid water from the drain could be seen dribbling through the side of the well, above the surface of the water. Amongst other sanitary measures recommended by Dr. Lloyd was the filling up of the well; and the cholera ceased in Silver Street as soon as the people gave over using the water. Another instance alluded to by Dr. Lloyd was Charlotte Place, in Rotherhithe, consisting of seven houses, the inhabitants of which, excepting those of one house, obtained their water from a ditch communicating with the Thames, and receiving the contents of the privies of all the seven houses. In these houses there were twenty-five cases of cholera, and fourteen deaths; one of the houses had a pump railed off, to which the inhabitants of the other houses had no access, and there was but one case in that house. The people in Rotherhithe, where the mortality from cholera has been greater than in any other part of the metropolis, are supplied with water to a great extent from certain tidal ditches communicating with the Thames, and receiving besides the refuse of the houses in the neighbourhood; and Dr. Lloyd informs me that a line may be drawn between the places where ditch-water is used, and those supplied from the Water Works, and that the cholera has been many times more prevalent in the first mentioned places; although, in my opinion, the water supplied from the water works is itself not free from suspicion of having conveyed cholera poison, being obtained from the Thames. Rotherhithe is less densely populated than many parts of the metropolis which have been comparatively free from cholera, and those ditches, it should be remembered, are not very offensive to the smell; being only Thames water rendered a little richer in manure; being, in short, probably equal to what Thames water would be if certain of our sanitary advisers could succeed in having the contents of all the cesspools washed into the river. In Bermondsey, the district in which next to Rotherhithe the cholera has been most fatal, the people also have to drink ditch water to a great extent.
The Registrar-General has very ably pointed out the connection between the higher rate of mortality from cholera on the south side of the Thames, and the lower level of the ground; but when this division of the metropolis is examined in detail, and compared with certain other parts of London, it will be found that the relation is not one simply of level, or of the state of the air in connection with it, but that it depends altogether on the water used by the people. Not because the water carries the poison to every individual case, but because it supplies a number of scattered cases which diffuse the disease more generally. The water works supplying the South of London take water from the Thames mostly at places near which the chief sewers run into it. Moreover, the wells in this part of London are very liable to be contaminated by the contents of cesspools. Mr. Quick, engineer of the Southwark waterworks, in his evidence before the Sanitary Commissioners in 1844, said that in the South side of the Thames the wells are often so contaminated owing to the cesspools and the wells being often about the same depth--viz. from eight to twelve feet, whilst on the north of the Thames the wells require to be from thirty to seventy, or eighty feet deep* (*First Report, p. 396). These, together with the water from the ditches mentioned above, are the chief sources of the high mortality on the south of the Thames, and where they are not in operation there has been comparative immunity from the disease. Bethlem Hospital is very copiously supplied with water from an Artesian well on the premises, and I am informed that there have been but two or three cases of cholera out of a population of about seven hundred. Mr. Morton, Surgeon to the Queen's Prison, informs me that, although there has been a good deal of diarrhea there have been but two cases of cholera in that establishment, containing a population, with the officers and attendants, of 300 and upwards, and one of the cases (the only fatal one) occurred in a patient who had been about a week in the prison, had suffered from an attack of cholera just before he entered, and had lost some members of his family by it. Now, the Queen's Prison is supplied with very good water from various wells within the walls. Bethlem Hospital is situated in Lambeth, where one in every eighty-eight of the population have been carried off by cholera; and the Queen's Prison in Southwark, where one in every sixty persons have died of it: and the latter establishment is closely surrounded by houses, in numbers of which the cholera has been very fatal. In another institution in London, situated at the same elevation as those just mentioned, there has been, together with a difference of water, a difference in the relative prevalence and facility of cholera amongst its inmates and the surrounding population, but here it has been against the institution and in favour of those outside: I allude to the Millbank Prison. The cholera showed itself there soon after its appearance in London last autumn; and during the summer of the present year it became very prevalent, and the greater number of the prisoners were sent away. Dr. Baly stated before the coroner that the cases occurred in different parts of the prison, amongst persons having no connection with each other, and that the strongest and most healthy men were often its victims. The water used in the Millbank Prison is obtained from the Thames at the spot, and is filtered, through sand and charcoal and looks very clear. Before these investigations there could be no objection to such water; but it would appear by the result that the filtration was not an effectual safeguard. I cannot help suggesting that the water used here may have had some connection with the dysentery which has been often prevalent in this prison, for dysentery has apparently been kept up in India by water containing human excrements; and the same circumstance was observed in the old barracks at Cork, by Mr. Bell, surgeon of that town* (*Dr. Cheyne on Dysentery, Dublin Hospital Reports, vol. iii).
The greater part of Westminster abounds in nuisances, and is crowded with very poor and destitute people. The average elevation of it is exactly the same as that of St. Saviour's and St. Olave's, Southwark, but the mortality from cholera in Westminister to the end of September has been but [749/750] 69 in the 10,000; whilst in St. Saviour's it has been 162, and in St. Olave's 152 or 179, according as the deaths in St. Thomas's Hospital are left out or included. The greater part of Pimlico and Chelsea have the same elevation as the Borough, but the mortality in them has been less than one-third as great as in the Borough. Westminster, Chelsea, and Pimlico are supplied with Thames water from the Chelsea water-works; but as the same water is supplied to the Court and a great part of the aristocracy, the Company have large settling reservoirs and very expensive filters, by means of which, probably, the greater part of the cholera poison has been got rid of. The registrar's district of Brixton is situated on rising ground, the elevation of which varies from 12 to 140 feet above Trinity high-water mark, giving an average elevation at least equal to that part of London situated on the north of the Thames; and it is inhabited very much by people in comfortable circumstances, occupying wide and open streets, and scattered rows of houses, or even detached villas; yet in looking over the reports, I find eighty-three deaths from cholera since May last. The population in 1841 was 10,175; this would yield 81 deaths in the 10,000, or twice as many as have occurred on the north of the Thames; but the population of Brixton has probably increased since 1841, by the building of new houses, more than in London generally. Still there can be no doubt that the mortality there from cholera has been much higher than in many of the worst parts to the north of the river; and the reason is not far to seek, for the greater part of the Brixton district is supplied by the Lambeth water-works with water obtained from the Thames near the Hungerford Suspension Bridge.
I will now proceed to narrate some circumstances that have occurred in the provinces. The drainage from the cesspools found its way into the well attached to some houses at Locksbrook, near Bath, and the cholera making its appearance there this present autumn became very fatal. The people complained of the water to the gentleman belonging to the property, who lived at Weston, in Bath, and he sent a surveyor, who reported that nothing was the matter. The tenants still complaining, the owner went himself, and on looking at the water and smelling it, he said that he could perceive nothing the matter with it. He was asked if he would taste it, and he drank a glass of it. This occurred on a Wednesday; he went home, was taken ill with the cholera, and died on the Saturday following, there being no cholera in his own neighbourhood at the time.
When the cholera made its appearance at York, about the middle of July last, it was at first chiefly prevalent in some narrow streets near the river, called the Water Lanes. The inhabitants of this spot had been in the habit from time immemorial of fetching their water from the river at a place near which one of the chief sewers of the town empties itself; and recently a public necessity had been built, the contents of which were washed every morning into the river just above the spot at which they got the water. In a short time from twenty to thirty deaths occurred in this locality; but the medical men considering the impure water injurious, the people were supplied from the water-works, with water obtained from the river at a point some distance above the town, and the cholera soon almost ceased in this part of the city, but continued to spread in some other parts. The cholera having thus abated in the Water Lanes, the gratuitous supply or water was cut off, and the people went to the river as before. There were still cases of cholera in the town, and it soon broke out again in this locality, and in the first few days of September eight deaths occurred among the persons who used water obtained direct from the river. The tap for general use was again opened, and the river water interdicted, and the cholera again ceased, and has not recurred. These circumstances were communicated to me by a friend on whose accuracy I can rely, and an extract from his notes on the subject afterwards appeared
in the Yorkshireman Newspaper.
The first cases of cholera in Exeter, in 1832, were three in the same day besides one in St. Thomas's, a suburb of Exeter, in a gentleman just arrived from London, where the disease was prevailing. The other three were a woman and her two children; the former, with one of her children, had [750/751] returned from Plymouth the previous day where she had been nursing a child that had died of the cholera. Within five days from this time, there were seven fresh cases in is many different parts of the town, amongst persons having no intercourse with each other or the first cases. The disease soon became very prevalent, and in three months there were 1,135 cases, and 345 deaths. Exeter is situated on ground which rises from the edge of the river to an elevation of 150 feet. In 1832 the inhabitants were chiefly supplied with river water by water-carriers, who conveyed it in carts and pails. Dr. Shapter, from whose work the above particulars are obtained, has kindly furnished me with information concerning the sewers, and maps of their position. The water-carriers, by whom Exeter was very greatly supplied, obtained their water almost exclusively from certain streams of water, diverted from the river in order to turn watermills; and one of the chief sewers of the town, which receives such sewage as might come from North Street, in which the first cases of cholera occurred, empties itself into the branch from the river which divides into the two mill-streams just mentioned. It must be remarked that the parish of St. Edmund, in which these streams of water were situated, had a lower mortality from cholera than other parts of the town like it densely populated and on low ground near the river. Dr. Shapter attributes this lower rate of mortality, and I believe rightly, to St. Edmund's being freely intersected by running streams of water. The people would probably not drink more of the water than in parts of the town where it was less plentiful, and had to be paid for, but they would have much better opportunities for personal cleanliness: so that whilst they would be exposed to only the same number of scattered cases, they would be less likely to have the malady spreading through families, and by personal intercourse. After the cholera of 1832 measures were taken to afford a better supply of water to Exeter; not, so far as I can find by Dr. Shapter's work, that its impurity was complained of, but because of its scarcity and cost. Water-works were established on the river Exe, two miles above the town, and more than two miles above the influence of the tide. Exeter is now very plentifully supplied with this water, and Dr. Shapter has informed me that this year there have only been about twenty cases of cholera, nearly half of which have occurred in strangers coming into the town, and dying within two or three days after their arrival.
We will now consider the town of Hull, in which, together with other sanitary measures adopted since 1832, there has been a new and more plentiful supply of water, but with a different result to that at Exeter. In 1832 Hull was scantily supplied with water conveyed in pipes from springs at Anlaby, three miles from the town. About five years ago new water-works were established to afford a more plentiful supply. These works are situated on the river Hull, at Stoneferry, two miles and three quarters from the confluence of that river with the Humber. About half the sewage of the town is delivered into the river of the same name, the rest being discharged into the Humber, as appears from information and a map kindly furnished me by Dr. Horner, of Hull, who has been making great efforts to have better water obtained for the town. The tide flows up the river many miles past the water-works, carrying up with it the filth from the sewers. The supply of water is, to be sure, obtained when the tide is down, but as the banks of the river are clothed with sedges in many parts, and its bottom deep with mud, the water can never be free from sewage. Moreover, there are some parts of the river above Stoneferry much deeper than the rest, and where the deeper water is, according to the testimony of boatmen, nearly stagnant; thus allowing the water carried up by the tide to remain and gradually mix with that afterwards flowing down. There are also boats, with families on board, pressing up the river to the extent of 5,000 voyages in the year. The water when taken from the river is allowed to settle in the reservoir for twenty-four hours, and is then said to be filtered before being sent to the town. In 1832 the cholera was confined almost exclusively to the poor, and the deaths amounted to 300.
This year, according to what I have gathered from the weekly reports, they [751/752] have been six times as numerous.
Dr. Horner informs me that they have occurred amongst all classes of the community; that he thinks one in every thirty-three of the population has been carried off although 8,000 or 10,000 are said to have left the town to escape the ravages of the pestilence. All this has happened
notwithstanding that the town is much better drained now than in 1832, and the drains in Hull proper are flushed frequently with water from the Docks.
PART II.
Communication of Cholera through the water at Dumfries--at Newburn-on-the-Tyne--at Bilston--Exemption of Birmingham and other towns from cholera--Propagation of cholera by means of water in India--The materies morbi probably sometimes destroyed by the digestive powers--Proof of communication of cholera derived from the period of its duration--Its decline explained--Measures for preventing the propagation of cholera by means of either food or water.
The former part of this paper concluded with the instances of Exeter and Hull, in both of which towns there had been, amongst other sanitary measures, a new and increased supply of water between 1832 and the present year; and in connection with this change was an immense difference in the prevalence of cholera for the better or the worse, according as the evacuations or the patients were shut out from, or admitted to, the water. In the next town I have to mention the drinking-water has remained the same and the two epidemics have been almost equally fatal.
The inhabitants of Dumfries drink the water of the river Nith, which flows through the town, and into which the sewers discharge their contents, which float afterwards to and fro with the tide. In 1832 there were 418 deaths from cholera out of a population of 11,606, being at the rate of 360 in 10,000, or 1 in every 28 of the inhabitants. The present epidemic visited Dumfries at the close of last year, and carried off 431 persons, or 1 in every 32, out of a population now numbering 14,000; so that the mortality his been excessive on both occasions.
There is no spot in this country in which the cholera was more fatal during the epidemic of 1832 than the village of Newburn, near Newcastle-upon-Tyne. We are informed, in an excellent paper on the subject by Dr. David Craigie,* that exactly one-tenth of the population died. (*Edin. Med. and Sur. Jour., vol. xxxvii) The number of the inhabitants was 550; of these, 320 suffered from the epidemic, either in the form of diarrhœa or the more confirmed disease, and the deaths amounted to 55. Being aware of this mortality, I wrote, about the beginning of the present year, to a friend in Newcastle--Dr Embleton--to make inquiries respecting the water used at Newburn, and he kindly procured me some information from the Rev. John Reed, of Newburn Vicarage, which I received in February, as well as an answer from Mr. Davison, surgeon, of Newburn, to whom I had written in the meantime. I learnt from these communications that the people were supplied with water in 1832, as at present, from three wells, two of which were very little used, and that the water in the third well is derived from the workings of an old coal mine near the village. The water of this well, as I was informed, although generally good when first drawn, becomes putrid after being kept two days. It was considered that the evacuations of the people could not get into any of the wells; but the vicar thought that the water of a little brook which runs past the village, and falls into the Tyne immediately afterwards, might find its way into that well which is chiefly resorted to. Putrefaction, on being kept a day or two, is so much the character of water containing animal matter, that after receiving confirmation of my views respecting the communication of cholera by water from many other places, I recently wrote to Mr. Davison again on the subject, and he has kindly taken a great deal of trouble to investigate the matter further. He informs me that the brook is principally formed by water which is constantly pumped from coal pits in the neighbourhood. About half a mile before reaching Newburn it receives the refuse of a small village, and between that village and Newburn it runs through a privy used by the workmen of a steel factory. In Newburn this brook receives the contents of the open drains or gutters from the houses. The drain which conveys water from a coal mine or drift not worked for a great number of years, to the well mentioned above, passes underneath the brook at one part of its course, and from that point runs alongside of the brook to the well, a distance of about 300 yards. Mr. Davison says that it is disputed whether there is any communication between the drain and the brook, but that it is highly probable that there may be, and that an occurrence which took place a few months ago seems to prove that there is. Some gas-water from the steel manufactory mentioned above got by accident into the brook, and some of the people affirm that the water in the well was strongly impregnated with it.
The first case of cholera in Newburn was that of a young man living close to the brook, about 100 yards above the place at which it passes the well. He was taken ill on the 29th December, 1831, and died, in the stage of consecutive fever, on Jan. 4th, 1832. There were some cases of diarrhœa in the village, but no new cases of cholera till the night of January the 9th, during which night and the following morning thirteen persons were taken ill. During the night of the 12th four persons were attacked; by the 15th there were fourteen new cases, and on this day the late vicar died--the Rev. John Edmonston. By the next day at noon there were it least fifty new cases. A few days after this the disease began to subside, and by the 2d of February had almost disappeared. As several days elapsed between the first case of cholera and the great outbreak, it is probable that the water in which the soiled linen must have been washed, and which would necessarily run into the brook, was the means of communicating the disease to the thirteen persons taken ill on the night between the 9th and 10th of January; unless, indeed, the intermediate cases of diarrhœa could transmit the disease. There have been a few cases of cholera at Newburn the present year, and five deaths, but I have not yet ascertained whether any of them occurred in houses the gutters from which enter the brook above the well; if so, probably some accidental circumstance has intervened to prevent a catastrophe like that which took place in the former epidemic.
The state of the water is often a means of the spread of cholera in mining districts, in addition to the more constant cause pointed out in the former part of this paper. In some places the mines divert the springs, and cause a great scarcity of water, thus limiting the means of personal cleanliness; in other places the people have to use water pumped out of the pits, which of course is liable to be contaminated by the fæces of the miners: this is the case to some extent in the neighbourhood of Bilston, in Staffordshire, as I learn from Dr. Ogier Ward, and also from the Health of Towns Report.* (*Appendix. Part 1, p. 35.)(1) In other districts, again, the ground is so saturated with the refuse of a large population congregated in spots which have neither sewers nor drainage of any kind, and often not even privies, that the impurities get into the wells. This is the state of Merthyr Tydvil, as we are informed by Sir H. T. de la Beche.* (*Ibid., p. 145.)
When the cholera was at Kendal in 1832, the only place in which it was particularly prevalent was a spot called Robinson's Yard, in which there were 20 cases and 6 deaths, out of a population of 96. "From the dunghill and privies" in this yard, "there is every reason to believe that moisture percolated the earth and vitiated the water in the well, as they were more elevated, and consequently the moisture, except by evaporation, could escape in no other direction. The water, moreover, seemed impure, and it was nauseous to the taste."‡ (‡Dr. Proudfoot on the Epidemic Cholera of Kendal, Edin. Med. and Surg. Journ., vol. xxxix, p. 79)
In a court, also, in Windsor, in which the cholera was lately prevailing, it was found that the contents of the drains had got into the well from which the people obtained their water.
There are several large and populous towns which nearly altogether escaped the cholera in 1832, and have had a like exemption from the epidemic that is now subsiding. There have been a few cases in these towns, it is true, and this makes the evidence to be derived from them more instructive; for as these cases were chiefly those of persons newly arrived from places where the disease was prevailing, and of a few individuals who were in close proximity with them after their arrival and illness, we learn that though the cholera was imported to these places and capable of affecting others, yet some means of communication necessary for its diffusion was wanting, or failed to operate. We shall find that in all these towns there was no connection between the sewers and drinking water by which the cholera could be propagated. Birmingham being a very large town, its freedom from cholera has attracted a great deal of attention, and not a few attempts have been made to solve what was thought to be a singularity, though, as we shall find, it is not really so. Birmingham possesses an advantage in point of salubrity in its elevated position, but Walsall, in the neighbourhood, which is as much elevated above the level of the sea, suffered rather severely from cholera both recently and in 1832; and Dowlais, in South Wales, at twice the elevation, was severely visited with cholera during the epidemic of 17 years ago. Birmingham is drained into the River Rea and its tributaries. "The state of the river Rea, which may be regarded as the cloaca or main sewer of the town, is very bad. The stream is sluggish, and the quantity of water which it supplies is not sufficient to dilute and wash away the refuse which it receives in its passage through the town. In hot weather it is consequently often very offensive, and in some situations it is at these seasons covered with a thick scum of decomposing matters."* (*Local Reports on the Sanitary Condition of the Labouring Population of England. 8vo. 1842, p. 194.) From this quotation it appears that if effluvia from sewers caused the prevalence of cholera, Birmingham ought not to have escaped. The state of the river may, indeed, have since been altered, but the description would, at all events, apply to 1832. There is one good property about the river which has escaped the observation of the reporters--viz., that the water is rendered too impure for any one to think of drinking it. The inhabitants are supplied with water from springs and wells, and by water-works, from the river Taine, which is quite uncontaminated by the sewers. In Birmingham, consequently, there is no opportunity for the communication of cholera through the water, and the activity of the local Board of Health, in paying attention to every case amongst the poor, has no doubt been the means of preventing the spread of the disease from one individual to another by contamination of the hands and the food.
Bath has enjoyed an almost total exemption from cholera both recently and in 1832, although Bristol has on both occasions suffered rather severely, and this year the epidemic has prevailed in some villages still nearer than Bristol. Bath is supplied with water conveyed in pipes from the hills surrounding the town, whilst the sewers empty themselves into the river Avon, from which but a very few of the poor people ever obtain water. Cheltenham has enjoyed a like immunity from cholera, with Bath, and the drinking-water there is quite free from connection with the sewers.
The above-mentioned three towns possess some physical advantages, in addition to the purity of the water, over some of the places in which cholera has been prevalent; but such is not the state of Leicester. It is situated in a low elevation, and entire quarters of the town are liable, after heavy rains, to be covered with offensive water from the overflowing of the open sewers and badly constructed drains; and it contains a large population of underfed operatives; yet there has been scarcely any cholera there either in 1832 or the present year. Leicester is supplied with water from springs and pumps, and partly by spring water conveyed in pipes; and the river which flows through the town and receives the sewage, is so much altered by the refuse of dye works, that the water is quite undrinkable.
Preston and Oldham, in Lancashire, are supplied with water from surface drainage on the neighbouring hills, and there has been scarcely any cholera at either of these places. The greater part of the town of Paisley is supplied in a similar way; and I am informed that the cases of cholera which have occurred there in the recent epidemic [925/926] were confined to a quarter of the town to which this supply of water does not extend. Nottingham is supplied with filtered water obtained from the river Trent, some distance above the town. In 1832 this supply did not extend to all the inhabitants, and the cholera was somewhat prevalent amongst the poor, of whom it carried off 289; the population of the town being 53,000. Since that time the water has been extended copiously to all the inhabitants, and there have been but six deaths from the epidemic in the present year. The local Sanitary Committee place the supply of water amongst the chief causes of this immunity from cholera,* and I believe justly. (*See Med. Gaz., p. 672.)
However injurious impure water must be to the health, there is no reason to suppose that it can assist in the spreading of cholera unless it contain the excretions of the patients. Stafford is an illustration of this. In that town, as I learn through the kindness of Dr. Harland, there is not a single sewer, and the liquid refuse from the houses runs down the channels on each side of the streets. It is common at the poorer houses to have holes dug in the ground to allow the waste and refuse water to run into. The town is built on a bed of sand, and water is everywhere found at 8 or 10 feet below the surface, and the whole of the inhabitants have pumps convenient to their dwellings. Dr. Harland, from whom I have these particulars, says he has no doubt that in many cases the refuse liquid must percolate through the sand and get into the pump water; and he has known some instances in which the filthy surface water was allowed to get into the wells. There has been scarcely a case of cholera at Stafford at any time, although the disease has been very prevalent it Bilston, and many other places in Staffordshire, both recently and seventeen years ago. As almost every house has its own well, it is evident that the water does not afford the means of disseminating the cholera in Stafford; but if the disease had been introduced to any extent by other means, the pollution of the wells would no doubt have rendered it more prevalent amongst the limited number of people using the water of such wells.
There are several towns in which the cholera has prevailed to a considerable extent, although the water cannot be blamed, so far as I have been able to learn. But under those circumstances it appears that the malady has been confined almost exclusively to the poor, and has spread chiefly by personal communication. So far as my inquiries have extended respecting the more considerable provincial towns, the results of them has been as follows:--In those towns supplied with water from a river where it contains the sewage of the town, the disease on making its appearance has become very prevalent. All those towns that have enjoyed a comparative immunity from cholera are supplied with water that is uncontaminated; and lastly, the cholera has prevailed to a considerable extent in some towns in which the water can have had no share in the extension of it. The profession may expect to receive a considerable amount of information on this subject shortly, from the replies that will be made to the questions lately issued by the cholera Committee of the College of Physicians.
As we are never informed in works on cholera what water the people drink, I have scarcely been able to collect any information on this point, respecting foreign countries. There are, however, one or two circumstances that I may mention. In 1831, when the cholera had extended itself across Poland, the Hungarians placed a strong cordon of military posts to guard all the passes and defiles of the Carpathian mountains. The epidemic, however, soon showed itself on the south-west side of the chain of mountains; it first appeared in the town of Eperies, situated on one of the streams issuing from the Carpathian mountains, and two days afterwards it appeared at Tockay, a town situated about 70 miles farther south at the junction of this stream, named the Bodrod, with the Theiss.* (*Dr. Craigie in Edin. Med. and Surg. Journ., Supplement, Feb. 1832, p. 150.)
Dr. Parkes informs us in his valuable work on cholera, that in the epidemic at Moulmein, in 1842-3, this disease was confined for many months almost entirely to the houses situated on or over the river; and that "one side of the main street runs close to the river, and the great majority of cases occurred on this side; comparatively few on the other." Dr. Parkes has informed me that he has no doubt that the people living near the river drank the water obtained from it; and the river of course received the refuse of the houses near to it. The circumstances detailed in the following passage from the same page (161) of his work, seem to illustrate very well the communication of cholera through the drinking-water, and are at all events better explained by this view of their cause than any other. "The only Europeans attacked at the commencement of the epidemic were the sailors belonging to the ships in the river: the ships nearest the shore suffered most. Thus nine cases occurred on board H. M. brig Britomarte, lying close in shore; she was moved about a mile away, into the centre of the river, and no more cases occurred. Three cases occurred on board H. M. brig Syren, also lying in shore: she was also moved into the centre of the river, and the cholera immediately ceased. The 63d regiment sailed in September and October, 1842, for Madras. One transport being accidentally detained three days in the river, had fourteen cases of cholera during the voyage; the other transports, four in number, got to sea at once, and had no cholera. A few cases occurred during this time among the Europeans on shore, but these consisted only of those who lived close to the river."
On some occasions in India the cholera has increased in prevalence with such rapidity that it has been thought that contagion would not account for the immense number of new cases: if, however, any of the discharges from the patients accidentally found admission to a limited source of water, we can perceive how that circumstance might account for these sudden outbreaks of the malady, in a warm climate where the drinking of water must be frequent and universal. Whether they have been really due to this cause can only be determined by persons resident in the country.
Many medical men to whom the above circumstances respecting the water have been mentioned, admit the influence of the water, without admitting the special effect of the new element introduced into it--viz., the cholera evacuations in communicating, the disease. They look upon the bad water as only a predisposing cause, making the disease more prevalent amongst those who use it--a view which, in a hygienic sense, is calculated to be to some extent as useful as the admission of what I believe to be the real truth, but which, I think, will be found to be untenable, when the circumstances are closely examined. If the bad water merely predisposed persons to be acted on by some occult cause of cholera to which it is supposed that all are exposed, those using such water ought to become more subject to the disease from the time it enters a town or neighbourhood; instead of which it has been shown in many of the above instances that no particular effect was observed amongst those using the water, until by the occurrence of a case or two of cholera, the evacuations entered the water, when, after a short period of incubation, there were several persons attacked nearly together.
The above evidence of the communication of cholera through drinking-water, confirms the view of the disease being propagated by the swallowing of the materies morbi in the cases resulting from personal intercourse; for if the evacuations can produce the disease when largely diluted, à fortiori must they be capable of causing it when undiluted.
The only circumstance of which I am aware that offers any material opposition to the views on the communication of cholera here explained, is that two or three members of a medical commission in Berlin, in 1831, are related to have swallowed a portion of the cholera evacuations experimentally. The reply that must be made to this is that the stomach has most likely the power of sometimes destroying the poison. There are many reasons for concluding that this is the case. Persons are more liable to the disease in proportion as they advance in age, as is shown by comparing the attacks at different ages with the numbers living of those ages,* and as people advance in life the powers of digestion diminish.(*See Dr. Budd's Lecture, Med. Times, Oct. 20, p. 315.) Whatever has a tendency to produce indigestion, increases the liability to an attack; as fear, anxiety and excesses in eating or drinking. To that part of the subject which refers to the communication of cholera through the water of a river, two objections naturally arise--1st, that the large dilution might be expected to render the poison innocuous; and 2d, that the whole, or nearly so, of the people using the water ought to be affected by it. One answer applies to both the objections: it is, that a poison capable of multiplying in the body must, one would conclude, be organized, and therefore consist of particles, however minute, any one of which happening to reach its suitable habitation without being destroyed, might induce the diseases. Or if the poison be really a chemical compound, capable of complete solution without losing its properties, it might yet be imbibed by minute cells, such as mucous globules or epithelial cells,* and be thus conveyed without being much diluted.(*I am indebted for the idea of epithelium cells conveying the poison, to Dr. Lankester, who indeed thought that I had suggested it.)
It has been asked how these views explain the cessation or decline of the disease; and whilst it must be at once admitted that we cannot actually tell why the cholera begins to decline in a place just when it does, it will appear on sufficient examination that the period of prevalence and declension of the malady are such as afford strong evidence of its communication--evidence even of this being its sole cause. The duration of cholera in a place is usually in a direct proportion to the number of the population. The disease remains but two or three weeks in a village, two or three months in a good-sized town, but in a great metropolis it often remains a whole year or longer. I find from an analysis of the valuable table of Dr. Wm. Merriman, of the cholera in England in 1832,* that 52 places are enumerated in which the disease continued less than 50 days, and that the average population of these places is 6,624. 43 places are likewise down in which the cholera lasted 50 days, but less than 100; the average population of these is 12,624. And there are, without including London, 33 places in which the epidemic continued 100 days and upwards, the average population of which 38,123; or if London be included, 34 places, with an average of 78,823.(*Trans. of Roy. Med. and Chir. Soc., 1844. The following short table will show these figures in a more convenient form:--
This difference in the duration of cholera points clearly to its propagation from patient to patient. If each case were not connected with a previous one, but depended on some unknown atmospheric or telluric state, why should not the twenty cases that happen in a village be distributed over as long a period as the twenty hundred cases which occur in a large town? The views propounded in this paper offer a more ready explanation of the decline of the disease for want of fresh victims, than the usual theory of contagion or infection; for all the members of the community are not liable to be reached by a poison which must be swallowed, as they would be by one in the form of an effluvium.
The recognized physical conditions of the season do undoubtedly influence cholera. Although it can flourish in every temperature, warm weather is usually most congenial to its progress. In September last the number of cases began to decrease both in London and many parts of the provinces immediately after a considerable diminution in the temperature of the weather. This circumstance,
however, is quite compatible with almost every theory of the cause of cholera. It certainly does not oppose the view of the communication of the disease; for whilst
temperature modifies the habits as well as the constitution of man, it might also be expected materially to influence the cholera poison, when it has to remain any time out of the body between quitting one patient and entering another, for the lower forms of organisms to which the special animal poisons bear a marked analogy, are greatly influenced by heat and cold.
The fact of cholera having spread from India over the greater part of the world, and then having retired within its former bounds to extend again after a number of years, is thought by many to have no kind of analogy amongst the more familiar diseases; but it is only a more marked instance of what occurs constantly on a smaller scale, [928/929] in all diseases in which each case owes its origin to a previous one. It is only in a great metropolis that the eruptive fevers are all constantly present; in a village or small town they each disappear, and remain absent for a longer or shorter period either till they be re-introduced from some distant place, or by poison accidentally preserved. Small islands often remain free from some of these diseases for very long periods at a time.
Assuming the views here entertained to be correct, it is not to be expected that we should be able to trace the communication of every case of cholera. The very nature of the mode of propagation of disease above explained must render it obscure and difficult of detection. And the difficulty is probably increased by the poison being conveyed by persons in whom the disease proceeds no further than diarrhœa. The communication of intestinal worms from one patient to another has never been detected, and yet we are obliged to conclude that their minute ova are swallowed, unless we not only adopt the hypothesis of spontaneous generation, but apply it to creatures much higher in the scale of development than do the usual advocates of the doctrine. If there really be such a disease as Asiatic cholera, distinct from the ordinary English cholera which prevails in autumn, with which it is confounded by the Registrar-General, who says that the deaths from cholera are now approaching the average,--a disease imported from Hamburgh after being absent fifteen years, and evidently spreading by communication in very numerous instances; we ought not to conclude that part of the cases must depend on some other occult cause, but rather, first to examine the one sufficient cause we have found, to ascertain whether it will not explain more and more of the facts the further they are inquired into; and to search whether the localities which are favourable to cholera do not promote it through physical conditions which favour its communication.
In concluding this paper it is necessary to point out the measures which, according to the opinions and evidence above detailed, might be expected to prevent the communication, and thus stay the ravages of cholera. They are fortunately of a kind that would not interfere with commercial intercourse, and which medical men would probably be willing to make trial of, whether they do or do not entirely concur in the absolute necessity of them. The most scrupulous attention to cleanliness should be inculcated on those waiting on the sick who ought especially to be careful to wash their hands before touching food. When cholera shews itself in a family having but one room, the patient should either be removed, or the other members of the family, except those required as nurses, should be provided with an asylum elsewhere, especially for cooking and eating their meals. As the evacuations might fly about as a fine dust whenever linen should be disturbed on which they had been allowed to become dry, it is desirable that the soiled linen and blankets should be immersed in water as soon as removed, and afterwards exposed to a boiling heat. The fruit that is hawked about the streets is kept at night in the rooms (and generally under the bed, if there be a bedstead) in which a crowd of people sleep, and in those courts and alleys into which contagious diseases are often first introduced by vagrants: hence people should be dissuaded from buying such fruit. When the cholera makes its appearance in a mining district it would be advisable that the men should work during two "shifts" in the twenty-four hours, of four hours each, instead of one "shift" of eight hours; and should be dissuaded from taking food to their work, and recommended to wash themselves on going home, as I believe they usually do. And, lastly, whilst cholera remains in the country, people should avoid using water which receives the contents of drains or sewers, or the refuse of persons navigating the water. Since anything touched by the hands may enter the mouth, it would be desirable to avoid even washing with such water; and all events, when no other water can be obtained, so much of it as is used for drinking and culinary purposes should be filtered and well-boiled.
I take the opportunity of expressing the obligation I am under to several medical gentlemen, to some of whom I was previously unknown, for the trouble they have kindly taken in answering my enquiries.
1. Since the above was written I have received, through the Rev. J. Win. Owen, a note from Mr. Wm. M. Hancox, surgeon of Bilston, from which I likewise learn that the cholera first made its appearance there this year in a street parallel with the course of a brook which receives the refuse of the whole town; and that "in a small square of buildings consisting of about ten houses, ten persons died of the disease. Most of the inhabitants of this range of houses were in the habit of using water that filtered itself into wells from this stream."
Return to John Snow Publications
Source: Snow, John. London Med. Gazette 45, 26 February 1850, p. 327, [Letter to Ed.].
51. "The alleged employment of chloroform by thieves."
By John Snow, M.D.
In two recent cases of robbery it has been asserted that chloroform was used to render the victims insensible; and although no real evidence has appeared of such having been the fact, yet the statement has gained great publicity through the newspapers, and the sentences on the prisoners have apparently been rendered more severe by the allegation.
It can readily be shown that if thieves and prostitutes were to resort to the use of chloroform in the public streets, in the manner alleged, the attempt would only lead to their instant detection on the spot. The sensation of pungency in the nostrils and throat that is cause by this agent, when its vapour is in sufficient quantity to produce any effect on the sensorium, is so strong and peculiar that no person can take a single inspiration without being aware that he is inhaling something very unusual. Chloroform, in fact, can never be administered without the consent of the party taking it, unless by main force, which has to be used in the case of children who are not old enough to be reasoned into taking it. If a child be asleep when the process of inhalation is commenced, it nearly always awakes before being made insensible, however gently the vapour may be insinuated. As breathing is perfectly under the control of the will, a person would, on finding such a strange attempt being made on him in the public street, instantly hold his breath, and use all his powers of resistance to repel the assault. And supposing the handkerchief, which is the alleged weapon, were held forcibly over his mouth and nostrils, in spite of his efforts, yet he would be able to struggle as long, whilst holding his own breath, as if another person were trying to prevent his breathing by the method called Burking. When it is recollected that a race of 150 yards can be run in one breath, these struggles, it will be perceived, would last long enough to attract a crowd.
It is not difficult to understand how the report of the above use of chloroform first gained currency. The first accounts of the use of this agent in surgery and midwifery which appeared in all the newspapers contained a description of its fruity odour and its administration on a handkerchief, but nothing was said of its pungency. Hence many persons, as I had experience, entertained the opinion that it might be used for effecting robberies. By and by, as it was reported, a person who had fallen down in the street thought, on coming to himself, that he recollected something of a handkerchief being applied to his face, and the insensibility from which he had just recovered was attributed to chloroform. It was most likely, if this was anything more than the ingenious invention of the reporter, that the individual in question had taken a fit. The paragraph, however, was a very suitable one for quotation: and the idea having gained general credence, it is probable that we shall often hear of it, as prosecutors who have to account for being in disreputable places and company, instead of the usual excuse of having been dining out, will try to remember something of a handkerchief.
I do not wish to apply this explanation to the case tried last week at the Old Bailey, and I cannot explain how the prosecutor got to the room of the prisoners, but I wish to state very distinctly my conviction that it was not by means of chloroform, and that, if anything was administered on a handkerchief in Whitechapel, it must have been some agent unknown to medical men, and which, if the police could discover it, would probably be of great service to humanity in the hands of legitimate practitioners. In the case tried on Saturday at the Surrey adjourned sessions it is given in evidence that the prisoner suddenly passed a handkerchief across a man's face in the street: they afterwards went into a public-house, and were seen there by a policeman drinking together. The man after this became insensible, and was robbed by the prisoner. The insensibility is attributed to chloroform on the handkerchief, which was suddenly passed across the man's face before he went into the public-house. This every one at all acquainted with the effects of that agent will perceive to be impossible.
Frith Street, Soho,
Feb. 11th, 1850.
Return to John Snow Publications
Source: Snow, John. London Med. Gazette45, 12 April 1850, pp. 622-27 (part 13).
52. "On narcotism by the inhalation of
vapors"
By John Snow, M.D.
[Part 13]
Action of Alcohol compared with that of Chloroform and Ether.
Experiments on frogs with alcohol--On fishes, with alcohol, chloroform, and ether--Quantity of alcohol necessary to cause drunkenness--To cause death. Anæsthetic effects of alcohol--Liebig's views of the action of alcohol--their application to ether and chloroform--Objections to these views.
I feel that I ought to apologise to the readers of the Medical Gazette for the great length of time that has been allowed to elapse before the completion of these papers. The delay has not arisen from any want of anxiety on my part to bring the subject to a conclusion, but from finding, as I proceeded with it, that it was desirable to repeat many experiments and institute fresh ones,
the performance of which occupied a great deal of time.
In order to enter on the investigation of the modus operandi of ether an chloroform with every advantage, it is desirable to ascertain whether or not alcohol,
which, in its chemical constitution and general physiological properties, considerably resembles these medicines, is identical with them in its action. It was previously stated* that alcohol, pyroxilic spirit, and acetone, which are miscible with water in all proportions, confirm the general rule then laid down, that the power of volatile narcotic substances of the
class we are considering is in the inverse ratio of their solubility, as a large quantity of the above three liquids requires to be taken to produce narcotism. (*Vol. xliii. p. 333.) It afterwards occurred to me that experiments might be instituted to ascertain whether alcohol and the other two liquids obey exactly the law which we found to apply to chloroform, ether, and a number of other bodies. Experiments to determine this point could not easily be made on animals that breathe air exclusively, on account of the length of time that the vapour would continue to be absorbed; but, by employing frogs and fishes, the end could be attained. In the experiments previously related, it was found that the second degree of narcotism was caused when the serum of the blood contained about a fifty-sixth part as much of the chloroform, ether, or other substance examined, as it would hold in solution. Now, if the rule apply to alcohol, the second degree of narcotism ought to be induced when the amount of spirit is equal to one fifty-sixth of the volume of the serum.
The following are some of the experiments undertaken to determine this point.
Exp. 47.--A frog was placed in a shallow glass jar, capable of holding a pint. Seven ounces of water, mixed with a fluid drachm and a quarter of rectified spirit of wine, were put into the jar. The spirit consisted of 80 per cent absolute alcohol, of which it consequently contained one drachm; and, as there are fifty-six drachms in seven ounces, the water contained one part of alcohol in fifty-six. It was the early part of March; and the frog, although quite sensible, was not very lively. When enclosed in the jar, it sat, with the head above the water, breathing the air at the rate of ninety respirations in the minute. As the jar was covered by a plate of glass, the air it contained would soon become charged with vapour of alcohol to the same relative extent as the water; that is to say, it would contain 1-56th part as much as if saturated at the same temperature, and the tendency of the absorption, by both the lungs and skin of the frog, would be to establish an equilibrium between the quantity of alcohol in the fluids of its body and that in the surrounding [622/623] water, when the blood of the frog would consist of about 1-56th part spirits. Two hours after the commencement of the experiment, the strength of the frog appeared to be diminished, and it had a difficulty in keeping its nostrils above the water. It was breathing irregularly, and much less frequently than before. At the end of four hours its head was under the surface, and it was not breathing. Being taken out for a minute or two, it moved its head and limbs feebly, but apparently in a voluntary manner, but did not attempt to breathe. It was replaced in the jar, and left for the night, with its head beneath the surface, the jar being covered as before. The next morning, twelve and a half hours from the beginning of the experiment, the frog was found with its nostrils slightly raised above the surface of the spirit and water, and breathing gently and slowly. Being taken out, it was found to flinch slightly on the skin being pinched, and was able to crawl slowly, chiefly by the use of the anterior extremities. It recovered perfectly in the course of the day. The temperature of the room during this experiment was 50 Fahr.
Exp. 48. Another frog was placed in the same jar, with seven ounces of water containing two and a half fluid drachms of the same spirit, the strength being consequently one part of alcohol in twenty-eight parts. In about an hour and a half the frog seemed feeble, and had difficulty in keeping its nostrils above the surface. At the end of two hours, its head had sunk beneath the surface, but the respiratory movements were going on, though feebly, and it seemed to be swallowing the liquid. At the end of three hours the lower jaw had fallen, and the mouth was open, but there were slight respiratory movements of the hyoid bones. There were feeble muscular twitches (subsultus tendinum) observed occasionally. A support was at this time placed under the anterior extremities of the frog, to keep its head above the surface of the water. It was found to be totally insensible to pinching. Its mouth continued open, and the feeble respiratory movements went on. At the end of five hours it was breathing very gently, and very slight twitchings of the toes could be observed occasionally. Seven hours and a quarter from the commencement of the experiment, the respiration had ceased. The frog was taken out, and showed no signs of life at first; but, on closely observing it, slight quivering movements of the toes, and of different parts of the muscles just beneath the skin, could be seen. It was exposed to the air in a shallow dish containing a very little fresh water. In two hours after its removal, feeble respiratory movements could be occasionally observed. The breathing gradually became quite re-established, and seven hours after its removal it had recovered both sensibility and voluntary motion. The next day it seemed pretty well, and had resumed its colour, having been rendered nearly black whilst narcotized. The other frog also became much darker in colour, whilst under the influence of the spirit, in the previous experiment.
In the former of the above experiments the frog appeared to be in the second degree of narcotism, sensibility and voluntary power being impaired, but not abolished. In the last experiment the narcotism reached, and apparently rather exceeded, the fourth degree. The effect produced was nearly the same as that caused by one twenty-sixth part as much chloroform as the blood would dissolve, in one of the frogs, the subject of Experiment 15, formerly related; and rather more than the effect produced by one thirty-second part as much ether as the blood would dissolve, in a frog used in Exp. 28.
Exp. 49. The frog employed in Exp. 47, being in good health, was, four days afterwards, placed in the same jar with nine ounces of water, containing five fluid drachms of rectified spirit of 80 per cent, equivalent to half an ounce of absolute alcohol; the proportion of alcohol being, consequently, one in eighteen of the mixture. At first the frog made some attempts to get out. At the end of seven minutes it withdrew its head voluntarily beneath the surface and ceased to breathe; but two or three minutes afterwards it raised it again above the surface, and breathed the air. Twenty minutes from the commencement, it appeared to have a difficulty in keeping its nostrils above the surface, and now and then made an abortive attempt to leap up. The eyelids were half closed, and the cornea looked dim. At the end of half an hour it was lying on its belly without any sign of life. A support was placed under it to keep its head above the surface, and feeble respiratory movements recommenced. Three quarters of an hour from the beginning of the experiment, the respiration had entirely ceased, and no external sign of life remained. It was left an hour longer in the jar, and was taken out after being exposed to the spirit and water, and the vapour given off from it, for an hour and three quarters. No pulsation of the heart could be observed externally, but on removing a portion of the integuments and sternum with the scissors, the heart was found to be pulsating feebly. The frog was placed again in the spirit and water, being laid on its back, so that the heart could be observed. It was noticed to continue pulsating feebly for half an hour. Being left for two hours, it was found at the end of that time that the action of the heart had entirely ceased. As only one or two drops of blood were lost in exposing the heart, and as frogs at the temperature at which this experiment was performed (52? Fah.) can live almost altogether without the pulmonary respiration, it is probable that the action of the heart was arrested by the narcotic effect of the alcohol; and it was found in experiment 42 and 43, formerly related, that one eighteenth part as much of the vapour of chloroform as the blood would dissolve, had
the effect of arresting the action of the heart in frogs.
Exp. 50. Two fluid drachms and a half of rectified spirit, equivalent to a quarter of a fluid ounce of absolute alcohol, were mixed with sufficient
water to make up fourteen ounces, which, consequently, contained one part of alcohol in fifty-six parts. This was put into the glass jar before used, and a small gold fish, weighing two drachms and a half, was put in. The jar was covered, to prevent loss of spirit by evaporation. After a few minutes the fish seemed rather more active than before it was put in. At the end of twenty minutes it no longer regarded, or was frightened by, any object touching the jar, and it began to oscillate from side to side when still. Half an hour from the beginning of the experiment it was swimming very much on its side. It did not become appreciably more narcotized, although it remained in the water and spirit until two hours had expired. It struggled whilst being removed into fresh water. In half an hour after its removal it had partially recovered, and when next observed, two or three hours later, it was in its usual state.
Exp. 51. Another small gold fish, weighing rather more than three drachms, was placed, in the same manner, in water containing one twenty-eighth part by measure of alcohol. In less than ten minutes the fish began to move about violently. Soon afterwards these movements became irregular and ill directed, the fish being unable to preserve the perpendicular position, and it no longer observed objects brought close to the jar. It continued, every now and then, to move about violently, and somewhat convulsively, till three quarters of an hour had expired, when it became quieter, floating on its side, and moving only occasionally. The opercula moved, but not regularly. At the end of an hour it had ceased to move its body and fins altogether, and a few minutes later it was found that the opercula did not move. It was placed in fresh water, and in a few minutes the opercula began to move, at first at long intervals, but in half an hour the respiration was regular, and the fish was beginning to move its body. The next morning it appeared quite well.
In Exp. 50 the fish was in the second degree of narcotism, and in the last experiment there was complete insensibility, and the fish would soon have died, probably not from absorption of additional spirit, but because the utmost extent of narcotism cannot be long continued without extinguishing the vital powers.
In some experiments with pyroxilic spirit, or wood naphtha, the same effects were produced on fishes, when it was mixed with water in the same proportion as the alcohol in the two last experiments; but the fishes died several hours afterwards, through the poisonous action of the naphtha, having first, in a great measure, recovered their sensibility and voluntary power.
The two following experiments are introduced for the purpose of showing that chloroform and ether act on fishes in the same way as on other animals.
Exp. LII [52].--Six fluid drachms of water in a small evaporating dish was placed on a plate of glass, by the side of a small dish containing chloroform; the two dishes were covered by a bell-glass, ground at
the edge, to fit air-tight on the glass plate, and left till the next day, in order that the water might be saturated with chloroform, by absorbing it in the form of vapour. As soon as the bell-glass was removed, the small dish of water was put quickly into two pints of water, in which a gold fish was swimming, in a glass jar capable of holding three pints, and the jar was covered to prevent loss by evaporation. In ten minutes the fish began to oscillate a little in swimming. At the end of twenty minutes it was swimming frequently on its side, and then again recovering its balance. Half an hour from the beginning of the experiment the fish floated for a minute or two on its side, at the surface of the water, without moving its body or fins; then it began to swim about again for a time and it continued occasionally to move for a short time, and then again to appear lethargic, until it was removed and put into fresh water, three hours after the commencement of the experiment. It struggled a little whilst being lifted out of the water. In an hour it had in a great measure recovered, and next day was as well as before. The water saturated with chloroform composed a fifty-fourth of the whole, which consequently contained one fifty-fourth part as much chloroform as it would dissolve, and the fish was in the second degree of narcotism.
Exp. LIII [53].--A fluid drachm of ether was mixed with two pints of water, and a gold fish put into it, and the jar was covered, as in the former experiment. As water is capable of dissolving one-tenth of its volume of ether, the water in this experiment contained one thirty-second part as much as it would dissolve. The fish was but little affected during the first hour, but at the end of an hour and a half it inclined to one side in swimming. When two hours had elapsed it was floating completely on its side, and had ceased to move its fins. It was taken out and put into fresh water. It moved a little on being handled. In about ten minutes it began to swim, and the effects of the ether gradually and completely went off.
As the deeper degrees of narcotism cannot be long continued without dangerously depressing the vital actions, so, with an agent whose effects last so long as those of alcohol, a state of complete coma cannot be induced at all without risk, especially if the body be exposed to a low temperature. Ordinary drunkenness does not exceed the second degree of narcotism; the popular term of dead drunk being often applied to a state of sleep from which the individual is still capable of being roused to state of incoherent consciousness. In order to estimate the quantity of spirit that would be required to induce the second degree of narcotism in a man having the average amount of blood, 410 fluid ounces, which were taken as the amount of serum in the body in the earlier parts of this article, may be divided by 56, which will give seven ounces, or three-quarters of a pint of proof spirit. This is a quantity which, I believe, agrees pretty well with general experience. Less than twice this amount, if taken all at once, and on an empty stomach, so as to be quickly absorbed, ought, according to the above considerations, to prove fatal; and there have been many instances of such a result.
A few years ago a man drank a bottle of gin, in the Haymarket, for a wager. He was soon in a state of profound insensibility, and the late Mr. Read, the instrument maker, informed me that when he applied the stomach-pump at the police station, in the presence of medical gentleman, the stomach was found to be quite empty. The man shortly afterwards died. The quantity of absolute alcohol in a bottle (twenty-four ounces) of strong gin is about thirteen ounces. In the fifth case in Dr. Ogston's paper on intoxication,* a woman lost her life by drinking less that a bottle of whiskey (*Edin. Med. and Sur. Jour., vol.xl.); and I believe that it is only by dividing the dose, and thus distributing its effect over a longer time, that any person can, with impunity, take a quantity of spirit exceeding this. The two bottles of wine which, when drinking was less unfashionable than at present, some persons could take after dinner, without being rendered altogether incapable, would contain, according to Mr. Brande's table, from nine to twelve ounces of alcohol; but this quantity was consumed during a protracted sitting, and after eating food, which would further retard its absorption. The difference in susceptibility to the influence of alcohol, though existing to some extent, is not so great as it appears to be. The real difference is more in the way in which the mind is affected by it. A person who is excited evinces the effects of a moderate quantity, which are not so apparent on one who is not excited; whilst to make both individuals quite insensible, the quantity, as in the case of ether or chloroform, would probably not differ more than the size of the individuals, or rather the quantity of blood they might contain. With respect to the large amount of wine and spirits that patients in a state of extreme debility sometimes take without being apparently intoxicated, the following remarks may be made. Such persons are usually incapable of showing excitement under the influence of narcotics; and, as the alcohol is given in divided doses, which are insufficient to cause insensibility or coma, the effects which are really produced pass unnoticed. Long habit has some effect in enabling a person to take a larger quantity of alcohol liquor: this, however, does not arise altogether from the diminished action of the spirit, but partly from experience of the muddled condition, which enables him to control his actions to some extent, and to go about his affairs with a sort of sober aspect when very unfit for business. The woman whose case is quoted above, and who was killed by less than a bottle of whiskey, was a drunkard; and, at all events, the habit of drinking alcohol has no power of enabling persons to increase the dose in the extraordinary manner in which that of opium can be increased.
The amount of anæsthesia from alcohol is apparently as great, in proportion to the narcotism, of the previous centres attending it, as from chloroform and ether. A case occurred in King's College Hospital illustrating this. On Thursday night, the 21st of December, 1848, Mr. Fergusson performed amputation of the leg on an elderly man who had just before sustained a bad compound fracture. The man was very drunk, and Mr. Fergusson informed me that he evinced but little feeling, and did not seem aware of what was being done. He called out once during the operation that he had the cramp in his leg. When I questioned the patient a day or two afterwards, he said that he did not remember anything of the operation, and he supposed that chloroform had been administered to him. This, however, was not the case. Alcohol does not yield sufficient vapour, at ordinary temperatures, to cause insensibility by inhalation in a reasonable time; but, if no better means had been discovered, there can be no doubt that it would have been both practicable and allowable to prevent the pain of severe operations by getting the patient to swallow a large quantity of spirit and water. The end would have justified the means, and, in fact, rendered it as praiseworthy as it is disgraceful when resorted to for the purpose of supposed enjoyment, or to satisfy a craving which has resulted from a pernicious habit.
The general tendency of physiological researches had for some time been to prove that all the strictly animal functions resulted from the combination of the oxygen of the air with the constituents of the body, when Liebig* stated the position more fully and clearly than, as I believe, had previously been done (*Animal Chemistry). His attempted explanation of the physiological action of alcohol, which many persons were inclined to extend to that of ether, on its introduction for inhalation, is in accordance with these views, and is to the following effect†.--That, according to all the observations hitherto made, neither the expired air, nor the perspiration, nor the urine, contains any trace of alcohol after indulgence in spirituous liquors‡ (‡This we shall afterwards find to be incorrect); that the elements of alcohol combine with oxygen in the body, and that its carbon and hydrogen are given off as carbonic acid and water; that the elements of alcohol appropriate the oxygen of the arterial blood, which would otherwise have combined with the matter of the tissues, or with that formed by the metamorphosis of the tissues: and that thus the change of the tissues, and the muscular and other forces which would result from that change, are diminished (†Ibid. p. 239.). Whilst it may be admitted that alcohol diminishes the change of tissues and the functions connected with these changes, and will, indeed, be shown further on that this is true with regard also to the narcotic vapours treated of in this article, it can readily be proved that it is not by appropriating the oxygen in the blood that this diminution or suspension of the molecular change of tissues is effected. The following, amongst other considerations, show this:--First, the carbon and hydrogen of fat, starch, sugar, and gum, as Baron Liebig had the merit of showing, combine with oxygen in the blood, and are given off as carbonic acid gas and water; yet these substances are in no degree narcotic. Second, the carbon and hydrogen of chloroform, which in the laws of its action is almost, if not quite, identical with alcohol, could not possibly combine with oxygen sufficient to act in the way supposed. The amount of carbon and hydrogen in twenty-four minims of chloroform--the quantity which, as it was estimated on a previous occasion, exists in the blood of the adult in complete insensibility,--is only about four grains: an amount totally insignificant when compared to the oxygen which is continually absorbed in the lungs. And, third, if alcohol and the agents allied to it acted by appropriating the oxygen in the arterial blood, breathing air richer than usual in oxygen ought to prevent or arrest their narcotic action. But such is not the case: breathing even pure oxygen does not remove intoxication, or prevent or remove the effects of narcotic vapours. The latter point I have ascertained as regards both the human subject and inferior animals, and have seen insensibility kept up in an animal by the ordinary amount of ether vapour, whilst its skin was of a bright vermilion colour from
the excess of oxygen in the blood.
(To be continued.)
Return to John Snow Publications
Source: Snow, John. Lancet 1, 27 April 1850, pp. 502-03, [Letter to Ed.].
53. "On the treatment of inflammation of the skin."
By John Snow, M.D. Lon.
To the Editor of the Lancet
Sir,--In consequence of the notice, in the last number of the Lancet, of a communication to the Academy of Sciences of Paris, by M. Robert Latour, recommending the application of an
adhesive compound to the skin, in order to arrest inflammation, I shall be obliged if you will allow me a little space in the same journal, in order to express my approval of this treatment, as well as to show that it is not new, but was advocated in the Lancet upwards of seven years ago, and has been practised more or less efficiently from time immemorial. In a paper on Inflammation, which was read at the Westminster Medical Society, and reported somewhat fully in the Lancet, in the early part of 1843, I was led to recommend this treatment, from a consideration of the causes which promote the circulation in the capillary bloodvessels, as well as from the result of experiments by M.M. Breschet and Becquerel, in which the skin of animals was covered with varnish, and from the effects of covering a portion of my own skin closely with oil-silk. The following passages are quoted from the report of that paper:--
"There was one indication which might be fulfilled with safety and advantage in every case of inflammation of the skin--that was, to stop the cutaneous transpiration, which, being the chief function of the skin, promoted the circulation in its capillaries, and thereby kept up its temperature. . . . On this principle he believed that the benefit of water-dressings and poultices chiefly depended, as well as the application of lunar caustic and of flour in erysipelas, the former making a dead, and, in a great measure, an impermeable, membrane of the cuticle, and the latter likewise interfering with transpiration."--the Lancet, Feb. 25, 1843, p. 805-6.
Since the introduction of collodion, I have applied it in erysipelas, with apparently great advantage. In a case of erysipelas of the face and head, which occurred in a lady about thirty years of age, in April last year, this was the only local application. It was applied, once every day, to the whole inflamed surface. The first application to every newly-inflamed part always afforded immediate relief. At the end of six days the inflammation had quite disappeared, and the patient was convalescent. It is in the first stage of inflammation of the skin that protecting it from the air appears to be of most service.--I remain, Sir, your obedient servant,
John Snow, M.D.
Frith-street, Soho, April, 1850.
Return to John Snow Publications
Source: Snow, John. London Med. Gazette 46, 23 August 1850, pp. 321-27 (part 14).
"54. On narcotism by the inhalation of
vapors."
By John Snow, M.D.
[Part 14]
Chloroform passes off unchanged from the blood, in the expired air--Its detection in the urine--in the dead body--in an amputated limb--Remarks on the process for its detection.
At the end of the last paper, reasons were given for concluding that the effects of narcotic vapours were not due, as some had supposed, to the hydrogen and carbon they contain, combining with the oxygen of the air dissolved in the blood; and evidence was adduced to show that if such combination do take place, this would not explain their narcotic action. It still remained desirable to determine by experiment, if possible, whether these bodies are decomposed in the system, or pass off unchanged in the breath, or in other ways. With this view the following experiment was performed:--
Exp. 54.--Ten minims of chloroform were put into a hydrogen balloon, holding 300 cubic inches. The balloon was filled up with air, which I breathed backwards and forwards, in the way in which nitrous oxide gas is taken, for probably about two minutes. The word probably is used, because, after observing the watch for a minute and a half, I lost the recollection of what I was doing, and on recovering so as to observe the watch again, I found that another minute had elapsed, and that I had carefully lain aside the balloon in the meantime. Half a minute after this, and three minute after beginning to inhale, I commenced to pass the expired air through a tube of hard glass, which was placed in readiness in a charcoal fire. To the further end of the tube were fitted other tubes connecting it with two Woolfe's bottles each containing a solution of nitrate of silver. The respired air was taken in by the nostrils and breathed out by the mouth, passing first through the red hot tube, and afterwards through the solutions of nitrate of silver. This process was continued for four minutes. The solution was rendered turbid, more especially that in the first bottle; being at first white, but shortly afterwards of a dark violet colour. At the end of twenty-five minutes from the inhalation, and when scarcely any appreciable effect of the chloroform remained on the feelings, I again breathed the expired air through the red-hot tube, the Woolfe's bottles having been removed, and a small tube moistened inside with solution of nitrate of silver having been attached. A slight precipitate of chloride of silver immediately appeared in the tube. The precipitate in the Woolfe's bottles having been washed and dried on the filter, was found to weigh 1.2 grain.
I have on other occasions, after inhaling chloroform, made the expired air to pass at once through a solution of nitrate of silver without the intervention of the red-hot tube, when not the least precipitate was occasioned; consequently, the chlorine which combined with the silver in the above experiment was the result of the decomposition of chloroform in the hot tube, and not in the circulation. As upwards of half a minute was allowed to elapse, during which several inspirations were taken between the conclusion of the inhalation and commencing to breathe through the tube, the lungs must have been completely emptied of the air taken from the balloon, and the vapour of chloroform must consequently have been exhaled from the blood. The further part of the experiment, performed twenty minutes later, more strongly proves this, and also shows that chloroform continues to be exhaled as long as any appreciable effects of it remain.
If all the chlorine of the chloroform united with the silver, the quantity of chloride obtained in four minutes, in the above experiment--viz. 1.2 grain, would indicate only 0.476 grain of chloroform. But I have found that on passing the vapour of a known quantity of chloroform through a red-hot tube, only about one-third of the chlorine is liberated, chiefly in the form of hydrochloric acid gas, and combines with the silver, as will be more fully explained further on: consequently, the above quantity of chloride of silver may be taken to indicate 1.428, or nearly a grain and a half of chloroform. It would not be easy to continue to test for the whole of the vapour exhaled by the breath. Indeed, breathing through the tubes and liquids for four minutes, in the above experiment, was attended with some inconvenience. But when it is considered that part of the chloroform used must have remained in the balloon, that a further part must have been exhaled before beginning to breathe through the red-hot tube, and that the vapour was still being exhaled twenty-five minutes after the inhalation, the experiment must help to confirm the view that by far the greater part of the chloroform inhaled is exhaled again by the breath.
It is probable that a small portion of chloroform passes out by other channels than that of the expired air: the latter, however, offers such a ready and expeditious outlet, that the quantity excreted in any other way is, most likely, very minute. I have on four occasions examined urine passes after the inhalation of chloroform, by boiling it in a flask, and passing the vapour, first through a red-hot tube, and afterwards through a tube moistened inside with solution of nitrate of silver, and I only on one occasion obtained a very slight precipitate of chloride of silver.
The presence of chloroform can be detected in portions of the body removed by the surgeon, when the patient is under its influence, and in the bodies of animals killed by it. And as this part of the subject is interesting in a medico-legal as well as in a physiological point of view, I shall enter a little more minutely into the account of it than I might otherwise have done. In the Journal de Chemie Médicale for March, 1849, a process for the detection of chloroform in the blood is described in the following terms:--"In order to recognize the presence of chloroform in the blood, we take advantage of the property which this body possesses of being decomposed at a red heat, in giving rise to chlorine and hydrochloric acid. In order to perform the operation, it is sufficient to boil an ounce of blood for some time in a glass flask over the water bath. The vapour must pass through a tube heated to redness at one part, and of which the extremity is smeared interiorly with a mixture of iodide of potassium and paste of starch. A strip of paper moistened with the same mixture may also be put into the tube. If any chlorine be produced by the decomposition of chloroform, the strip of paper will be turned blue. In this way one part of chloroform in 10,000 of blood may be discovered." It is not stated in this article whether the chloroform detected had entered the blood during life, or had been added after
its removal, though the former was probably meant.
In employing this process I substituted solution of nitrate of silver for the starch and iodine test, considering that to obtain some of the chlorine as chloride of silver would be
more satisfactory, in a medico-legal point of view, than merely showing the presence of something which decomposes the iodide of potassium. I find, also, that the nitrate of silver possesses other decided advantages. In the first place, it is a much more certain and delicate test. The iodine test is not acted on by hydrochloric acid, but only by the free chlorine, very little of which is produced by passing the vapour of chloroform through a
red-hot tube, and that not constantly. Again, if there be a trace of chlorine to set free a little of the iodine, a little warm vapour,
which is very apt to rush through the tube, whilst it does not affect the chloride of silver, may either prevent the blue colour of iodide of starch being developed, or suddenly discharge it, as I have seen. And lastly, the nitrite of silver test allows of a quantitative analysis being made, whilst the other does not admit of it. Dr. Alfred Taylor has, however, suggested to me to combine the two tests with a third one, by introducing a slip of starch paper moistened with solution of iodide of potassium, and also a slip of blue litmus paper, into another part of the tube, where it is not wet with the nitrate of silver. Used in this way, these additional tests may tend to confirm the evidence, and to meet objections that might possibly be made to the nitrate of silver test when used alone.
Before relating the experiments in which the presence of chloroform was detected in the body, it will be preferable to give some account of the decomposition which takes place when the vapour of that substance is passed through a red-hot tube. Soubeiran, when treating, in 1831,* of the body afterwards named chloroform, said, that on passing it, in the form of vapour, through a tube of porcelain filled with small fragments of porcelain, and made red-hot, that a good deal of charcoal is deposited, and that a gas is produced formed almost entirely of hydrochloric acid; and that there is found besides a very small quantity of chloride and of an inflammable gas. He added, that, unless the pieces of porcelain are so arranged in the tube as to delay the passage of the vapour, without obstructing it too much, there is more chlorine liberated, and a substance left in the tube which strains paper like an oil. (*Annales de Chimie et de Physique, t. xlviii. o. 135.) Liebig* says of chloroform, "when its vapour is passed through a red-hot tube it is decomposed into carbon, hydrochloric acid, and a crystalline body which appears in long white needles." (*Turner's Chemistry, 8th edit. p. 1009.) On another occasion† he says that this crystalline body is probably the perchloride of carbon discovered by Mr. Faraday (†Annales de Chimie, t. xlix.).
I performed the following experiments with a view more particularly to ascertain whether any appreciable quantity of free chlorine is produced during the decomposition of chloroform at a red heat:--
a. Ten grains of chloroform were put into a dry retort, made out of a small green glass tube, and capable of holding only a drachm. The retort was heated gradually in the water bath. Its beak was kept red-hot by the flame of a spirit lamp, and communicated with two Woolfe's bottles, containing solution of nitrate of silver. Charcoal was deposited in the beak of the retort at the part where it was red-hot: half an inch from this part,
on each side, there was a copious deposit of long white, needle-shaped crystals, and, after a time, a reddish-brown oily-looking liquid appeared. The precipitate of chloride of silver,
which was found almost exclusively in the first bottle, weighed, after being washed and thoroughly dried, 12.5 grains.
b. Ten grains of chloroform were put into a similar retort and treated in the same way, except that the beak of the retort opened under a receiver in the mercurial trough. The deposits in the tube of the retort were the same as before, and 9.15 cubic inches of gaseous matter were obtained in the receiver. The tenth of a cubic inch of water being passed through the mercury, 8.5 cubic inches of the gas were absorbed by it. Solution of potash absorbed one-tenth of a cubic inch more, and the remainder consisted almost, or entirely, of air expelled from the retort.
c. Ten grains of chloroform were treated in the same way as before, the beak of the small retort communicating with two Woolfe's bottles, the first of which contained only thirty minims of distilled water, and the second some solution of nitrate of silver. A very slight cloudiness was merely produced in this solution in the second bottle. The water in the first bottle being added, at the end of the process, to a solution of nitrate of silver, and the precipitate occasioned being boiled in nitric acid, washed, and thoroughly dried, was found to weigh 11.45 grains.
If one of the three atoms of chlorine which were contained in the chloroform were to combine with the single atom of hydrogen, the hydrochloric acid thus produced from ten grains would weigh 3.04 grains, and would suffice to form 12.08 grains of chloride of silver. In experiment a, the chloride of silver obtained exceeded this by a very little. In experiment b, any chlorine which might be developed would be absorbed by the mercury, and the 8.5 cubic inches of gas absorbed by the small quantity of water must have consisted of hydrochloric acid. The weight of it would be 3.24 grains--a very little more than ought by theory to result from the combination of one of the atoms of chlorine with the hydrogen of the formyle; and it would combine to form 12.7 grains of chloride of silver. In experiment c, the thirty minims of water,
whilst they absorbed the hydrochloric acid gas, could absorb but a very minute quantity of chlorine, certainly less than the tenth of a grain, and consequently if a greater amount of chlorine than
this had been evolved it must have passed on to the second bottle, and there caused a precipitate of chloride of silver. On precipitating with nitrate of silver, it will be observed that the quantity of chloride obtained was very nearly that which ought to be formed by the hydrochloric acid produced as suggested above. These experiments, then, tend to show, that if chlorine be produced by passing the vapour of chloroform through a red-hot tube, it must be in extremely small quantity, and that consequently the proper tests to employ are those which indicate the presence of hydrochloric acid.
The following is a brief account of the experiments for the detection of chloroform in the body:--
Exp. 55.--Two kittens about a fort-night old were placed in a glass jar holding 120 cubic inches. Twelve minims of chloroform were dropped
on a piece of blotting paper in the jar, and it was closed. In two minutes the kittens were both insensible, and in two minutes more one of them had ceased to breathe; the other continued to breathe feebly and irregularly for six minutes longer. On the following day one of the kittens was opened: there was no odour of chloroform perceptible in this, any more than in the numerous other animals I have killed with it.
a. The lungs, liver, and kidneys of this kitten were placed in a wide-mouthed glass flask with two or three drachms of water. The flask was placed in the water bath, to which (common salt not being at hand) was added a little chloride of calcium, to increase the temperature somewhat. A tube passing through the cork of the flask was connected with one of hard glass, which was kept red-hot in the flame of a spirit lamp, and to the end of the latter tube was attached one wetted inside with solution of nitrate of silver. About the time that the contents of the flask began to boil, a white curdy precipitate appeared in the latter tube. This precipitate was rendered dark-coloured by the light.
It was insoluble in nitric acid, and very soluble in ammonia.
b. Two days after the death of the kittens, the lungs, heart, liver, and kidneys of the other animal were treated in a similar manner. Soon after the water in the flask began to boil, a precipitate
of chloride of silver appeared in the tube.
c. Three days after their death, the brains of both kittens were put into a flask without any water, and heated in the chloride of calcium bath, as the other parts had been. On this occasion the tube moistened with solution of nitrate of silver ended in a Woolfe's bottle containing a few minims of the same solution. By the time that the liquid which had exuded from the brains began to boil, a precipitate began to appear in the tube, and in a short time there was one also, to a slight extent, in the bottle. The brains were kept boiling in their own serosity for an hour. On the following day heat was again applied to the flask containing the brains which had not been removed; the tube and Woolfe's bottle having, however, been cleaned and supplied with a fresh solution of nitrate of silver. Not the slightest precipitate was obtained on this occasion, although the brains were kept boiling for two hours.
d. Five days after its death one of the kittens was skinned, and the flesh of the limbs, together with the greater part of that of the body and neck, was stripped off and put into the flask and
treated as before, with the exception that, instead of the solution of nitrate of silver, a slip of paper moistened with a mixture of starch and solution of iodide of potassium was placed in the farther end of the tube. After the flesh had been made to boil for a little time in its own juice, a small part of the paper was turned blue.
e. Six days after its death the skin of the other kitten was removed, and its flesh put into a flask and treated as above; on this occasion, solution of nitrate of silver being used as the test.
The serosity of the flesh had scarcely began to boil, when a precipitate of chloride of silver began to appear, and was soon as copious as on any previous occasion, both in the tube and Woolfe's bottle.
At this time the intestines of the kittens were beginning to be offensive, although the flesh used in the experiment was not all decomposed. The bodies had lain on a table since the time of death, at the beginning of last May, when the temperature was cool. From the size of the animals, the quantity of chloroform inhaled by each was considerably less than a grain.
To try the delicacy of the above process, a grain of chloroform was dissolved in a hundred drops of rectified spirit, and one drop of this solution was dropped into a flask containing a thousand grains of water. On treating this as above described, a distinct precipitate of chloride of silver was obtained in the tube, thus indicating the presence of the hundredth part of a grain of chloroform in a thousand grains of water.
Exp. 56.--On May 9, some portions of muscle, nearly sufficient to fill a three-ounce bottle, were taken from the calf of the leg of a little boy, about five years old, which had just been amputated by Mr. P. Hewett, under the influence of chloroform, in St. George's Hospital. About four hours afterwards the pieces of muscle were put into a flask, and treated as before described, solution of nitrate of silver being the test applied. When the liquid exuding from the muscle had been boiling for about ten minutes the precipitate began to appear, and was soon very distinct.
On July 2d, I assisted Dr. Taylor, in the Laboratory of Guy's Hospital, in applying this process to a little of the blood of a man whose death had been occasioned by chloroform, six days
previously. The blood, which had been kept in a stoppered bottle, measured six and a half drachms, was of a dark red colour, fluid, but rather thick, and did not smell offensive. It was put into a clean Florence oil flask, from which a tube proceeded which was made red-hot, and a further tube moistened inside with solution of nitrate of silver. The flask was heated in the water bath, to which, after a time, common salt was added. The process was continued for twenty minutes or more, and although a slight cloudiness was observed in the tube, no distinct precipitate of chloride of silver was obtained. It should be remarked that this small quantity of blood must necessarily have been exposed to the air, before it was put into the bottle, by which means it would lose a part of its chloroform.
At the suggestion of Dr. Taylor, some chloroform (about 8 drops) was put into a flask with an ounce of water, and in the further tube were placed, first, a slip of starch paper moistened with solution of iodide of potassium; next, a slip of blue litmus paper, and the distal extremity of the tube was wetted inside with solution of nitrate of silver. The intermediate tube being made red-hot, as soon as heat was applied to the water bath, the two pieces of paper and the solution of nitrate of silver began to be affected, almost simultaneously: the starch paper being rapidly rendered very blue, the change of colour beginning at one end and traveling rapidly along it.
On the same occasion, in order to try the delicacy of these tests, a drop of chloroform, which is equal to the third of a grain, was agitated in a minim measure with fifty minims of alcohol. Five minims of this solution were added to an ounce of water in a flask, which [325/326] would consequently contain the thirtieth part of a grain of chloroform. A fresh tube being attached, containing the three tests before employed, and the flask being heated in the water bath, a decided effect was, in a little time, produced on all the tests. The starch paper was rendered blue; the litmus paper was turned red; and a very distinct precipitate was obtained in the solution of nitrate of silver.
Exp. 57.--July 13: Half a drachm of chloroform was diffused through a jar holding 670 cubic inches, and a kitten, weighing a little over thirteen ounces, was put in. In two minutes it was quite insensible, and at the end of ten minutes it died. On the 15th the kitten was opened, and the viscera of the chest, the liver, and the brain, weighing together nearly two ounces, were put into a flask and heated in the salt water bath. A tube coming from the flask was kept red-hot, and a further tube contained a slip of starch and iodide of potassium paper, and a slip of blue litmus, and terminated near the bottom of a Woolfe's bottle containing a few minims of solution of nitrate of silver. At the early part of the process, the edge of the starch paper seemed to be slightly changing colour, but after a little time no change of colour could again be observed in it. The blue litmus was very soon reddened, and the solution of nitrate of silver began to be turbid, and the turbidity increased for some time. The viscera were kept boiling in their serosity for half an hour.
On the following day other six ounces of the same kitten were put into the same flask; the intestines, skin, and larger bones being only left. Fresh starch paper was put into the tube which terminated in the bottle containing the same solution of nitrate of silver. After a little time the starch paper was decidedly darkened, at the corner nearest the flask, but only to a limited extent, which did not increase. The parts were kept boiling in their serosity for two hours, when the process was ended by the breaking of the tube at the part where it was red-hot, owing to a little condensed steam being projected against it. At the same moment the limited blueness of the
starch paper was discharged. The tube being left lying on the table, it was found the next day that the starch paper was very blue throughout its entire extent, from what cause I do not know. The precipitate of chloride of silver was separated by filtration, and but for an accident would have been dried and weighed. There appeared to be not less than the twentieth part of a grain of it.
There is no deposit of carbon in the red-hot part of the tube in this process, as the apparatus always contains sufficient air for the formation of the carbon into carbonic acid. The white needle-formed crystals previously mentioned are deposited, but not in sufficient quantity to be of service as a test. It is desirable to make the tubes proceeding from the flask incline a little upwards, so that the vapour which is condensed before reaching the red-hot part may flow back again. I consider that the solid organs of the body should be taken for analysis, in preference to the blood in a separate state, as that contained in the minute vessels is protected from the action of the air. The parts should be cut in pieces, and put into the flask, without any addition. The stomach should not be selected for examination by the above process, as the gastric juice contains a minute quantity of free hydrochloric acid, and hence the evidence would be liable to objection. The intestines also do not seem suitable parts for examination, as the sulphuretted hydrogen they might contain would interfere, more or less, with the tests. In other respects it matters little what part of the body be used, further than that the most vascular parts are the best. As regards a quantitative analysis, it results from some of the experiments, detailed in an early part of these papers,* that, in a case of death from chloroform, a quarter of a pound of any organ of average vascularity would contain about the twelfth part of a grain, which, if the whole of it were separated and decomposed, would produce about the tenth of a grain of chloride of silver. (*[part 5, in] Med. Gaz., vol. xlii. p. 415.)
The process above described does not prove the presence of chloroform itself, but only that of a volatile compound containing chlorine. In this respect it resembles the processes for the detection of arsenious acid and corrosive sublimate in the tissues, which prove only the presence of a compound of arsenic, or of mercury. The only compounds containing chloride which are volatile at the heat of boiling water, are substances such as chloride of ethyle, Dutch liquid, and some others, which resemble chloroform in their effects, but are none of them in common use. In order to be quite certain that the precipitate is no other salt of silver than the chloride, besides the tests of ammonia and nitric acid, solution of potash might be added to another portion of it, as recommended by Dr. Taylor, in treating of hydrochloric acid.* (*Medical Jurisprudence, p. 91.) Potash does not change the chloride of silver without heat.
With these limitations and precautions the process is, I believe, liable to no fallacy. There are chlorides in the body, but they cannot be decomposed, except at a high temperature, and not till the part under examination should become dry, which, in the method here described, could not take place in the most protracted examination. Besides, I have made several examinations of parts not containing chloroform without meeting with anything that produced the slightest effect on the nitrate of silver, or on the starch or litmus test. The bodies of two kittens killed with the vapour of ether were submitted to the process, by portions at a time, which were made to boil in their own serosity for an hour or two, but not the least effect was produced on any of these tests. Hearing, in the beginning of May last, that chloroform was suspected, by some of the coroner's jury, to have been used in the case of a woman who was found dead, under mysterious circumstance, in the Wandsworth Road, I applied to Mr. John Parrott, who was polite enough to send me some portions of the body, including part of the brain and liver. They had been kept in a covered jar from the time they were removed from the body. The chemical examination commenced four days after death, whilst the parts were fresh, and although very carefully conducted, not the least effect was produced, either on the nitrate of silver or starch and iodine test.
(To be Continued)
Return to John Snow Publications
Source: Snow, John. Medical Times 22, 31 August 1850, pp. 228-31, [Letter to Ed.].
55. "Remarks on the administration of chloroform, in answer to Professor Lizars."
By John Snow, M.D.
Vomiting under the Influence of Chloroform attended with no Danger.--The Glottis not Paralyzed.--Safety and Advantages of Chloroform in large Operations, involving the Mouth.--Objection to Administering it on a Handkerchief.--Necessity and Advantages of an Apparatus.--List of Deaths from Chloroform.--Means of Avoiding all Danger in giving it.
I regret to differ in opinion from Professor Lizars on some practical points of his letter in the last number of the Medical Times, respecting the administration of chloroform; but, however unpleasant it may be to differ from so deservedly eminent a surgeon, it becomes the more a duty to correct what one believes to be erroneous, on account of the increased attention which his fame must command for his statements. What I conceive to be the errors in question appear to have arisen from Professor Lizars not having given the subject the amount of study and attention that it requires. He says, that those administering chloroform "have only to attend to two important points in order to insure safety to the patient. The first indication is to give directions to the patient that his stomach be kept empty." He proceeds to say, "for that reason operations should be performed before breakfast, as chloroform always produces vomiting when the stomach is full, and the rejected fluid is liable to enter the paralysed glottis and produce suffocation. To this cause I apprehend the great proportion of those who have died under the influence of chloroform may be ascribed." The italics are his own. I entirely agree in the propriety of an empty stomach preparatory to the inhalation of chloroform; but if any one thinks this a means of avoiding danger, he might be seriously disappointed in a case in which danger should really exist. I, as well as others, had been in the habit of directing patients not to take food for two or three hours before inhaling ether, and the same directions have been given since the introduction of chloroform. But it constantly happens that I have to give it to patients whom I have not seen before, and to whom the surgeon has omitted to give directions on the point, and not unfrequently the patient has taken a meal just before I arrive; yet in no case has the inhalation been either postponed or omitted on that account. The patient is, indeed, liable, though by no means certain, to vomit when the stomach is full, but the vomiting has not, in any case, been attached with ill consequences of any kind, and I have seen, at least, two hundred patients vomit whilst partially under the influence of chloroform. In two or three cases, in fact, the patient who had eaten a very full meal, vomited and inhaled by turns during the whole operation. If the rejected fluid were liable to enter the glottis, of course there would be some inconvenience, either at the time or afterwards. As Professor Lizars is so afraid of the patient having food in the stomach before inhaling, it may safely be assumed, that his experience of vomiting, after chloroform, is by no means so large as that stated above. As regards his apprehension, that the great proportion of deaths are due to this cause, the simple answer to it is, that the patients who have died from the effects of chloroform did not vomit, and that nothing was found in the windpipe to obstruct respiration, in such of them as were examined after death.
Having stated the facts bearing on the question of vomiting, I may proceed to the theory of the subject, and, for an explanation, need not go further than Professor Lizars's own letter. At the concluding part, he says, "in the administration of chloroform, I have stated, that the constant production of retching, proves that the pneumogastric nerves are excited." Now, although retching occurs only occasionally, and never whilst the patient is deeply narcotised; yet, if it prove that the pneumogastric nerves are excited, it explains why the glottis, which is supplied by branches of these nerves, is not paralysed. The truth is, that the glottis is one of the organs of respiration, and retains more or less sensibility as long as the patient has sensibility enough to breathe. And so long as there are sensibility and energy sufficient to effect the complicated act of vomiting, the functions of the glottis appear to be unimpaired. When the narcotism from chloroform is confined within reasonable bounds, there is as little danger of blood getting into the windpipe, in operations involving the mouth, as of vomited matters in other cases. When the first fatal instance of inhalation of chloroform occurred in a girl near Newcastle, Dr. Simpson hastily asserted that she had been suffocated by some brandy given to her when dying, although but a teaspoonful was given which was swallowed, and ever since that time there has been a prejudice in Edinburgh against giving chloroform in large operations involving the mouth. Severe pain, has consequently, been inflicted in many such cases in that city; whilst in London probably nine-tenths of these operations have been performed under chloroform. If much blood flow into the throat there will always be some embarrassment to the respiration, whether a patient be insensible or not. The practice in such cases always was to lean the patient's head forward now and then, and, if this be still attended to[,] the blood does as little harm under the proper influence of chloroform as without it. I cannot but think that Professor Lizars must have been mistaken in the case of tooth-drawing, in which he supposed that the blood trickled down the glottis. I have given chloroform in many cases, in which from eight to twelve teeth were removed at one operation; and, although subsequent vomiting, in some of the cases, revealed a good deal of blood which had been swallowed or flowed down the pharynx and esophagus, there were never any symptoms of a drop having entered the windpipe or lungs. That the glottis is fully competent to take care of the air passages, and that suffocation is not very readily caused under the influence of chloroform, I have further ascertained by putting the heads of animals under water whilst insensible. These experiments will be given in detail on another occasion; but I may mention that a cat lay, in one instance, exactly two minutes with its head under the liquid, and readily recovered soon after being withdrawn.
It may be interesting to some of the readers of the Medical Times, if I enumerate some of the more important operations about the mouth in which I have administered chloroform. I may preface the account by mentioning an operation performed by the late Mr. Liston, in which ether was the agent employed, as showing that he was not afraid of narcotism in operations involving the mouth. The operation consisted in the removal of a very large tumour occupying the central part of the lower jaw, in a young lady. The bone was divided far back on each side.
Mr. Tatum removed a very large tumour of the lower jaw in a man in St. George's Hospital, and one by Mr. Fergusson in King's College Hospital; also one in a gentleman, in private practice, by that surgeon. The superior maxillary bone was removed on two occasions, in St. George's Hospital, in which I gave chloroform, and also, on three occasions, by Mr. Fergusson also removed the superior maxillary bone in the case of a lady. In these, and similar operations on the face, the patients were first made insensible by means of the inhaler, and the insensibility was kept up during the operation by means of a sponge applied near the mouth from time to time; not more than about fifteen or twenty minims of chloroform being put on the sponge at once. Besides the prevention of the dreadful pain, the chloroform has the further advantage, in large operations on the face, of greatly diminishing the tendency to syncope from the unavoidable loss of blood. I have seen no ill effects from it in any case. One patient died soon after the operation, and I have explained the cause of death at some length in the Medical Gazette for February 9, 1849.
In the operations for nasal polypi, and for epulis, a good deal of blood generally flows backwards into the throat, but without any injurious consequences. In the operation for hare-lip, when the child is laid on its back, the blood also flows into the throat, if more than a few drops be lost, and is either all swallowed, or part of it is allowed to flow out by turning the child quickly round for a moment now and then. Mr. Fergusson operates with the child in this position, and I have administered chloroform in twelve of his operations for hare-lip within the last two years. Two of the children were but three weeks old, and two or three of the others were under three months.
Besides having the stomach empty, the other point to which Professor Lizars considers it necessary to pay attention, in order to avoid danger, "is the allowing the patient to breathe atmospheric air along with the chloroform." He adds, that "an experienced assistant is required to administer the chloroform, and to do nothing else. He must watch its effects, allowing fresh atmospheric air to enter the nostrils and mouth occasionally during its administration and influence, otherwise the blood may become too greatly carbonised, and death ensue." These remarks are, on the whole judicious; but it is not easy to understand his exact meaning respecting the atmospheric air. If he considers that patients can inhale the vapour of chloroform unmixed with air, that is an error into which a great part of the speakers at the Académie de Médécine fell, in a discussion which took place last year. No human being has breathed unmixed vapour of chloroform, or ever will, as it can only exist in a separate state, at the ordinary pressure of the atmosphere, when raised to the temperature of 140°; or at the ordinary temperature, when the atmospheric pressure is reduced to about one-sixth the usual amount. The experiment of inhaling pure vapour of chloroform could only be tried on a small animal under the receiver of an air-pump. Professor Lizars, perhaps, means, however, that the mixture of vapour and air must be intermitted, and breathed by turns with air surcharged with vapour. This, however, is not at all requisite if the vapour be diluted to a sufficient point. If, for instance, the patient be breathing 95 to 96 per cent of air, with 4 or 5 per cent of vapour of chloroform, it will be unnecessary to intermit the process till insensibility be complete. It is not sufficiently understood, or, at least, borne in mind, that the vapour of chloroform requires to be largely diluted with air, not for the purpose of respiration, (its physical constitution ensures that,) but to prevent its operating with dangerous rapidity. In proof of this, it is only necessary to state the circumstance, that, in giving ether, only 70 to 80 per cent of air is breathed with 20 or 30 per cent of vapour; whilst, in the case of chloroform, there should be 95 or 96 per cent. of air; and, in the case of hydrocyanic acid, which I have administered in the Hospital for Consumption, there must be over 99 per cent of air, with much less than 1 per cent of vapour.
Professor Lizars recommends chloroform to be administered by putting two drachms or so upon a handkerchief. [229/230] This is the plan of Dr. Simpson. I have taken every proper opportunity, since the time when chloroform was first introduced, of opposing its use on a handkerchief in the way recommended; but I cannot hope that anything that I can write will receive one-tenth the circulation of the pamphlet issued by the Physician-Accoucheur to the Queen in Scotland, and copied into all the newspapers in the kingdom, when he first tried the effects of chloroform in an undiluted state, on the recommendation of Mr. Waldie, of Liverpool. The small amount of safety attending the use of the handkerchief may be judged of from Professor Lizars's estimate of that safety, notwithstanding his two points which he supposes to secure it. He admits that chloroform is a valuable agent in large operations, but others, attended with a not much less amount of pain, as the amputation of a finger or toe, he would have to be performed without it. Now others, as well as I, who have formed our opinion of it, from its use with a suitable inhaler, have no hesitation in recommending it in the smallest operations, being sure that with skill and care it is quite free from danger. I have twice taken chloroform to have a tooth drawn, and would not undergo a similar operation without it, so long as I could get a skilful person to administer it with a suitable apparatus.
Professor Lizars considers an instrument indispensable for giving chloroform to horses, but says, "in human surgery no inhaler or any instrument should ever be used; it is highly reprehensible--many lives must have been sacrificed to its employment." Now, an inhaler is not necessary for the horse any more than for man, except as a means of rendering the process more agreeable, manageable, certain, and safe; all which points it is our duty to consult in the human subject, as much as in the horse, although, perhaps, the former is the less deserving creature. Professor Lizars must have seen some very imperfect form of inhaler, perhaps with a tube to enter the mouth. He can hardly be aware that a former pupil of his own, who is now justly eminent, not less for his observations on ether and chloroform than on many other subjects--I allude to Dr. Francis Sibson--contrived an inhaler whilst at the Nottingham Infirmary, and disapproves of the handkerchief. With respect to the inhaler which I employ, it allows of such easy respiration that a person might wear it day and night for an indefinite period, uncharged with chloroform, and removing it to take his meals, without injury to his health. To prove that the handkerchief and not the use of inhalers has been the chief cause of the deaths from chloroform, it is only necessary to enumerate the fatal cases.
2. Feb. 23, 1848. Mrs. Simmons, of CincinattiU.S. Extraction of teeth. Inhaler; no medical man present.
3. A young woman at Hyderabad, in Hindostan. Distal phalanx of a finger. Handkerchief.
4. May, 1848. Madlle. Stock, aged 30, at Boulogne. Opening an abscess. Handkerchief.
5. Dec., 1848. Young gentleman at Govan, near Glasgow. Intended toe-nail operation. Handkerchief.
6. Jan. 24, 1849. J. Verrier, aged 17, Lyons. Intended amputation of finger. Handkerchief.
7. Feb. 20, 1849. Samuel Bennett, Westminster. Amputation of toe. Handkerchief.
8. Aug. 23, 1849. Mdme. Labrune, Langres, France. Intended extraction of tooth. Handkerchief.
9. Oct. 10, 1849. John Shorter, aged 48, St. Thomas's Hospital. Toe-nail operation. Inhaler; given by a non-medical person.
10. Nov., 1849. Girl Jones, Shrewsbury. Removal of eyeball. Not stated.
11. Young lady, Berlin. Intended extraction of tooth. Napkin.
12. Feb., 1950. Artilleryman, Mauritius. Amputation of last phalanx of middle finger. Handkerchief.
13. Alex. Scott, aged 34, Guy's Hospital. Removal of portion of hand. Handkerchief.
These, I believe, comprise all the recorded cases in which death was clearly due to the administration of chloroform.
In one of the cases it is not stated that a handkerchief was used, though, from the context of the report, that seemed to be the case. Of the other twelve an inhaler was used in only two of the cases, and in neither of them was it used by a medical man, whilst, in the ten instances in which death was caused by chloroform on a handkerchief, it was administered by a qualified medical man in every instance but one. There have been four cases in which death was accidentally cause by chloroform taken by the deceased parties when no one else was present. Two of these deaths occurred in Scotland. A handkerchief was used in each instance, and, but for the practice of taking chloroform on a handkerchief, these persons would probably never have taken it at all. However, I have not included these cases in the above list. There was a death commonly attributed to chloroform which I have not included in the list--that which occurred at Mr. Robinson's the dentist; for I believe that that was case of fatal syncope, due to mental emotion in a subject with fatty degeneration of the heart, and great enlargement of the liver. He was only just beginning to inhale, when he suddenly died. In that case an inhaler was employed.
Other supposed causes of the deaths from chloroform have been suggested by various writers, besides those above mentioned, only one of which I shall notice. Many persons, especially in Edinburgh, have attributed the fatal cases to the impurity of the chloroform employed; but, in the first place, it has been examined in nearly all the cases, and found, to be quite good. And, again: although it might contain impurities which would cause irritation at the time, and subsequent disagreeable effects, it could not become contaminated with anything likely to cause sudden death; and, before this assertion is repeated, we ought to be told with what substance stronger than itself chloroform is liable to be contaminated. I fully admit the necessity of having chloroform, as well as other medicines, quite pure; as its adulteration, though not liable to cause death, may cause disappointment, and other disagreeable consequences; and it must also be admitted, that this, as well as other drugs are liable to impurity, both in London and elsewhere. I am of opinion, however, that impure chloroform has not been supplied by the respectable houses of this metropolis. I generally use Mr. Morson's chloroform; but have, at one time or other, used that of Mr. Squire, Mr. Jacob Bell, Mr. Bullock, Mr. Hooper, Mr. Taylor, and others, and always found it good. I have also used the chloroform of Messers. Duncan, Flockhart and Co., of Edinburgh, and cannot give it any better praise than by saying it was equally good. If the Edinburgh people wish to assert that they can produce something better than pure chloroform, they must call it by another name, for it must be a different medicine.
The real cause of deaths from chloroform undoubtedly is, that in each case the patient has had an overdose; I mean more than was necessary to render the patient, or one of similar size and strength, insensible. By a dose of chloroform, however, must be understood, the quantity inhaled during an operation. For instance, when the inhalation is left off for two or three minutes, a great part of the chloroform exhales by the breath, and the patient perhaps requires to inhale a little more. This should be considered a repetition, and not an increase of the dose.
The necessary points to be observed, in order to avoid the risk of giving an overdose, are, 1st, that its vapour be systematically diluted with a sufficient quantity of air, by means of a suitable apparatus--when no accident can happen, without the continued neglect of evident warning symptoms; and, 2nd, that the person exhibiting the chloroform should keep his whole attention directed to the patient, and be able to understand all the signs that occur. I have not space here to go fully into the description of the signs which indicate when the inhalation should cease, and an operation begin, but would refer to some papers of mine, "On Narcotism by Inhalation," in the Medical Gazette, 2nd vol. for 1848, and also to some papers on "Chloroform," by Dr. Sibson, in the same volume. I may state, however, that it is chiefly by attention to the state of the respiration and the eye, that danger is to be avoided. The pulse may be felt as a physiological inquiry, or with reference to the operation, but gives no guiding information concerning the chloroform, for the following reasons:--When the vapour is diluted to a safe extent, it might be continued till death, as I have ascertained in animals, and the pulse would still beat distinctly for many seconds after the respiration had ceased; and if, on the other hand, the vapour be of dangerous strength, the heart might suddenly cease to beat, and the first intimation of danger from the pulse would come only too late.
If chloroform be given on a handkerchief at all, not more than from fifteen to twenty minims(a) should be put on at once ((a) Drops of chloroform are widely different from minims, being extremely small). In this way it may be given in midwifery, as that quantity, and often much less, suffices for each application; but in surgery, where the full effect is required, this would be insufficient.
Frith-street, Soho-square, Aug. 27, 1850.
Return to John Snow Publications
Source: Snow, John. London Med. Gazette 46, 1 November 1850, pp. 749-54 (part 15).
56. "On narcotism by the inhalation of vapors."
By John Snow, M.D.
[Part 15]
Detection of ether in the expired air after inhalation--Detection of alcohol in the expired air after it had been taken into the stomach--The effects of chloroform and ether prolonged by causing the exhaled vapour to be re-inspired.
In my last communication it was shown that the vapour of chloroform can be detected by chemical tests, as it exhales from the blood in the expired air. The strong odour of ether, which continues to be perceived for hours in the breath of persons who have inhaled it, is a pretty good indication that this medicine is exhaled from the blood in a similar manner. I thought it desirable, however, to have a more material proof of the fact, than that afforded by the odour, and therefore contrived and performed the following experiments:--
Exp. 58.--As a preliminary measure I passed the expired air for twenty minutes through strong sulphuric acid, inspiring by the nostrils, and expiring by the mouth, through a spiral tube immersed in cold water; a continuation of this tube afterwards dipping into half an ounce of sulphuric acid contained in a bottle. The acid was afterwards boiled in a small retort, the beak of which communicated with a gas receiver under water. No gas was obtained beyond the air expelled from the retort by the heat, and the acid was not changed in colour.
Exp. 59.--On the following day--August 1st, I inhaled three fluid drachms of ether gradually, in the course of four minutes, and was rendered almost unconscious. After waiting for a minute, in order that the lungs might be entirely emptied of the vapour remaining at the conclusion of the inhalation, I commenced to pass the expired air through sulphuric acid, the air first passing through a spiral tube immersed in iced water, to condense the watery vapour, as in the last experiment. This procedure was continued for twenty minutes. A [749/750] few hours afterwards the sulphuric acid was placed in a small retort, the beak of which communicated with a receiver under water, and was heated with the flame of a spirit lamp. It was gradually rendered quite black by the heat, and 11.3 cubic inches of gas were obtained in the jar. The jar being transferred to the mercurial trough, and solution of caustic potash being introduced, the contents, after standing for an hour or two, and being agitated occasionally, till no further reduction of bulk would take place, were diminished to 3.9 cubic inches, showing an absorption of 7.4 cubic inches of carbonic acid gas. The jar being reversed, and a lighted taper being applied to its mouth, its remaining contents took fire, and burnt with a bluish flame. As 2.6 cubic inches of air were contained in the retort at the commencement of the process, the quantity of inflammable gas was probably 1.8 cubic inch.
Exp. 60.--On August 2nd, I again inhaled three fluid drachms of ether, and proceeded exactly as in the last experiment. The sulphuric acid was rendered black as before, and 7.6 cubic inches of gas were collected in the receiver. Potash absorbed 3.2 cubic inches of this, and the jar being reversed and a lighted taper applied to its mouth, the remaining contents burnt with a flame which gradually descended in the jar to the surface of the mercury. Allowing for the air expelled from the retort, the quantity of combustible gas was 1.6 cubic inches.
Exp. 61.--In order to ascertain the nature of the inflammable gas produced, another experiment was performed, on a subsequent day. The same quantity of ether was inhaled, and the expired air was passed through sulphuric acid in the same manner. The acid was boiled in the retort until 7.1 cubic inches of gas were obtained in the receiver, when the process was stopped. Solution of potassa being agitated in the gas absorbed 3.5 cubic inches. Two cubic inches of oxygen gas were added to the remaining 3.6 cubic inches, and a portion of the mixed gases was transferred to Dr. Ure's eudiometer. As it did not explode with the spark from a small electric machine, a small quantity of pure hydrogen gas was added, when explosion took place with the following result. The quantities are in hundredths of a cubic inch:--
Hydrogen
........
3.0
Oxygen, [etc.]
........
21.0
Total
........
24.0
After explosion
........
16.5
Loss of volume
........
7.5
being a diminution of three parts more than the hydrogen would occasion. The remaining 16.5 parts were agitated with a little solution of potassa, when a further diminution of about six parts took place; a little more than ten parts being left. This result shows that the inflammable gas under examination was carbonic oxide, which, in becoming converted into an equal volume of carbonic acid, consumes half its own volume of oxygen. The beak and upper part of the small retort contained 1.9 cubic inch of air, which would be necessarily expelled into the gas receiver, and when this and the oxygen afterwards added are subtracted, the remainder is in the same proportion, very nearly, as the carbonic acid produced by the explosion; consequently the gases obtained by heating the sulphuric acid were carbonic acid gas, and carbonic oxide.
In these experiments, the ether passing off in the expired air is in part absorbed by the sulphuric acid, and on the application of heat is decomposed into various products; the above gases being given off, and free carbon remaining in the acid, and rendering it black. Sulphurous acid gas is evolved, but is absorbed by the water. On adding a few minims of ether to half an ounce of sulphuric acid, and operating in the same way as in the above experiments, the same products were obtained. Alcohol, when heated with a large excess of sulphuric acid, yields the same products as ether; but as I had taken no kind of fermented liquor before inhaling the ether in the above experiments, these products must have resulted from the sulphuric ether.
From the general resemblance between the action of alcohol, ether, and chloroform, and from these substances being governed in their action by some of the same general laws, as previously shown in the experiments of frogs and fishes,* (*Med. Gaz., last vol., p. 622)it might be expected that since chloroform and ether can be shown to pass off in the expired air, alcohol would also [750/751] be exhaled in the same manner. Common experience, so far as the sense of smell is concerned, is in accordance with this view. Leibig [sic], however, says,* "according to all the observations hitherto made, neither the expired air, nor the urine, contains any trace of alcohol, after indulgence in spirituous liquors" (*Animal Chemistry, p. 239). This, so far as I know, was true as regards the human subject, but Dr. Percy† had obtained alcohol by distilling the urine of a dog, to which he had given a fatal dose of it (†Prize Thesis "On the Presence of Alcohol in the Brain," etc.).
Feeling a strong conviction that alcohol must pass off in the breath, I have made many experiments during the last twelve months, with a view to detect it. At first, I caused the expired air, after spirit had been drunk, to pass, for an hour or longer, through a spiral tube, immersed in ice and salt, but did not succeed in detecting alcohol in the condensed water. A little reflection, however, made it evident that alcohol could only exist there in extremely minute quantities; for the spirit which had been taken, being equivalent only to two ounces of absolute alcohol, the inspired air would only be able to take up about a two-hundredth part as much vapour of alcohol as would saturate it, at the heat of the body; and it would be in vain to attempt to reduce the air to such a low temperature as would cause it to deposit any part of so relatively small an amount of vapour; in other words, the alcoholic dew-point of the air must be lower than the temperature of the ice and salt, and , consequently, all the spirit that could be arrested would be that which might be attracted by the small quantity of condensed water. By collecting together the water condensed from the breath in six different experiments, I succeeded, however, in obtaining spirit in a pure state, as will be detailed further on.
In the following experiments the same method was employed, as detailed above, for the detection of ether.
Exp. 62.--August 6th, 1850. Two ounces and a half of rectified spirit of wine, of 80 per cent, were diluted with rather less than a pint of water, and taken, with bread and butter, at suppertime. A slight feeling of inebriation was occasioned by it, but not sufficient to interfere, in the least, with the proper performance of the experiment. The air was afterwards taken in by the nostrils and breathed out by the mouth, through a wide tube communicating with a metal box containing a spiral arrangement, by which the air was obliged to pass round several times. This box was surrounded with ice. The air was conducted next, by a glass tube half an inch wide to the bottom of a bottle containing half a fluid ounce of sulphuric acid. The object of condensing the moisture of the breath, in the metal box, was to prevent its diluting the sulphuric acid beyond the point at which it ceased to decompose alcohol when heated. The expired air was, in this manner, passed through the sulphuric acid for thirty-five minutes. Care was taken that no air coming from the stomach by eructation should pass into the apparatus. Two and a half fluid drachms of clear water were condensed in the metal box. The following morning, the sulphuric acid was put into a small retort, communicating with a gas receiver over water, and heated with the flame of a spirit lamp. The acid was rendered quite black, and 5.1 cubic inches of gas were obtained, of which 2.6 cubic inches consisted of air from the retort. The receiver being transferred to the mercurial trough, and a little solution of potassa introduced, 1.65 cubic inches were absorbed. The jar being inverted, and a light applied to its mouth, the remaining contents took fire, the flame gradually descending in the jar to the surface of the mercury. The quantity of inflammable gas was 0.85 cubic inch.
Exp. 63.--Another night the same quantity of rectified spirit was taken, in the same manner, and the expired air passed through the spiral box and the sulphuric acid as before. Six fluid drachms of acid were employed this time, and the process of breathing through it was continued for an hour. Two and a half drachms of water were again condensed in the metal box, and the acid was increased in bulk by rather more than half a drachm. The sulphuric acid was next morning placed in a retort and heated. It was turned black, and six cubic inches of gas were obtained, two of which consisted of air from the retort. Solution of potassa absorbed 3.45 cubic inches of carbonic acid gas, and the remaining contents of the receiver burnt with a slight explosion, on a light being applied. The inflammable gas did not amount to more than 0.55 cubic inch.
Exp. 64.--The same quantity of rectified spirit was taken at night on another occasion, and the expired air passed for an hour through sulphuric acid in the same way as before. The quantity of acid employed this time was a fluid ounce. On the following morning six drachms of the acid were heated in a small retort: they were rendered quite black, and somewhat viscid. 4.85 cubic inches of gas were obtained in the receiver, of which 1.8 cubic inch consisted of air from the retort; potash absorbed 0.6 cubic inch; 0.85 cubic inch of the remainder was transferred into a small jar, to the mouth of which a taper was applied, when the contents burnt for a little time with a bluish flame. To the residue in the receiver 3.8 cubic inches of oxygen were added, and a portion of the mixture was introduced into the eudiometer. As it did not explode with the electric spark, a small quantity of pure hydrogen gas was added, when an explosion was effected with the following result:-
Hydrogen
........
3.0
Oxygen, etc
........
32.0
Total
........
35.0
After explosion
........
27.0
Diminution
........
8.0
being a loss of 3.5 more than occasioned by the hydrogen.
Solution of potassa being agitated in the remaining 27 parts, they were diminished to 19; showing an absorption of 8 parts of carbonic acid. The loss of volume was consequently very nearly half as great as the quantity of carbonic acid gas produced by the explosion; and therefore the inflammable gas under examination was carbonic oxide, the amount of which was just one-fourth of the mixed gas introduced into the eudiometer. It is evident on calculation that nearly 1.8 cubic inch of carbonic oxide must have been expelled from the retort, and that this and the carbonic acid were the only gases evolved by the sulphuric acid.
The decomposition which the alcohol, absorbed from the expired air, undergoes in the sulphuric acid is the same as that undergone by the ether in the experiments previously detailed.
Exp. 65.--The water condensed in the metal box, surrounded with ice in the above three experiments, and in three others not related, amounted together to two ounces. It was placed in a retort, and about three drachms were distilled. This product was placed in a smaller retort, and about twenty minims were distilled into a small test tube. Dry carbonate of potassa was added to this till it would dissolve no more. In a little time a layer of clear spirit, about the tenth of an inch in thickness, floated on the top of the solution of potash. A piece of asbestos being dipped in this, it burnt with a blue flame. A very little powdered camphor was dropped into a small tube, drawn at one end to a capillary point. This point being brought in contact with the liquid floating on the solution of potash, a little of it rose by capillary attraction, and was observed to dissolve the camphor within. On blowing at the other end of the tube, a minute drop of solution of camphor was forced out, and received on a piece of glass, when the spirit immediately evaporated, leaving a coating of camphor. These tests leave no doubt of the presence of alcohol. The process used in this experiment is similar to that employed by Dr. Percy for the detection of alcohol in the brain and other organs.
Exp. 66.--Two and a half fluid ounces of rectified spirit, of 80 per cent, were diluted with water, and taken at suppertime. The air was afterwards inspired for fifty minutes by the nostrils, and expired by the mouth, through a glass tube which dipped into three ounces of water contained in a bottle. Next morning the water was put into a retort, and about three drachms were distilled, which were put into a smaller retort, and about twenty minims were distilled into a small test tube. On carbonate of potassa being added in excess, a thin layer of clear liquid floated on the surface. This was proved to be alcohol; for a little bit of asbestos being moistened in it, burnt with a blue flame, and it dissolved camphor in the way described in the former experiment.
Whilst the above experiments show that alcohol is exhaled in the breath after it has been taken into the stomach, a little consideration will prove that only a small part of it can be excreted in this manner. When there are two ounces of alcohol in the blood, the air which reaches the lungs can only take up, as stated before, about a two-hundredth part as much as would saturate it at the temperature of the blood. At this rate, a person breathing the usual amount of air would only exhale about twelve minims of alcohol in an hour; consequently, if it had to pass off entirely in the expired air, its effects would continue for a very much longer period than they do; and, since alcohol can hardly be detected in the other excretions, it must be decomposed in the system into fresh products.
I have assumed from the first that the speedy subsidence of the narcotism caused by chloroform and ether, in comparison with that from alcohol and other narcotics, depends on the volatility of the former substances, which allows of their ready exit by the expired air. Indeed, the effects of these medicines usually subside in the period which a calculation founded on this view would assign to them. It was previously estimated, for instance, that twenty-four minims of chloroform are contained in the blood of an adult of average size in a state of very complete insensibility; this being about one twenty-eighth part as much as the blood would dissolve. The inhalation being now discontinued, the fresh air which reaches the air cells will abstract from the blood nearly one-twenty-eighth part as much as it can hold in suspension at the temperature of 100°; and as each hundred cubic inches of air, when saturated at 100°, contains 43.3 cubic inches of vapour of chloroform, 43.3÷28=1.54 cubic inches, or 1.48 minims, will be the quantity removed by the first hundred cubic inches of air which reaches the air-cells. It has been shown that about half the inspired air gets as far as the air-cells; and, supposing the patient to be breathing 400 cubic inches in the minute, 200 cubic inches would act in the removal of the vapour. In this manner it would take two minutes and a half to reduce the quantity of chloroform from 24 to 18 minims, and the narcotism from the fourth to the third degree; after which the effects would diminish more slowly, and in three and a half minutes longer the narcotism would have diminished to the second degree. Then, as the air would only take up about one-fifty-sixth part as much as it would hold, in about five minutes longer we might expect the return of consciousness; and the slight dizziness or confusion which might remain would subside still more gradually. The above statement expresses pretty well what usually occurs when the inhalation has been kept up for a little time. Children recover from the effects of chloroform more rapidly, on account of their quicker circulation and respiration. Old people, on the other hand, more slowly, for the opposite reason. When insensibility is produced in the course of two minutes for a short operation, and the inhalation is not repeated, the effects of the vapour subside more quickly than stated above; because, at the same time that the chloroform is passing off by the lungs, it is also escaping from the main current of the circulation, by permeating the coats of the small vessels, and diffusing itself in the tissues, and thus allowing the brain to resume its functions.
Ether is more volatile than chloroform; but being also much more soluble, the relative quantity absorbed into the system is so much greater, as to more than compensate for the superior volatility; and consequently the effects of ether subside somewhat more slowly than those of chloroform, the ether taking rather longer to pass off in the expired air.
It follows as a necessary consequence of this mode of excretion of a vapour, that, if its exhalation by the breath could in any way be stopped, its narcotic effects ought to be much prolonged. The following experiments show that such is the case:--
Exp. 67.--About 750 cubic inches of oxygen gas were introduced into a balloon of thin membrane varnished with solution of Indian rubber in turpentine. The balloon was attached to one of the apertures of the spiral box which forms part of the ether inhaler I employ, and which was used for condensing the moisture in the experiments on alcohol previously detailed. Four ounces of solution of potassa were put into the inhaler, and to its other opening was attached a tube, connected with a face-piece without valves.* (*I used the same arrangement in giving oxygen gas last year, at the request of Dr. Wilson, to a cholera patient in St. George's Hospital. The patient, who was in a state of collapse, was not saved or relieved by it.) After inhaling as much chloroform as I could without being rendered unconscious, I immediately began to breathe the oxygen from and to the balloon, and over the solution of potassa. In this way the vapour exhaled in the breath had, the greater part of it, to be re-inspired. This process was continued for ten minutes, during which time the feeling of narcotism subsided very little, and it passed off very slowly afterwards, about half an hour elapsing before it was quite gone.
The oxygen was used, in this and the following experiments, to allow of respiration being continued for some time from the balloon without employing such an amount of air as would take up a great deal of the vapour. As there was air both in the lungs and inhaler at the beginning of the experiment, the oxygen was not breathed unmixed with nitrogen. The solution of caustic potash was employed for the purpose of absorbing the carbonic acid gas generated by respiration as the air passed to and fro over a large extent of its surface.
Exp. 68.--On another day the same quantity of oxygen and solution of potassa were employed, and fifteen minims of chloroform were placed in the spiral inhaler, in a small glass vessel, which prevented its mixing with the solution of potassa. I then began to breathe as in the former experiment, and continued to do so for fifteen minutes. The effects of the chloroform were gradually induced during the first three minutes, causing a considerable feeling of narcotism, but not producing unconsciousness. After the end of three minutes, the feeling of narcotism remained stationary till twelve minutes had elapsed, and during the last three minutes it very slightly diminished. The experiment was discontinued on account of a feeling of want of breath. It was half an hour longer before the effects of the chloroform were altogether removed.
Exp. 69.--The oxygen and solution of potassa were employed as before, and two and a half fluid drachms of ether were put into the inhaler, with the potash. The oxygen was breathed to and fro over the potash for twenty minutes. The effects of the ether were rapidly developed during the first three minutes, but not amounting to loss of consciousness. From this time, the influence of the ether remained nearly the same to the end of the experiment, and afterwards subsided very gradually.
The effects of the small quantity of chloroform and ether inhaled in these experiments would have passed off in three or four minutes, if the exhaled vapour had been allowed to diffuse itself in the air in the usual way.
The amount of carbonic acid absorbed by the potassa was determined, and will be given in the next communication, as it forms a separate branch of the inquiry into the action of narcotic vapours.
Return to John Snow Publications
Source: Snow, John. London Med. Gazette 46, 15 November 1850, pp. 834-835 [Letter to Ed.].
57. "Further remarks on the employment of chloroform by
thieves"
By John Snow, M.D.
In a former communication on this subject* I said, that if "thieves and prostitutes were to resort to the use of chloroform in the public streets, in the manner alleged, the attempt would only lead to their instant detection on the spot" (*Med. Gaz. Last volume, p. 327). This opinion has been more than confirmed by what has since occurred. In two or three cases in which it was alleged that robberies had been effected by means of chloroform, that part of the accusation which related to the use of this agent broke down on the cross-examination; whilst in two instances--the only ones, as I believe--in which it has been proved that chloroform was used with felonious intent, the culprit failed to induce insensibility, and was detected on the spot, although the attempt was not made in the street, but in a more secluded place. The first of these cases occurred in London, a few months ago. A young man returning after midnight with his sweetheart from a dance at a public-house, induced her to accompany him down a Mews or stable-yard. He there took out a bottle containing chloroform, and poured some of it on a han[d]kerchief, which he applied to the young woman's face. She tore away the handkerchief, and called out in such a manner as to bring a policeman from a neighbouring street to her assistance, who secured the offender, and picked up the bottle, which the latter had thrown away in his flight. The reader will probably remember that this case was amicably compromised, by the prisoner marrying the complainant, whilst he was remanded, and out on bail.
The other case, which happened recently, and is detailed in the Medical Gazette of yesterday, is of a more atrocious kind. A man who was lodging at an hotel in Kendal, secreted himself in the room of an elderly gentleman, whom he attacked in the middle of the night with a rag steeped in chloroform. The means used, so far from keeping the gentleman asleep, had a contrary effect; and although the robber struggled with his victim till blood was drawn by his violence, and the bedding had fallen on the floor in the scuffle, he did not succeed in making him insensible, or in preventing his bringing assistance by his cries.
It is quite true that the attempt, had insensibility been induced, might have resulted in murder; for the thief in the dark, and without experience to guide him, could not have known when to stop in time to spare life, if that were his intention. I therefore coincide in the remark in the leading article of the Medical Gazette of yesterday, respecting the insufficiency of eighteen months' imprisonment as a punishment for such a crime.
There may, however, have been circumstances which would have some weight with the Bench, and have not appeared in the newspapers.* (*Our information of the facts was derived not from a newspaper, but from private information from a respectable source. -Ed. Gaz.) I can easily suppose that it was the man's first attempt at robbery; for I cannot imagine that an experienced thief, or one who had the advantage of belonging to a gang, and therefore of consulting about, and trying beforehand, the means to be used, would on hearsay or newspaper evidence, have adopted the use of an agent so ill suited to assist him. Again, a chief object of punishment is to protect the public by preventing future crime; but in this instance the signal failure of the attempt at robbery will do more to deter others from using a like means than any example that could be made of the criminal. I think that this kind of attempt is not very likely to be repeated; and although chloroform is one of the thousand articles the use of which should be confined to medical men, yet the subject, in my opinion, is hardly of sufficient importance to require legislative interference. The murders by arsenic, in the rural districts, are a disgrace to the age and country in which we live, and have long and loudly called for a legal enactment to limit the sale of this poison: but if Parliament have to discuss what articles have to be admitted into the provisions of a "Sale of Poisons Restriction Bill," I am afraid that we shall be long in obtaining such an enactment; and if, when at last obtained, it be complicated by including too many substances, it will not work well.
The public have been greatly alarmed about the employment of chloroform by thieves, but what they really have to dread is, that robbers will still resort to the old means of the bludgeon, the pistol, and the knife, and not to one which allows the victim so good an opportunity to escape, and themselves so great a chance of detection. Every person who has inhaled chloroform must be quite aware that it could never have been given to him, in his sober senses, without his knowledge, even though every care were used to lessen the impression it makes, by beginning with the vapour largely diluted, and gradually increasing its strength; and no domestic animal, however tame, can be induced to take chloroform voluntary, but before being made insensible, or in the least affected by it, must always be in some way secured. Therefore, to use chloroform for the purpose of overcoming a person is to adopt a means that cannot be put in force till he is already overcome, and involves a difficulty just like that contained in the juvenile problem of catching a bird by applying a little salt to its tail.
[Editorial comment:] * * * Chloroform has been used in France for the perpetration of rape, and the offender tried and convicted. We hope Dr. Snow's prediction, that it cannot be used for robbery without the certainty of failure and detection, may not be proved wrong by experience.
Return to John Snow Publications
Source: Snow, John. Medical Times 22, 14 December 1850, p. 635, [Letter to Ed.].
58. "Dr. Snow on chloroform"
By John Snow, M.D.
Sir,--I shall be obliged if you will allow me space for a few observations in reply to some remarks in the Clinical Lecture of Mr. Bransby Cooper, reported in last week's Medical Times, respecting the effects of chloroform on a patient on whom he operated for the removal of a large tumour of the thigh. My object is merely to prevent mistaken impressions which might limit the application of the greatest boon that medical science has conferred on the present generation; and I feel confident that Mr. Cooper himself will be glad that I have given expression to my opinions, though they differ somewhat from his own. The operation in question did not appear to me to be a protracted one, but rather the reverse, considering its magnitude. The quantity of chloroform inhaled was between two and three fluid drachms. I have often been present at more protracted operations, at which a much greater amount of chloroform was consumed. The collapse, as Mr. Cooper terms it, undoubtedly arose from the loss of blood, and had no connexion with the chloroform. On a surgeon who stood near to me remarking on the faintness of the patient, I observed that it would have occurred without the chloroform, to which he fully assented; and I thought that such was the opinion of every one present, but have, it seems, been mistaken. I gave wine to the patient at the conclusion of the operation, certainly with no view of removing the effects of the chloroform, for I believe that these agents have a very similar action.
With respect to the loss of blood being small, if the term be used in comparison with what might be expected in such an operation, I can in some measure agree to it; but I consider that it was large compared with that which usually takes place in operations. Every one who has read the description of the operation will perceive that the hæmorrhage would be likely to be considerable, and, at all events, it was such as to tell very decidedly on the pulse and the colour of the lips. The fact of the hæmorrhage being chiefly venous, would not lessen its after effects, though it might diminish the danger at the moment. The large wound from the operation would also assist in keeping up the collapse; for, although chloroform usually leaves a soothing effect for some little time, the system begins to feel, more or less, the effects of any injury that it may have sustained as soon as the insensibility passes off. As for the reaction, which Mr. Cooper states did not take place in his patient till between ten and eleven at night, it was the reaction from the operation, none taking place from chloroform, as it is not required. I have seen a patient upwards of eighty years of age inhale six fluid drachms of chloroform for neuralgia in the course of the evening, and yet there was neither depression nor reaction from its use, the pulse being scarcely affected by it. The patient merely recovered from his insensibility after each inhalation. The only depression which I have seen produced by it, is that connected with a feeling of sickness which it sometimes occasions. That chloroform, when incautiously given, is capable of causing sudden death, must be freely admitted; but, used with due care, its effects quickly pass off; and under no circumstances is protracted collapse one of those effects. Its action, on the other hand, is rather that of a stimulant; a tincture of chloroform having been in use for many years, under the name of chloric ether, as a diffusible stimulant and antispasmodic.
All those who were in the Profession before the discovery of inhalation for causing insensibility to pain, must remember that syncope was by no means uncommon at operations, whilst now the reverse is the case; and in some hospitals where chloroform is constantly used, brandy, wine, and ammonia have altogether ceased to be kept in the operating theatres. Out of many hundred operations that I have witnessed under the influence of chloroform, I can only remember five in which spirits, [illegible word] ammonia were given on the operating table, and only two in addition to Mr. Cooper's case, in which there was severe and protracted collapse. In these two cases the operations were of unusual magnitude. I have, however, heard and read of operations performed years ago in which the patients died on the table, and that, occasionally, when neither the loss of blood nor the injury inflicted seemed adequate to cause such a result; and if, now and then, we still see great collapse following an operation, we ought, rather than blame the chloroform, to consider whether the event might not have been still more disastrous if the patient had had to suffer the pain of the operation.
Mr. Cooper describes the subsequent state of the patient as follows:--
"During the next two days her condition was very precarious. There was a quick, feeble, and at times fluttering pulse, dry and parched tongue, excessive thirst, hot and burning skin, frequent vomiting, and occasional rigors, attended with no salutary action whatever in the wound, which discharged a greenish exceedingly offensive, watery fluid. A favourable change, however, then took place."
Respecting these symptoms he says:--
"I have some little hesitation in speaking confidently or decidedly as to the true cause of her symptoms since the operation, namely, whether they were simply and purely the effect of loss of blood on an irritable subject, or whether they were the consequences of hæmorrhage modified by the influence of chloroform. I am disposed to incline to the latter however, for she certainly sustained but little loss of blood during the operation, and what she lost was chiefly venous; and, I must say, her condition has appeared to me rather to be produced by the influence of some poison, some irritating or abnormal constituent in the blood, than by the influence of hæmorrhage."
Now, any medicine may be called a poison when spoken of in a disparaging sense. Chloroform is a narcotic of the least irritating kind. In point of strength it is situated between opium and alcohol, but it differs from both of these agents in the short time which it remains in the blood. On the day subsequent to the operation, chloroform could only remain in the blood in almost infinitesimal quantity, whilst the opium, if not the alcohol, she had taken, would probably remain in comparatively much larger quantity. Experience, however, indicates that the symptoms (unless it were the single one of vomiting) could arise from none of these "poisons," and that, if due to a poison at all, they must have been caused by some of the morbid poisons which are apt to infest an hospital--such as that of erysipelas. The vomiting was most likely due either to the same cause as the other symptoms, or to the opium taken on the evening after the operation, but, whatever its cause, it was probably not injurious.-- I am, Sir, etc.,
54, Frith-street, Soho. John Snow.
Return to John Snow Publications
Source: Snow, John. London Jour. Med. 3, 1 February 1851, pp. 122-129.
59. "On the inhalation of various medicinal substances"
By John Snow, M.D.
The following are the chief reasons why it may be desirable to give medicines, in some instances, by Inhalation, in preference to the more ordinary method by deglutition.
1. As the influence of the medicine appears immediately, and a greater surface is offered for absorption, a larger dose may be given, and a more sudden and profound effect produced on the economy than it would be safe, or, in some cases, even possible to produce in any other manner. An instance in point is the insensibility induced by chloroform and ether.
2. The process of digestion is less interfered with, than by taking medicines into the stomach.
3. Many medicines which have a disagreeable taste--as turpentine, creasote, and camphor--are not unpleasant when inhaled in the form of vapour.
4. Agents, such as benzoic acid, and some of the gum-resins, which are believed to exert a local action on the mucous membrane of the air-passages, may be expected to have a greater effect when inhaled, than when they are taken into the stomach in the same doses, and reach the lungs only through the circulation.
5. Some agents, as chlorine and ammonia, have a local action when inhaled, which they could not exert if exhibited in any other way.
It was almost solely with a view to their local action that medicines were inhaled, prior to the discovery at Boston, in America, of etherization, which established a new era in inhalation; and even at the present time, with the exception of ether and chloroform, hardly any medicines are exhibited by inhalation, unless in affections of the lungs; although there evidently ought to be no such limitation of the practice.
It must be acknowledged in the outset, however, that it is a much less simple and easy matter to have medicines properly inhaled, than to direct them to be swallowed; and it is the object of the present communication rather to attempt the removal of difficulties, and to point out the physical conditions under which certain medicines can be inhaled, than to detail the results which have been obtained by inhalation.
Owing to neglect of the physical properties of a medicine, it has sometimes been supposed to be inhaled, when in fact it was not, unless in a quantity almost infinitesimal. It has not been unusual, for instance, to direct a drachm or two of tincture of hyoscyamus or conium to be put into half a pint or a pint of hot water, in order to be used for inhalation. Now the virtues of an infusion of these plants remain in the extract, after the water is all evaporated at a moderate temperature; and if the patient had inhaled day after day from the same water (having it made hot for the purpose), till it had all been consumed, the medicine would have been found at the bottom of the vessel in the form of an extract, to which water might have been added for the process to be commenced afresh. It is obvious, therefore, that any effects which have been produced by inhaling in this manner, were due either to the vapour of the water, which is very beneficial in irritable states of the mucous membrane, or to physical causes depending on the construction of the inhaler, and the mode in which it was used.
The most important of the additions to the mechanical means for inhalation, which followed the discovery of etherization, is the flexible face-piece, to include both the nostrils and mouth. Dr. Sibson introduced this, although Dr. Hawksley contrived a similar one about the same time. It is shewn in the engraving, which accompanies this paper, in the modified form in which I use it [see Fig. 2 in the engraving below]. The sides and margin, which form the flexible part, consist of thin sheet lead, lined with oiled silk, and covered with leather. The expiratory valve can be moved more or less to one side from the opening it covers, so as to admit unmedicated air, whenever the vapour feels too pungent. The advantages of a face-piece of this kind are, that it can be fitted to every variety of face; that the patient requires no instructions, having nothing to do but to continue breathing in his usual way, either by his mouth or nostrils, as he pleases; and that it imposes no labour on the respiratory muscles, for when applied to any suitable form of inhaler, it may be kept attached to the face for any length of time without fatigue. As I recommend the face-piece in every kind of inhalation (except where substances have to be drawn into the larynx in the form of powder, when a glass tube may be used), it has been described before treating of individual medicines, to which attention may now be directed.
I. INHALATION OF MEDICINES WITH THE AID OF HEAT.
A. IN THE DRY WAY. OPIUM, it is well known, is very extensively inhaled, in China and India, as an indulgence; but it has not been much used in this manner in the practice of medicine, so far as I am aware. I sought to ascertain the temperature at which the active ingredients of opium are given off, and whether the effects of the fumes are due to morphia, or to new products generated by the heat applied. For this purpose, I heated morphia and the meconate of this alkaloid in an oil bath, using a long narrow test-tube, on the recommendation of Dr. Bence Jones. I find that neither pure morphia nor the meconate are volatile, unless the heat be raised till they begin to be decomposed. This occurs at about 400º Fahr., when they become brown, and a brown sublimate begins to be condensed in the interior of the tube. The sublimate obtained from morphia is slightly reddened by nitric acid, but is not altered by the perchloride of iron. The sublimate from the meconate gave the same results, except on one occasion, when some minute colourless crystals were sublimated from it, at a temperature of from 380º to 400º. These were rendered of a deep red by nitric acid, and were reddened also by the perchloride of iron. We may conclude, therefore, that the effects produced by the inhalation of opium are chiefly, if not altogether, due to the generation of new products by the heat applied.
For the inhalation of opium, the Chinese use a pipe of a peculiar construction, which they heat over a spirit lamp. The preparation which they use is the watery extract, and the quantity employed at one time is said to be a piece about the size of a pea; but whether the dose requires to be increased with the habit of using it, as happens when opium is taken into the stomach, I have not been able to learn. The Chinese opium-pipe is too complicated for general use by patients, and anything in the form of a pipe would be liable to misuses ; as Europeans, with the exception of the Turks, use a pipe merely to draw the air into the mouth and puff it out again, instead of inhaling with it, as I believe is the practice in all eastern nations. I have therefore contrived an inhaler, which is adapted for a greater number of other medicines as well as opium. (Fig. 1)
It is made chiefly of tin, and consists of cylindrical chamber, between four and five inches in diameter, and three or four inches deep, under the centre of which a spirit lamp is placed. The bottom of the inhaler consists of a thin piece of talc, on which is placed a small capsule of Berlin-ware, for the purpose of holding the extract of opium. A porcelain funnel-holder, which is placed on the talc, keeps the capsule exactly over the flame of the lamp. The talc allows sufficient heat to be transmitted to the opium, without conducting it to the sides of the inhaler, and, consequently, the air which is inhaled is not unduly heated. The lid of the inhaler is moveable; it is provided with a delicately balanced valve for the admission of air, and is connected with the face-piece before mentioned, by means of an elastic tube of wide calibre, as shewn in the engraving.1 (1The Inhalers are made by Matthews, Portugal Street.)
The extract of opium, in the form of a pill, is placed in the capsule without any addition, and the spirit-lamp is lighted beneath it with a very small flame, which may be increased if requisite. The patient begins to inhale immediately the lamp is lighted, and continues to do so as long as anything is given off. The moisture contained in the extract is first expelled by the heat and inhaled, then follow the active principles of the opium, accompanied, after a time, with some smoke, and nothing is left but a porous carbonized mass. The process, being conducted slowly, usually lasts about ten minutes. If the volatile products be too irritating at any time, and excite coughing, the spirit-lamp should be removed for a minute, the inhalation being continued, however, in the mean time. The patient learns very soon to accommodate the process to his tolerance of the vapour, the pungency of which is very slight.
At the Hospital for Consumption at Brompton, the physicians to which institution kindly invited me to assist in contriving and super-intending the inhalation of medicines, a considerable number of patients have inhaled opium during the last twenty months,--some of them having inhaled every evening for several weeks in succession, and discontinued only on leaving the hospital. Three or four of the patients had emphysema with chronic bronchitis; but the majority had phthisis, with cavities in the lungs--cases, in which the cough was more than usually troublesome, being generally chosen. The cough was relieved by the inhalation in the greater number of cases, and many of the patients increased in weight, and improved considerably in general health. Other remedies were used at the same time, and contributed to the improvement, but it seemed to be in part due to the inhalation. It has caused constipation of the bowels in only two or three of the patients; I have, however, experienced that effect when I have inhaled it for experiment. The quantity of watery extract of opium inhaled at one time has generally been two grains; but, in a few cases, three grains have been used. Crude opium was used in one case, instead of the watery extract; but the fumes it gives off are more irritating to the bronchial membrane, than those from the latter agent.
Morphia is, in my opinion, the most suitable preparation of opium for inhalation; but I have not recommended it at the Bromptom Hospital, on account of its expense. It has, however, been inhaled by one patient, in the dose of half a grain, and I have inhaled it in the same quantity. It is much easier and pleasanter to inhale than the extract of opium, the extractive matter of which supplies some smoke, which is probably quite inert. It is of service to mix the morphia with a little dry plaster of Paris, to give it more weight and bulk.
With respect to the doses just mentioned, it should here be remarked that a medicine, when inhaled, cannot be all absorbed, as usually happens when it is taken into the stomach, for only part of it reaches the lungs, whilst another part is expired again with the air which has occupied the nostrils or mouth, the larynx, trachea, and larger bronchi. I am inclined to believe that about one-half of what is inhaled is usually absorbed; for on inhaling air charged with vapour of chloroform from a bladder or small balloon, I experienced as much effect from ten minims, when it was breathed backwards and forwards for a minute or two, as from twenty minims, when the air was breathed only once.
EXTRACT OF STRAMONIUM has been inhaled in the Brompton Hospital, with more or less relief, by five or six patients affected with asthma. Four grains were used, in the same manner as opium. The spirituous extract of aconite was used also by one patient, in the quantity of a grain; and it is probable that other extracts might be employed with advantage, in the same manner.
GUM-RESINS. The fumes given off by these medicines may be inhaled in the same way as opium; but, as these fumes are pungent when in large quantity, it is advisable to powder two or three grains of the gum-resin, and mix it with about ten times as much of some inert powder, as gypsum, before exposing it to heat in the capsule. Used in this way, ammoniacum gives off a very fragrant odour, and, though rather pungent, can be inhaled very well by most persons. With steam the gum-resins can be easily inhaled, as the quantity of vapour which they give off, at the temperature of boiling water, is small. In this way, however, the patient gets no great amount of the medicine; but probably enough to exert some local action.
B. WITH VAPOUR OF WATER. For the inhalation of medicines along with the vapour of water, I employ the above-described inhaler, using a somewhat larger earthenware capsule than for inhalation in the dry way. Into this capsule or dish, about half an ounce of water is put, together with the medicine to be inhaled. The water is heated by the spirit-lamp, sometimes till it boils gently, but generally to a point rather short of boiling. This quantity of water yields as much vapour as a patient can conveniently breathe in about half an hour; and a much greater amount of the medicine can generally be inhaled than if it were placed in a larger quantity of water. In the case of some substances, indeed, as iodine, oil of turpentine, and camphor, which are particularly adapted for inhalation in this manner, the medicine is all inhaled before the water is finished.
IODINE may be most conveniently inhaled, by adding a small quantity of a strong spirituous solution of it to half an ounce of water. Twelve minims of the iodine tincture of the Dublin Pharmacopæia, containing one grain of iodine, are a suitable dose. The advantage of adding the iodine in the form of tincture is, that it becomes equally diffused through the water. As the patient inhales, the water becomes less and less deep in colour, and by the time that he has inhaled about three-fourths of the water, he has inhaled the whole of the Iodine; and the remaining water is colourless. On account of its irritating effects on the stomach, it would probably be advisable that iodine should be given by inhalation, in every case in which its exhibition is required. Allusion is here made only to iodine, and not to the iodide of potassium, which, not being volatile at the heat of boiling water cannot be inhaled in this manner. I very much doubt whether phthisis be one of the diseases to be benefited by iodine. It was inhaled by eighteen patients at Brompton, in the summer of 1849, and the following autumn and winter; they generally commenced with half a grain, and it was increased, in one or two cases, to two grains; but the usual dose was a grain once a day. In two or three cases it was discontinued, as it seemed to increase the cough, and one or two of the patients complained of head-ache from its use. It was continued, however, for more than a month, in ten of the cases; and I was present on nearly every occasion, to see it inhaled. It may consequently be said to have had a fair trial; but no benefit could be observed to follow its use. It was not inhaled as above recommended, but from a Woulfe's bottle, over the interior of which its spirituous solution was diffused; no artificial heat or vapour of water was employed; the inhalation was continued till the iodine had disappeared. There were consequently no extraneous circumstances to interfere with its action.
OIL OF TURPENTINE has been inhaled in a few cases, by putting twenty drops of it, with about half an ounce of water, into the capsule; the spirit-lamp being placed underneath, as usual. The boiling point of oil of turpentine is much higher than that of water; but owing to the great density of its vapour, as compared with steam, it evaporates more quickly than water, as happens with iodine, and consequently it is all inhaled before the water is consumed. The cough has appeared to be relieved in the cases in which it was used. One was case of hæmoptysis, which subsided under its use, as, however, it might have done without it.
CAMPHOR can be conveniently inhaled by putting thirty or forty drops of the tincture into half an ounce of water. It is usually consumed as soon as the water with which it is mixed. It has appeared to relieve the cough, in a few cases in which it has been used.
BENZOIC ACID can be inhaled with the vapour of water. If six grains be put into half an ounce of water, the patient will inhale about half of it, and should leave off before the water is quite dried up, to avoid the pungent fumes which would otherwise arise. For the next inhalation, some water and about three grains more of benzoic acid can be added to that which remained. I have not seen sufficient of its employment to speak of its effects.
CREASOTE may be best inhaled in the same manner. If not more than about four drops be put into the half ounce of water, all of it will be inhaled. I have generally given creasote, however, with the inhaler marked number 2 in the engraving. Several patients have inhaled it at the Brompton Hospital, generally using three or four drops twice a-day. The benefit from its use has not been very great, but might probably have been greater, if it had been inhaled with vapour of water, which itself is serviceable.
II. INHALATION OF MEDICINES AT THE ORDINARY TEMPERATURE.
The smaller inhaler, shewn in the engraving, was contrived for the inhalation of chloroform in medical and obstetric cases [see Fig. 2]. It is made of brass tube, rather less than an inch in diameter, and is lined with bibulous paper to absorb what is put in, and afterwards yield it up in the form of vapour as the patient inhales. It is adapted by a screw to a face-piece similar to that employed with the other inhaler. It is not my intention to speak of chloroform on the present occasion. Amongst the other medicines which have been inhaled with it, are hydrocyanic acid and conia; and it is adapted for the inhalation of almost any agent that does not require the application of heat.
HYDROCYANIC ACID has been inhaled by several patients at the Brompton Hospital, but it has not seemed to produce any good effects which would not have resulted from its use by deglutition. The quantity inhaled was generally twice as much as one would give by the stomach, and it was somewhat diluted with water, to diminish the pungency of the vapour, and enable the nurse to measure the quantity more easily in the minim glass.
CONIA, the volatile alkaloid of spotted hemlock, has been inhaled by several patients. Some of this active principle having been kindly given to me by Mr. Morson, I first tried small doses on myself, and found that a minim of it could be inhaled without inconvenience. This was the quantity usually administered, although two minims were inhaled in a few cases. Dizziness was caused by it in many instances, especially when the larger dose was employed, but this effect subsided in less than an hour. The cough was usually relieved by it, and in two or three cases of asthma, the breathing was also relieved. The conia was diluted with nine parts of spirit, both for convenience in giving the right dose, and in order that it might be better diffused over the paper in the inhaler, and offer a larger surface for evaporation.
The following experiment, performed in 1848, on the inhalation of conia, may not be uninteresting, as shewing that this is one of the agents which might be employed for the prevention of pain in operations.
A chaffinch was placed in a covered glass jar, holding 100 cubic inches, and one grain of conia was put in. The bird seemed unaffected for ten minutes, and the jar was opened with the intention of trying a larger dose; a minute afterwards, however, it fell on its side and lay, not relaxed, but like a stuffed bird, as its head did not droop. It moved its legs, now and then, by convulsive starts. It was insensible to pricking and pinching, although, from the appearance and motion of its eyes, it seemed to be conscious all the time. It recovered its sensibility in about two minutes, but was not able to stand for ten minutes. It afterwards appeared well.
In a guinea-pig, in which the inhalation was continued till a fatal effect was produced, violent convulsions occurred before death, and the heart remained irritable afterwards.
AMMONIA has been inhaled with great relief in a few cases, in which more or less bronchitis, with difficulty of expectoration, existed. The inhaler employed was similar to that described by Mr. Smee in the Medical Gazette for 1843, except that an elastic tube and face-piece were attached to it. It consists of a Woulfe's bottle with wide apertures, and a tube for the entrance of air, descending a certain way, but not dipping into the solution employed. The ammonia was given weaker than by Mr. Smee. Two ounces or so of cold water remained constantly in the bottle; and when it was about to be used, twenty minims of strong solution of ammonia were added, and the patient inhaled for half an hour, or as long as ammonia continued to be given off. The inhalation was repeated twice or three times a day.
It may be remarked, that either ammonia or hydrocyanic acid might be inhaled, along with vapour of water, in the opium-inhaler first described; so that a person provided with it might apply it in almost every kind of inhalation.
CHLORINE has been inhaled by a few patients, in different stages of phthisis, but with no advantage, although it was continued by some of them for a few weeks. To obtain it, some chloride of lime was put into the Woulfe's bottle-inhaler, just mentioned, and moistened with a little water. When it was wished to increase the quantity of chlorine beyond the small amount spontaneously given off, the inspiratory valve of the face-piece was prevented from closing completely, and a little of the expired air being thus allowed to get into the bottle, the carbonic acid it contained acted on the lime, and caused chlorine to be liberated.
It will be observed, that the medicines mentioned above have all been recommended to be inhaled, either alone, or with the vapour of water: and, as a general rule, it is better for medicines to be inhaled singly; since no two being equally volatile, they could not be inhaled if combined, in the proportions in which they might be mixed. The method of administering medicines by inhalation also being yet as it were, in its infancy, the exhibition of one at a time is better adapted for the collection of correct observations respecting their effects.
54, Frith-street, Soho, January 2, 1851.
Return to John Snow Publications
Source: Snow, John. Wilson and Ogilvy, 57 Skinner Street, Snowhill, London, 5 March 1851 [an open letter published as a pamphlet].
60. "A Letter to the Right Honourable Lord Campbell, Lord Chief Justice of the Court of Queen's Bench, on the Clause Respecting Chloroform in the Proposed 'Prevention of Offences Bill.' "
By John Snow, M.D.
(5 March 1851)This open letter, published as a pamphlet, is internally dated March 5, 1851.
Licentiate of the Royal College of Physicians; author of On the Inhalation of Ether in Surgical Operations.
My Lord,
More than four years have elapsed since a discovery was made in a great nation, descended, though now separated, from our own--a discovery, which, from the benefits it has conferred on humanity, is second only to that made by Jenner, in this country, nearly half a century ago. Your Lordship must be aware that I allude to the inhalation of Ether, for the prevention of pain, discovered by Dr. Jackson and Mr. Morton of Boston, in America. No acknowledgment has been made to these gentlemen by this kingdom, or its government, and perhaps the consciousness of having conferred a great benefit on mankind is its own sufficient reward: but it would be truly unfortunate if the first notice of this great discovery by the British Legislature should be in a new penal law for crimes supposed to be committed through the means which it supplies,even though, the law should not point to Sulphuric Ether itself, but to that medicine which, on account of certain slight advantages, has, in a great measure, superceded it.
The prominent mention of Chloroform, in the fourth clause of the Bill presented by your Lordship to the House of Lords, on the 24th ult. [February], is to be regretted on other grounds. It ill becomes the gravity of the law, and is, I feel assured, far from your Lordship’s intention, that a legal enactment should be made on a false alarm, or to meet a trivial and unsuccessful innovation in the mode of attempting a crime: to legislate on this matter would revive the groundless fears of the public, which have subsided, or been allayed; and might even cause evil-disposed persons to make trial of a means, which they would conclude to be not without efficiency, when it had given rise to a law for its suppression. There is no reason to believe that Chloroform has been employed in more than two instances with criminal intent; and so far from aiding the perpetration of crime, it has led to the immediate detection of the offender, on both occasions. The knowledge of these two cases is more calculated to deter from similar attempts, than any increase of the punishment, which a culprit might expect to escape altogether, by avoiding detection.
When administered gradually, Chloroform can be breathed easily enough, by a person willing and anxious to take it; but he has to draw his breath many times before he becomes unconscious. During all this interval he has a perfect perception of the impression of the vapour on his nose, mouth, and throat, as well as of other sensations which it causes; and every person who has inhaled Chloroform retains a perfect recollection of these impressions and sensations. If Chloroform be given to a child whilst asleep, the child awakes, in nearly every instance, before being made insensible, however gently the vapour may be insinuated. No animal, either wild or tame, can be made insensible, without being first secured; the Chloroform may, it is true, be suddenly applied on a handkerchief to the nose of an animal, but the creature turns its head aside, or runs away, without breathing any of the vapour. If a handkerchief, wetted with sufficient Chloroform to cause insensibility, is suddenly applied close to a person's face, the pungency of the vapour is so great as immediately to interrupt the breathing, and the individual could not inhale it, even if he should wish. From all these facts it is evident that Chloroform cannot he given to a person in his sober senses, without his knowledge and full consent, except by main force. It is certain, therefore, that this agent cannot be employed in a public street or thoroughfare; and as the force that would required to make a person take it against his will, would be more than sufficient to effect a robbery, and enough to effect any other felony, by ordinary means, it would afford no help to the criminal, in more secluded situations. Supposing that the felon or felons could succeed in keeping a handkerchief closely applied to the face, the person attacked would only begin to inhale the Chloroform when thoroughly exhausted by resistance or want of breath, and when, in fact, the culprits could effect their purpose without it.
Many people who read brief and imperfect accounts of the exhibition of Chloroform on a handkerchief, soon after its introduction into use, formed the opinion that it was capable of being employed to cause stupefaction, for felonious purposes. After a time, persons who fell down in a fit, and others who were overtaken by the effects of drink, whilst in disreputable company, were reported to have been the victims of Chloroform; but the first cases which, as far as I am aware, came in a definite form before a Court of Justice, occurred at the beginning of last year, and require a brief notice.
On January 10th, [1850] a robbery was committed in Thrall Street, Spitalfields, for which two women, named respectively Elizabeth Smith and Margaret Higgins, were examined three or four times at Worship Street, tried at the Central Criminal Court on February 8th, convicted and sentenced to be transported for fifteen years. The following is the evidence given by the prosecutor, at one of the examinations before Mr. Hamill. He was proceeding along the Whitechapel Road, between 9 and 10 o'clock in the evening, "when he felt some one, whom he believed to be a woman, touch his left side, and at the same time felt a rag or handkerchief pressed over the lower part of his face. He instantly became insensible, and was conscious of nothing that occurred to him, until about day-light the following morning, when he slowly revived, and upon recovering sufficiently, found himself lying in a very dirty bed, in a wretched apartment."* (*Times, 25 January 1850.)
It will be observed by your Lordship that the witness gives no account of either the local or general sensations which Chloroform causes. He felt a handkerchief or rag applied to his face, and instantly became insensible. This circumstance alone indicates that Chloroform was not the agent employed. But there are other reasons which prove the view I entertain of the matter. Whitechapel Road is a very busy thoroughfare between 9 and 10 in the evening, and admitting that a gentleman could be made insensible in the instantaneous manner alleged, without the opportunity of making the least resistance, or calling for assistance, it is impossible that he could be dragged, or otherwise conveyed, in that state to another street, without attracting the attention of passers by, and even causing the collection of such a crowd as would ensure the interference of the Police. As the effects of Chloroform subside very rapidly when quickly induced, the dose would, moreover, require to be repeated, before the victim could be conveyed a distance of two or three hundred yards.
If the transaction occurred at the time and place alleged, the prosecutor, however insensible he might be, must have appeared to accompany the woman voluntarily; but I know no drug which can be administered on a handkerchief to produce effects of this kind, and am inclined to believe that the agent which could cause such results must be more subtle than anything that can be contained in an apothecary's phial. Whether it was witchcraft, animal magnetism, or some other invisible kind of attraction, I shall not attempt to decide.
The long continuance of the insensibility (ten hours) in this case, shows that it was not caused by Chloroform, the effects of which pass off in a few minutes, or, at the longest, in half an hour; and this remark applies to every substance that will quickly cause insensibility, when breathed from a handkerchief; for the volatility which enables it to be taken in this way, causes its ready elimination from the blood, in its passage through the lungs. It must concluded, therefore, that the insensibility, in this instance, was caused by something which had been swallowed. Laudanum, ardent spirits, and fermented liquors, are articles which are capable, amongst others, of causing prolonged stupor, but there are no means of ascertaining now what might have been used.
After the examination of the prisoners in this case had been two or three times adjourned, a woman came forward and gave evidence that, on an occasion previous to the robbery, the prisoner Higgins "had told her that a man named Gallagher, with whom she cohabited, had undergone an operation at the London Hospital, they had given him some stuff to send him to sleep, and that he had contrived to bring some of it away with him from that institution."* (*Times, 25 January 1850.) The medical officers of the London Hospital have no knowledge of any Chloroform having been taken away by a patient, and it must occur to your Lordship that the statement of a person who alleged that she had been in the confidence of the thief, and had kept her unlawful secrets for a long time, carries with it no great weight.
Whilst the alleged action of Chloroform in the above instance was too instantaneous, in the other case of alleged robbery by means of this agent its reputed action was so long deferred as to prove clearly that it proceeded from a different cause.
Charlotte Wilson was tried at the Surrey Adjourned Sessions, on February 9th, 1850, for a robbery committed on a man in the beginning of the previous month. The prosecutor stated that he was walking along the Borough, towards London Bridge, when he was accosted by the prisoner, who passed a handkerchief across his face, and he became very unwell. Not suspecting that any narcotic was contained in the handkerchief, (a circumstance which alone is sufficient to prove that no Chloroform was used), he ran into a public house hard by, and called for a glass of brandy. A Police constable stated that he saw the prisoner accost the prosecutor, and pass something across his face. He then saw them enter the public-house, when he saw the woman drinking with the prosecutor. About ten minutes afterwards he saw the prisoner run out of the house with a hat and scarf. The prosecutor was at that time insensible.
The effects of Chloroform are induced whilst a person is breathing it, and attain their greatest intensity within twenty seconds after the inhalation has ceased; it is consequently impossible for a person to go into a public-house, and be seen drinking there, between the time of taking the Chloroform and the insensibility induced by it.
The man was a considerable time before he recovered his senses; another circumstance which proves that the stupor had not been caused by Chloroform.
A non-medical witness, who gave evidence before the Magistrate, was confident that the stupor or insensibility was not caused by liquor, but by some deleterious article such as Chloroform. The Court and Jury who tried the prisoner were of the same opinion, and she was sentenced to be transported for ten years, although a student from any hospital in London could have informed the Court that Chloroform had not been employed.
The landlord of the public-house in which the robbery was committed, said that the prosecutor appeared to be in liquor when he entered. This evidence may be safely received; for a publican could not be deficient in experience on this point, and could hardly be influenced by prejudices that would lead him to consider a customer intoxicated who was not so. This evidence admitted, the case is perfectly clear; for nothing is more common, when a person in liquor goes on drinking, than for him shortly afterwards to be lying insensible.
Some remarks of mine on the two cases just alluded to appeared, soon after their occurrence, in the Medical Gazette,and were quoted by the Times newspaper. Two or three robberies were afterwards committed in which Chloroform was alleged to have been used, but the Counsel ridiculed the idea, and the part of the cases having reference to Chloroform broke down on a cross-examination. There have been, however, two cases, in which it was attempted to administer this article with felonious intent; and to these it is necessary to refer.
On April 30, 1850, a young man, named Charles Jobling, was placed at the bar, before Mr. Broughton, at the Marylebone Police Court, charged with having attempted to administer Chloroform, with intent to violate a young woman, to whom he had been paying his addresses for nine months. It was proved that whilst returning from a concert at a public house, about one o'clock the same morning, the prisoner induced the complainant to accompany him down a yard, when he uncorked a phial, poured the contents on a handkerchief, and applied the latter to her face. She immediately pulled away the handkerchief, and called out so loudly that she obtained the assistance of a policeman from the neighbouring street, who took her assailant into custody. When asked by the Magistrate if she felt any ill effect from the application of the handkerchief, the complainant replied as follows: "I did not, your Worship, as I pulled it away from my face instantly, it was completely saturated with wet, and had a remarkably strong smell."
The prisoner was remanded, and bail was accepted for his appearance on a future day. During this interval he married the young woman, and at the next examination she begged for his discharge. After a further remand, and a severe lecture, the worthy Magistrate reluctantly surrendered the prisoner to his wife who, if she does not remain of the same forgiving disposition, doubtless finds means of punishment as severe as any which the law had in store for him.
The other instance of felonious attempt to administer Chloroform was of a more serious character; but it equally illustrates the inapplicability of this medicine in aiding the plans of a criminal.
In October last, a man named Charles Venn contrived to secrete himself under a bed, in an hotel at Kendal, and attempted to give Chloroform, at midnight, to an elderly gentleman in his sleep. The effect of this attempt was to awake the gentleman; and although the robber used such violence that the night-dress of his victim was covered with blood, and the bedding fell on the floor in the scuffle, he did not succeed in his purpose. The people in the house were disturbed, and he was taken into custody, and ultimately sentenced at the Westmoreland Michaelmas Session, to eighteen months' imprisonment with hard labour, including one month's solitary confinement.
A crime was committed in France on a person under the influence of Chloroform, but not by the agency of that article. The Chloroform was voluntarily inhaled by a female, for the lawful purpose of having a tooth drawn without pain, and the dentist took advantage of the stupor so induced, as he might have done of a fainting fit, or any other kind of insensibility, to effect violation. The clause in your Lordship's Act, being directed against the application of stupifying drugs with criminal intent, would not apply to such a case, nor is it necessary to frame a law for the purpose: for should such a crime unhappily be perpetrated in this country, it could be dealt with by existing laws, as it has been in France.
I trust that I have said sufficient to induce your Lordship to consider whether it would not he advisable to withdraw the word Chloroform, the presence of which can only be alarming to the public, suggestive to the criminal, and little creditable to the sagacity and gravity of the law; whilst its removal would not affect the operation of the Act, even in a case, should such a one again recur, in which it might be foolishly attempted to exhibit the article.
In conclusion, I will venture to make a few additional remarks on the operation of the fourth clause of the bill presented by your Lordship.*
(* The clause runs as follows. "And whereas it is expedient to make further provision for the punishment of persons using Chloroform, or other stupifying things, in order the better to enable them to commit felonies: be it enacted, that if any person shall unlawfully apply or administer, to any other person, any Chloroform, Laudanum, or other stupifying or overpowering drug, matter, or thing, with intent thereby to enable such offender or any other person to commit any felony upon the person to whom the same may be applied or administered, or attempted to be applied or administered, or upon his or any other person's property, every such offender shall be guilty of felony, and being convicted thereof shall be liable, at the discretion of the Court, to be transported for life, or for any term not less than seven years.")
All the dietetic and medicinal, as well as other narcotics, are capable of causing stupor when taken in sufficient quantity. The stupifying or overpowering matters in most frequent use in this country, are ardent spirits, wine, and beer. I conclude that the clause under consideration does not apply to spirituous and fermented liquors, when openly given, with whatever intent, but to the fraudulent administration of other substances, similar in action, but more powerful. It cannot be denied that opiates are sometimes exhibited, with felonious intent, in malt liquor, the bitterness of which disguises their taste, and such a crime cannot be too severely punished; but it would he a great error to conclude that the offence called hocussing is so common as the statements of prosecutors at the Police Courts would imply. Persons who have been dead drunk are very unwilling to admit, even to themselves, that the result was the consequence of their own voluntary potations, and still less willing to admit it to the world, when they have to complain of having been robbed whilst in bad company. Therefore, before such evidence is received as conclusive, it should be confirmed by chemical analysis, or in some way; otherwise errors may occur, such as that at the Surrey Adjourned Sessions, alluded to above.
The rapid supervention of stupor ought not to be accepted as proof that it was not occasioned by spirituous or fermented liquors, for these articles sometimes produce their effects with great velocity. Ardent spirits, indeed, under some circumstances, act with greater rapidity than almost any thing else except Prussic Acid, and on some occasions are not even surpassed by that poison. In the instance of a child lately killed by gin, for administering which, a woman named Maria Ewens is now awaiting her trial, the little girl was carried out of the woman's room in a state of insensibility, a few minutes after she entered; and there are cases on record in which a man has dropped down insensible the instant after swallowing a large draught of ardent spirits.
At the trial of Johannah Driscoll at the Central Criminal Court in December last [1850], for a robbery committed in a house of ill fame, it was alleged that Chloroform might have been put into some gin taken by the prosecutor. Chloroform, however, although very soluble in rectified spirit of wine, does not mix easily with potable spirits, and when dissolved imparts to them such a very hot and sweet taste, that no one could take them without being aware of the adulteration. It would, moreover, be very difficult to make a person insensible by giving such a solution of Chloroform as a drink, even were he disposed to take it.
I have the honour to be, My Lord,
Your obedient Servant,
John Snow, M.D.
54, Frith Street, Soho,
March 5, 1851.
THE END.
[printed by] Wilson [and] Ogilvy, 57 Skinner Street, Snowhill, London
Go to Group 5 (# 61-74)
Click to return to Stream 1 - d: John Snow's Publications
Click to continue to Stream 1 - e: Memoir of his friend Benjamin Ward Richardson
 (#46-60)
(#46-60) Return to John Snow Publications
Return to John Snow Publications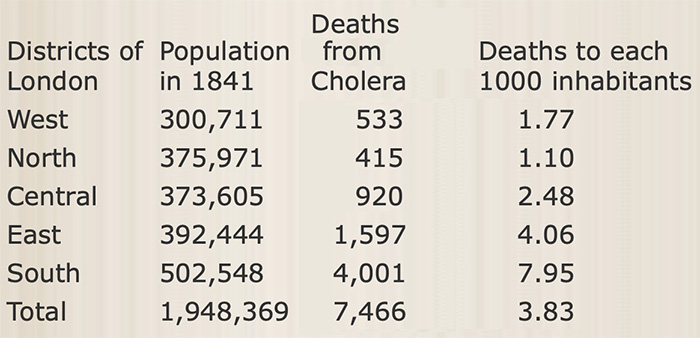
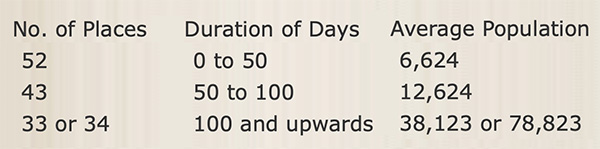
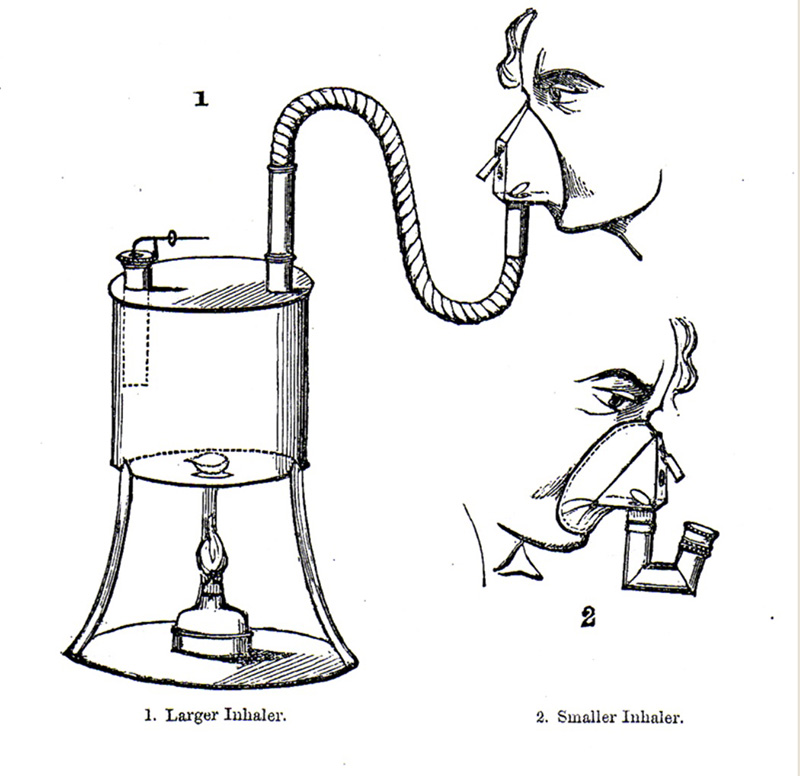
 (# 61-74)
(# 61-74)
